Download as pdf or txt
You might also like
- Orange Juice SongbookDocument60 pagesOrange Juice SongbookLewis BlossNo ratings yet
- Clinical Microbiology Laboratory Test RequisitionDocument1 pageClinical Microbiology Laboratory Test RequisitionRhodjane Dela Cruz0% (1)
- CMP Final Draft FuelDocument33 pagesCMP Final Draft Fuelapi-594648232No ratings yet
- Ocean Acidification PPDocument17 pagesOcean Acidification PParpita laxmanNo ratings yet
- 3.6.5 SOP - Sputum CultureDocument3 pages3.6.5 SOP - Sputum CultureSemeeeJunior50% (2)
- Work Method Statement For Directional DrillingDocument3 pagesWork Method Statement For Directional Drillingnice hossainNo ratings yet
- Lab 9. Sample CollectionDocument23 pagesLab 9. Sample CollectionSuzan AbdNo ratings yet
- Specimen Collection, Transport and Processing: Julius T. Capili, RMT, MPH, PHDDocument38 pagesSpecimen Collection, Transport and Processing: Julius T. Capili, RMT, MPH, PHDRica Rebadomia100% (2)
- Stool Specimen Collection PDFDocument8 pagesStool Specimen Collection PDFJane CalderonNo ratings yet
- Urine Culture: D.M.M. LabDocument15 pagesUrine Culture: D.M.M. LabTomi RahmadaniNo ratings yet
- Urine Specimen Collection: Ms. Sneha SehrawatDocument36 pagesUrine Specimen Collection: Ms. Sneha SehrawatRajaNo ratings yet
- Group 3 - ParasitologyDocument8 pagesGroup 3 - Parasitologyjulo_05No ratings yet
- SPECIMEN CollectionDocument42 pagesSPECIMEN CollectionAtmaSearch Atma Jaya100% (1)
- CLM.20 Microbiology Specimen CollectionDocument19 pagesCLM.20 Microbiology Specimen Collectionfldos universeNo ratings yet
- Blood Culture (Manual System)Document26 pagesBlood Culture (Manual System)SAMMYNo ratings yet
- Specimen CollectionDocument5 pagesSpecimen CollectionCliford BumanglagNo ratings yet
- Capillary Blood CollectionDocument8 pagesCapillary Blood CollectionARIF AHAMMED P100% (1)
- Body FluidsDocument81 pagesBody FluidsAris ResurreccionNo ratings yet
- 07 - Partograph - GLG20140212Document50 pages07 - Partograph - GLG20140212Geline Joy D. SamillanoNo ratings yet
- Bacteriology Laboratory OrganizationDocument65 pagesBacteriology Laboratory Organizationtummalapalli venkateswara rao100% (1)
- Sample Collection and TransportDocument64 pagesSample Collection and Transportvijayasree bavireddyNo ratings yet
- IUGR Case PresentationDocument21 pagesIUGR Case PresentationAlice ChirilaNo ratings yet
- Aubf Lab Types of Urine SpecimenDocument18 pagesAubf Lab Types of Urine SpecimenNerizaNo ratings yet
- Specimen CollectionDocument27 pagesSpecimen CollectionJohny Joseph100% (2)
- URINALYSIS & BODY FLUIds Pericardial Analysis.Document48 pagesURINALYSIS & BODY FLUIds Pericardial Analysis.Syazmin KhairuddinNo ratings yet
- Proper Collection and Preservation of SpecimenDocument6 pagesProper Collection and Preservation of SpecimenDavid SantosNo ratings yet
- Pre-Analytical Consideration and Venipuncture ComplicationsDocument52 pagesPre-Analytical Consideration and Venipuncture ComplicationsVenom100% (1)
- Appropriate Clinical Specimens Collection and Transport For Diagnostic VirologyDocument48 pagesAppropriate Clinical Specimens Collection and Transport For Diagnostic Virologylong thom100% (1)
- Specimen Collection, Transport and ProcessingDocument50 pagesSpecimen Collection, Transport and ProcessingJam SanchezNo ratings yet
- Course Outline in Medical MicrobiologyDocument5 pagesCourse Outline in Medical MicrobiologyRami Tounsi100% (1)
- Collection of SpecimenDocument4 pagesCollection of SpecimenHamss AhmedNo ratings yet
- Specimen Collection & Transport GuideDocument168 pagesSpecimen Collection & Transport Guidesinghranjanr5748100% (1)
- BT CT PT PTTDocument31 pagesBT CT PT PTTCristineVillablancaNo ratings yet
- Parasitology QuestionsDocument6 pagesParasitology QuestionsKolin N JandocNo ratings yet
- Coombs TestDocument11 pagesCoombs TestunilabreynosaNo ratings yet
- Hema Lesson 1Document64 pagesHema Lesson 1fleur harrisonNo ratings yet
- Collection, Transport and Storage of Specimens For Laboratory DiagnosisDocument25 pagesCollection, Transport and Storage of Specimens For Laboratory DiagnosisBrihadishwaran ThiyagarajanNo ratings yet
- Identification of BacteriaDocument4 pagesIdentification of BacteriaExamville.comNo ratings yet
- Diagnostic ParasitologyDocument35 pagesDiagnostic ParasitologyEarl Jayve Magno GoNo ratings yet
- Sputum CultureDocument6 pagesSputum CulturePranav Kumar PrabhakarNo ratings yet
- Specimen Considerations (Part 2)Document8 pagesSpecimen Considerations (Part 2)Race Mendez0% (1)
- CSF and Other Body FluidsDocument9 pagesCSF and Other Body FluidsJobelle0% (1)
- Lab DiagnosisDocument42 pagesLab DiagnosisNestley TiongsonNo ratings yet
- 56 Ambiguous GenitaliaDocument8 pages56 Ambiguous GenitalianasibdinNo ratings yet
- Fundamentals of Lab Sciences - QuDocument66 pagesFundamentals of Lab Sciences - QueebookachipNo ratings yet
- QestionsDocument12 pagesQestionsesraaNo ratings yet
- Mycobacteria: Nocardia, Rhodococcus, Tsukamurella and GordoniaDocument7 pagesMycobacteria: Nocardia, Rhodococcus, Tsukamurella and Gordonia20C – Gorospe, Rhai Chezka V.No ratings yet
- Blood Specimen Collection and ProcessingDocument6 pagesBlood Specimen Collection and ProcessingIzkandar RitzzneyNo ratings yet
- ESR (Erythrocyte Sedimentation RateDocument2 pagesESR (Erythrocyte Sedimentation RateLeah Claudia de OcampoNo ratings yet
- CSF LectureDocument58 pagesCSF Lectureshweta yadavNo ratings yet
- Urine AnalysisDocument69 pagesUrine AnalysisAffan ElahiNo ratings yet
- Reproduction and Growth in Bacteria: By: Hafiza Asfa Shafique Microbiology BS Biotechnology VDocument26 pagesReproduction and Growth in Bacteria: By: Hafiza Asfa Shafique Microbiology BS Biotechnology VJawadNo ratings yet
- Part 2 of Medical VirologyDocument113 pagesPart 2 of Medical Virologygatete samNo ratings yet
- Histochemistry Chapter 5Document48 pagesHistochemistry Chapter 5Zelalem DejazmachNo ratings yet
- Section 4 - Laboratory Biosafety Level Criteria - FINAL DOCUMENTDocument30 pagesSection 4 - Laboratory Biosafety Level Criteria - FINAL DOCUMENTEriani WulandariNo ratings yet
- CM Stool Examination (Ocfemia, Eliazel Galorio - BSLABSCI-PLTCIDocument30 pagesCM Stool Examination (Ocfemia, Eliazel Galorio - BSLABSCI-PLTCIeliazel ocfemiaNo ratings yet
- Overview of Hemolytic Disease of Fetus and Newborn Erythroblastosis FetalisDocument3 pagesOverview of Hemolytic Disease of Fetus and Newborn Erythroblastosis FetalisEditor IJTSRDNo ratings yet
- Coombs Test - Principle, Types, Procedure and Result InterpretationDocument34 pagesCoombs Test - Principle, Types, Procedure and Result InterpretationABHINABA GUPTANo ratings yet
- Stool Microscopic ExaminationDocument5 pagesStool Microscopic Examinationsamantha_ong_22No ratings yet
- Level 3Document9 pagesLevel 3Zain HadiNo ratings yet
- Prothrombin Time: Reference Range, Interpretation, Collection and ..Document3 pagesProthrombin Time: Reference Range, Interpretation, Collection and ..Francis Polycarp DiazNo ratings yet
- Anaerobic Culture .: Ahmed GomaaDocument42 pagesAnaerobic Culture .: Ahmed Gomaaah7510No ratings yet
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Specimen Collections in The Medical Microbiology and parasitologyNOTESDocument43 pagesSpecimen Collections in The Medical Microbiology and parasitologyNOTESPrincewill SeiyefaNo ratings yet
- Cap Adult UtiDocument39 pagesCap Adult UtiHartiniNo ratings yet
- Test ID: FRT4: T4 (Thyroxine), Free, SerumDocument2 pagesTest ID: FRT4: T4 (Thyroxine), Free, SerumHartiniNo ratings yet
- LAB CriticalTests 02 220Document3 pagesLAB CriticalTests 02 220HartiniNo ratings yet
- Heri Fadjari - Case StudiesDocument15 pagesHeri Fadjari - Case StudiesHartiniNo ratings yet
- Leonard Nainggolan - Predict Thrombocytes Recovery in Dengue Patients With IPFDocument28 pagesLeonard Nainggolan - Predict Thrombocytes Recovery in Dengue Patients With IPFHartiniNo ratings yet
- Algoritma Transfusi Di Kamar OperasiDocument1 pageAlgoritma Transfusi Di Kamar OperasiHartiniNo ratings yet
- Automatic Stop OrdersDocument1 pageAutomatic Stop OrdersHartiniNo ratings yet
- Inform Consent HIVDocument465 pagesInform Consent HIVHartini100% (2)
- Checklist Lean Lab MS-TSDocument15 pagesChecklist Lean Lab MS-TSHartiniNo ratings yet
- Inform Consent HIV PDFDocument1 pageInform Consent HIV PDFHartiniNo ratings yet
- Sign Antibiotic Prophylaxis in Surgery - Surgery Specific Quick Reference GuideDocument1 pageSign Antibiotic Prophylaxis in Surgery - Surgery Specific Quick Reference GuideHartiniNo ratings yet
- Sign Antibiotic Prophylaxis in Surgery - Surgery Specific Quick Reference GuideDocument1 pageSign Antibiotic Prophylaxis in Surgery - Surgery Specific Quick Reference GuideHartiniNo ratings yet
- Policies To Promote Antimicrobial Stewardship Programs PDFDocument32 pagesPolicies To Promote Antimicrobial Stewardship Programs PDFHartiniNo ratings yet
- Biological Specimen Tracking Log (Identifiable) : Study: Protocol #: PI: Lab: Storage LocationDocument1 pageBiological Specimen Tracking Log (Identifiable) : Study: Protocol #: PI: Lab: Storage LocationHartiniNo ratings yet
- Military Engineer Services Notice Inviting Tender (Nit)Document14 pagesMilitary Engineer Services Notice Inviting Tender (Nit)jatanNo ratings yet
- The Efficiency of Electrocoagulation in Treating Wastewater From A Dairy Industry, Part I: Iron ElectrodesDocument8 pagesThe Efficiency of Electrocoagulation in Treating Wastewater From A Dairy Industry, Part I: Iron ElectrodesazerfazNo ratings yet
- MCNW2820 ThinkBook 16p Gen 4 v041423Document131 pagesMCNW2820 ThinkBook 16p Gen 4 v041423james cabrezosNo ratings yet
- Airburst - Hendrick.r17 LRDocument2 pagesAirburst - Hendrick.r17 LRManuel Javier Rodríguez VNo ratings yet
- Mountain Passes of PakistanDocument3 pagesMountain Passes of PakistanMohsin Raza Maitla0% (2)
- Detecon Study Customer Experience Management in The Telecommunications Industry. Market Survey and Action Recommendations For The Optimal Design of Customer ExperiencesDocument58 pagesDetecon Study Customer Experience Management in The Telecommunications Industry. Market Survey and Action Recommendations For The Optimal Design of Customer ExperiencesDetecon InternationalNo ratings yet
- Ad620 PDFDocument16 pagesAd620 PDFRODRIGO TROCONISNo ratings yet
- Newborn Studio Guide by Jessica G. PhotographyDocument13 pagesNewborn Studio Guide by Jessica G. PhotographyClau ppNo ratings yet
- Dodds-Ancient Concept of Progress 4Document28 pagesDodds-Ancient Concept of Progress 4Trad AnonNo ratings yet
- Usmc Vector 21Document64 pagesUsmc Vector 21David PerrinNo ratings yet
- Android Quiz App 22617 MADDocument19 pagesAndroid Quiz App 22617 MADSandip kotkarNo ratings yet
- SANS 3000-4-2011 - Railway Safety RegulatorDocument115 pagesSANS 3000-4-2011 - Railway Safety RegulatorBertus ChristiaanNo ratings yet
- Estim Ated Vs Actual Wing WeightDocument9 pagesEstim Ated Vs Actual Wing WeightRoc GMNo ratings yet
- Proposal NewDocument19 pagesProposal NewAzimSyahmiNo ratings yet
- Practical Training ReportDocument6 pagesPractical Training ReportGorishsharmaNo ratings yet
- Anti-Money Laundering Regulations and Its Effectiveness: JMLC 17,4Document13 pagesAnti-Money Laundering Regulations and Its Effectiveness: JMLC 17,4hatim islamNo ratings yet
- Recent Advances in The Synthesis of Pipe Rid Ones and Piperidines PM Weintraub JS Sabol JM Kane DR Borcherding Tetrahedron 59 2953 2989 2003Document37 pagesRecent Advances in The Synthesis of Pipe Rid Ones and Piperidines PM Weintraub JS Sabol JM Kane DR Borcherding Tetrahedron 59 2953 2989 2003KybernetikumNo ratings yet
- Full Download Zoology 9th Edition Miller Test BankDocument35 pagesFull Download Zoology 9th Edition Miller Test Bankcaveneywilliams100% (25)
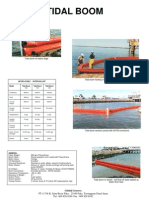
- Tidal Boom at Waters EdgeDocument1 pageTidal Boom at Waters Edgeapi-3703371No ratings yet
- BSP 2Document6 pagesBSP 2mianwaseemNo ratings yet
- A Sad Hy Arogan Ivar An A MantraDocument9 pagesA Sad Hy Arogan Ivar An A MantraKrishNo ratings yet
- ASTM D6905 - 03 Standard Test Method For Impact Flexibility of Organic CoatingsDocument3 pagesASTM D6905 - 03 Standard Test Method For Impact Flexibility of Organic CoatingsCemalOlgunÇağlayan0% (1)
- Analogy - Verbal Reasoning Questions and Answers Page 4Document2 pagesAnalogy - Verbal Reasoning Questions and Answers Page 4Palak JioNo ratings yet
- Impact of Online Gaming in Academic Performance of Students of Our Lady of Fatima University of Antipolo S.Y. 2021-2022Document9 pagesImpact of Online Gaming in Academic Performance of Students of Our Lady of Fatima University of Antipolo S.Y. 2021-2022Ralph Noah LunetaNo ratings yet
- JD ExamDocument2 pagesJD ExamCarmen T. TamacNo ratings yet
- 4 - 0 Pex DW GBDocument8 pages4 - 0 Pex DW GBpushinluckNo ratings yet