Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Confined Space - Generic - Rescue Plan TemplateDocument10 pagesConfined Space - Generic - Rescue Plan TemplateNick Shelley100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- DHS Tactical EMS Guide PDFDocument204 pagesDHS Tactical EMS Guide PDFxose lois Lopez100% (2)
- Thyroid Cancer Care Collaborative: A Computerized Clinical Decision Support System For Management of Thyroid NodulesDocument22 pagesThyroid Cancer Care Collaborative: A Computerized Clinical Decision Support System For Management of Thyroid NodulesJoko WowNo ratings yet
- Register Pasien Bedah Onkologi 28 April 2019Document2 pagesRegister Pasien Bedah Onkologi 28 April 2019Joko WowNo ratings yet
- Perioperative Pain Management - Bali 2019Document55 pagesPerioperative Pain Management - Bali 2019Joko WowNo ratings yet
- REGISTER PASIEN BEDAH DIGESTIF 4 Nov 2018Document4 pagesREGISTER PASIEN BEDAH DIGESTIF 4 Nov 2018Joko WowNo ratings yet
- Mdy095 PDFDocument11 pagesMdy095 PDFJoko WowNo ratings yet
- Laporan Jaga Bangsal Hari Jumat, 19 October 2018Document8 pagesLaporan Jaga Bangsal Hari Jumat, 19 October 2018Joko WowNo ratings yet
- Manualspindle HSDDocument183 pagesManualspindle HSDMario DuranNo ratings yet
- Salter Chapter 5: Preceptor of Module Dr. Hermansyah, SpotDocument37 pagesSalter Chapter 5: Preceptor of Module Dr. Hermansyah, SpotKahfi Rakhmadian KiraNo ratings yet
- Head and Neck MnemonicsDocument8 pagesHead and Neck MnemonicsTONY GO AWAY100% (1)
- Teacher's Answers - The Passive VoiceDocument5 pagesTeacher's Answers - The Passive VoiceMichelle100% (1)
- Eloquent: InformalDocument93 pagesEloquent: InformalRahulJakharNo ratings yet
- Tibia VaraDocument13 pagesTibia VaraRafael Lima LopesNo ratings yet
- Asda-A2 M en 20100429Document517 pagesAsda-A2 M en 20100429Mario Plinio CrivelliNo ratings yet
- (Ebook - Martial-Arts) Pressure Points - Military Hand To Ha PDFDocument27 pages(Ebook - Martial-Arts) Pressure Points - Military Hand To Ha PDFDragos-Cristian FinaruNo ratings yet
- Multi OrganDocument10 pagesMulti OrganthyinkslingerNo ratings yet
- MFL 70404801 20200811Document120 pagesMFL 70404801 20200811رحيق الجنةNo ratings yet
- Impaired Skin IntegrityDocument2 pagesImpaired Skin IntegrityBesael Baccol100% (1)
- Narrative On Rodney KingDocument2 pagesNarrative On Rodney Kingapi-316918731No ratings yet
- Introduction of Online Basic First Aid Course - For Circulation April 2021Document39 pagesIntroduction of Online Basic First Aid Course - For Circulation April 2021Yuwaraj NaiduNo ratings yet
- Basic Concepts in BiomechanicsDocument20 pagesBasic Concepts in Biomechanicsmuhammad kaleemNo ratings yet
- Eighth Division: Court of AppealsDocument18 pagesEighth Division: Court of AppealsBar2012No ratings yet
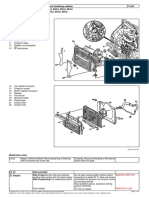
- Removing and Installing RadiatorDocument2 pagesRemoving and Installing RadiatorAnonymous d8ermLyF3No ratings yet
- List of Incidents at Walt Disney World - WikipediaDocument1 pageList of Incidents at Walt Disney World - WikipediaDanna MirandaNo ratings yet
- AdairDocument13 pagesAdairPhilippe RomanskiNo ratings yet
- Climb Injury Free Compressed Book SampleDocument52 pagesClimb Injury Free Compressed Book SampleColegio MontahueNo ratings yet
- Mri - Lumbar SpineDocument7 pagesMri - Lumbar SpineJEET GHOSHNo ratings yet
- TracheaDocument12 pagesTracheaShimmering MoonNo ratings yet
- Compartment SyndromeDocument25 pagesCompartment SyndromeestyjayantiNo ratings yet
- Difference Between Sprain and StrainDocument4 pagesDifference Between Sprain and StrainTayyab AliNo ratings yet
- Istezanje Nakon SpavanjaDocument6 pagesIstezanje Nakon SpavanjaLaza UrosevicNo ratings yet
- 3D CAFE Modelling of Transitional Ductile - Brittle Fracture in SteelsDocument141 pages3D CAFE Modelling of Transitional Ductile - Brittle Fracture in SteelsCatalin PruncuNo ratings yet
- Tumble Action Washer: Use & Care GuideDocument11 pagesTumble Action Washer: Use & Care GuidetheussatNo ratings yet
- S2 Tibial NailDocument32 pagesS2 Tibial NailAloexandru All IonNo ratings yet
- Question Paper and Answer Key For RUHS Medical Officers Recruitment Examination - 2015Document17 pagesQuestion Paper and Answer Key For RUHS Medical Officers Recruitment Examination - 2015Mayanka SaxenaNo ratings yet