Download as pdf or txt
You might also like
- Gateway-and-Apple 1111Document5 pagesGateway-and-Apple 1111Khulan Tsetsegmaa100% (3)
- Kasatha 5eDocument1 pageKasatha 5eBryce St. LouisNo ratings yet
- 10.Q. Workshop: Evaluating Policy Using Natural Experiments and Quasi-Experimental MethodsDocument2 pages10.Q. Workshop: Evaluating Policy Using Natural Experiments and Quasi-Experimental MethodsAnandyagunaNo ratings yet
- Advantages and Limitations of Naturalistic Study Designs and Their Implementation in Alcohol Hangover ResearchDocument10 pagesAdvantages and Limitations of Naturalistic Study Designs and Their Implementation in Alcohol Hangover ResearchJere AyerbeNo ratings yet
- E009180 FullDocument14 pagesE009180 Fullsirius albertNo ratings yet
- SdarticleDocument8 pagesSdarticlePao ItzuryNo ratings yet
- Why All Randomised Controlled Trials Produce Biased ResultsDocument11 pagesWhy All Randomised Controlled Trials Produce Biased ResultsSimona BugaciuNo ratings yet
- CBR 34 47Document14 pagesCBR 34 47atouyaNo ratings yet
- The Limitations of Observation StudiesDocument5 pagesThe Limitations of Observation StudiesalbgomezNo ratings yet
- s13063 019 3444 yDocument12 pagess13063 019 3444 yAlessandra BendoNo ratings yet
- Investigating The Preferences of Older People For Telehealth As A New Model of Health Care Service Delivery: A Discrete Choice ExperimentDocument13 pagesInvestigating The Preferences of Older People For Telehealth As A New Model of Health Care Service Delivery: A Discrete Choice Experimenttherese BNo ratings yet
- Experimental StudiesDocument46 pagesExperimental StudiesPalwasha Khan100% (1)
- Effectiveness of School-Based Smoking Prevention Curricula: Systematic Review and Meta-AnalysisDocument16 pagesEffectiveness of School-Based Smoking Prevention Curricula: Systematic Review and Meta-AnalysisClaudiaGárateHenríquezNo ratings yet
- STROBE PortugueseDocument5 pagesSTROBE PortugueseBruno SilvaNo ratings yet
- Clinical TrialsDocument40 pagesClinical TrialsUmashankar SharmaNo ratings yet
- TrialsDocument25 pagesTrialsJason_Cordova_5798No ratings yet
- Fogg and Gross 2000 - Threats To Validity in Randomized Clinical TrialsDocument11 pagesFogg and Gross 2000 - Threats To Validity in Randomized Clinical TrialsChris LeeNo ratings yet
- An Extension of The CONSORT StatementDocument8 pagesAn Extension of The CONSORT StatementgfguevaraNo ratings yet
- The Patient 'S View On Rare Disease Trial Design - A Qualitative StudyDocument9 pagesThe Patient 'S View On Rare Disease Trial Design - A Qualitative StudyAMNA KHAN FITNESSSNo ratings yet
- Use of Patient Preference Studies in HTA Decision Making: A NICE PerspectiveDocument5 pagesUse of Patient Preference Studies in HTA Decision Making: A NICE Perspectiveaxel pqNo ratings yet
- Acta Obstet Gynecol Scand - 2018 - Bhide - A Simplified Guide To Randomized Controlled TrialsDocument8 pagesActa Obstet Gynecol Scand - 2018 - Bhide - A Simplified Guide To Randomized Controlled Trialscogiw65923No ratings yet
- Evidence-Practice Gaps in Lung Cancer: A Scoping Review: European Journal of Cancer Care October 2016Document13 pagesEvidence-Practice Gaps in Lung Cancer: A Scoping Review: European Journal of Cancer Care October 2016Dharpure Mr. Harshal Namdeorao --No ratings yet
- BATHE Journal PDFDocument10 pagesBATHE Journal PDFKAROMAHUL MALAYA JATINo ratings yet
- Observational Studies: Why Are They So ImportantDocument2 pagesObservational Studies: Why Are They So ImportantAndre LanzerNo ratings yet
- Etica Epidemiologicos enDocument14 pagesEtica Epidemiologicos enAlina PopaNo ratings yet
- Nutrición en DeportistasDocument21 pagesNutrición en Deportistasmorga.astridNo ratings yet
- Obesity Reviews - 2023 - Blaxall - Obesity Intervention Evidence Synthesis Where Are The Gaps and Which Should We AddressDocument18 pagesObesity Reviews - 2023 - Blaxall - Obesity Intervention Evidence Synthesis Where Are The Gaps and Which Should We AddressPatyNo ratings yet
- Dissertation Randomised Controlled TrialDocument4 pagesDissertation Randomised Controlled TrialBuyAPaperOnlineUK100% (1)
- Journal Pone 0294218Document10 pagesJournal Pone 0294218bronson.harryNo ratings yet
- Influence of Primary Care Practices On Patients' Uptake of Diabetic Retinopathy ScreeningDocument9 pagesInfluence of Primary Care Practices On Patients' Uptake of Diabetic Retinopathy ScreeningAvel GonzalesNo ratings yet
- A Systematic Review of The Effectiveness of EnviroDocument8 pagesA Systematic Review of The Effectiveness of EnviroAaron OsorioNo ratings yet
- Doing Research in General Practice: Advice For The UninitiatedDocument4 pagesDoing Research in General Practice: Advice For The UninitiatedRizky Damayanti StrahovskiNo ratings yet
- Oup Accepted Manuscript 2018Document4 pagesOup Accepted Manuscript 2018Alejandro GuzmanNo ratings yet
- GuidelineDocument24 pagesGuidelineeganNo ratings yet
- 003 - 2014-06-13 - Evidence Based Medicine A Movement in CrisisDocument7 pages003 - 2014-06-13 - Evidence Based Medicine A Movement in CrisisAušra KabišienėNo ratings yet
- Good Epidemiological Practice (GEP) IEADocument7 pagesGood Epidemiological Practice (GEP) IEAMarian MarchioriNo ratings yet
- Setting A Research Agenda For Medical Over UseDocument7 pagesSetting A Research Agenda For Medical Over UsemmNo ratings yet
- Treatment of Patients With Small-Cell Lung Cancer From Meta-AnalysesDocument9 pagesTreatment of Patients With Small-Cell Lung Cancer From Meta-AnalysesmaleticjNo ratings yet
- Effectiveness and Efficacy TrialsDocument4 pagesEffectiveness and Efficacy TrialsgfguevaraNo ratings yet
- 2004 Beyond RCT - AjphDocument6 pages2004 Beyond RCT - AjphSamuel Andrés AriasNo ratings yet
- Mejora de Validez en Investig Del Tratamiento de ComorbilidadDocument11 pagesMejora de Validez en Investig Del Tratamiento de ComorbilidadDanitza YhovannaNo ratings yet
- Patients With Gout Adhere To Curative Treatment If Informed Appropriately: Proof-Of-Concept Observational StudyDocument5 pagesPatients With Gout Adhere To Curative Treatment If Informed Appropriately: Proof-Of-Concept Observational Studytika_876267153No ratings yet
- 10 1111@jhn 12756Document10 pages10 1111@jhn 12756Federico CilloNo ratings yet
- Artikel RandomizedDocument8 pagesArtikel RandomizedUtari Meria NadaNo ratings yet
- Bioethics - 2023 - Heynemann - Therapeutic Misunderstandings in Modern ResearchDocument15 pagesBioethics - 2023 - Heynemann - Therapeutic Misunderstandings in Modern ResearchPaulo Afonso do PradoNo ratings yet
- The Causes of Prescribing Errors in English General PracticesDocument8 pagesThe Causes of Prescribing Errors in English General PracticesrosianaNo ratings yet
- International Journal of Pharmacy Practice AbstractsDocument40 pagesInternational Journal of Pharmacy Practice AbstractsFabiola NogaNo ratings yet
- 21 e 2 EfcfDocument16 pages21 e 2 Efcfsupaidi97No ratings yet
- Interventions For Preventing Delirium in Older People in Institutional Long Term CareDocument4 pagesInterventions For Preventing Delirium in Older People in Institutional Long Term Carejuan.pablo.castroNo ratings yet
- Summary of Third Expert Report 2018Document116 pagesSummary of Third Expert Report 2018Diego12001No ratings yet
- Descriptive Study - 22Document37 pagesDescriptive Study - 22santosh dnyanoba pawaleNo ratings yet
- Putting Life in Years Pliny Telephone Friendship Groups Research Study Pilot Randomised Controlled TrialDocument12 pagesPutting Life in Years Pliny Telephone Friendship Groups Research Study Pilot Randomised Controlled TrialMahmoud Abd ElazizNo ratings yet
- Effectiveness of Interventions To Reduce Ordering of Thyroid Function Tests: A Systematic ReviewDocument23 pagesEffectiveness of Interventions To Reduce Ordering of Thyroid Function Tests: A Systematic ReviewGNo ratings yet
- Atestados de La Rueda de Cambio de ComportamientoDocument7 pagesAtestados de La Rueda de Cambio de Comportamientovero060112.vcNo ratings yet
- Clinical Research and Medical CareDocument7 pagesClinical Research and Medical CareNino MdinaradzeNo ratings yet
- 2ahandout ENG 2020 ElearningDocument5 pages2ahandout ENG 2020 ElearningNupura AjeshNo ratings yet
- 1.4 Means (Opcional)Document13 pages1.4 Means (Opcional)Epi SidaNo ratings yet
- Eff Ectiveness of An Integrated Telehealth Service For PatientsDocument11 pagesEff Ectiveness of An Integrated Telehealth Service For Patientsprincejor13No ratings yet
- 2013 SMILE Published ProtocolDocument8 pages2013 SMILE Published ProtocolqqqqqNo ratings yet
- The Reporting of Studies Conducted Using Observational Routinely-Collected Health Data (Record) StatementDocument22 pagesThe Reporting of Studies Conducted Using Observational Routinely-Collected Health Data (Record) StatementMayra SaenzNo ratings yet
- Education and Debate: Qualitative Research and Evidence Based MedicineDocument11 pagesEducation and Debate: Qualitative Research and Evidence Based MedicineNúbia BatistaNo ratings yet
- LSHTM Research Online: Usage GuidlinesDocument11 pagesLSHTM Research Online: Usage GuidlinesnomdeplumNo ratings yet
- Janna Wisniewski - 2020 - Acta Trop - SR and MA of Cost-Effectiveness of ITN DistirbutionDocument10 pagesJanna Wisniewski - 2020 - Acta Trop - SR and MA of Cost-Effectiveness of ITN DistirbutionnomdeplumNo ratings yet
- Global Fund - 2017 - Supply Chain Mapping in DRCDocument42 pagesGlobal Fund - 2017 - Supply Chain Mapping in DRCnomdeplumNo ratings yet
- WHO - 2020 - VCAG 12th Meeting ReportDocument38 pagesWHO - 2020 - VCAG 12th Meeting ReportnomdeplumNo ratings yet
- 03.24.20 - PMI Malaria Program Guidance During COVIDDocument23 pages03.24.20 - PMI Malaria Program Guidance During COVIDnomdeplumNo ratings yet
- Confounded About ConfoundingDocument108 pagesConfounded About ConfoundingnomdeplumNo ratings yet
- Annex D: Case Study On The Health Network Quality Improvement System (HNQIS)Document8 pagesAnnex D: Case Study On The Health Network Quality Improvement System (HNQIS)nomdeplumNo ratings yet
- 2013 - Bhutta - Lancet - InterventionsDocument13 pages2013 - Bhutta - Lancet - InterventionsnomdeplumNo ratings yet
- 2014 - Webster - MJ - Exit Interveiws Ghana Public Health FacilitiesDocument20 pages2014 - Webster - MJ - Exit Interveiws Ghana Public Health FacilitiesnomdeplumNo ratings yet
- 2013 - Fischer Walker - Lancet - Burden of DiseaseDocument12 pages2013 - Fischer Walker - Lancet - Burden of DiseasenomdeplumNo ratings yet
- HCPP 2015 Final POP (USAID) v2 (Final) (Version To Share)Document86 pagesHCPP 2015 Final POP (USAID) v2 (Final) (Version To Share)nomdeplumNo ratings yet
- Schiavetti - 2018 - AJTMH - Quality of Medicine in KinshasaDocument10 pagesSchiavetti - 2018 - AJTMH - Quality of Medicine in KinshasanomdeplumNo ratings yet
- 2014 - Gething - MJ - Declining Malaira in Africa - Improving The Measurement of ProgressDocument5 pages2014 - Gething - MJ - Declining Malaira in Africa - Improving The Measurement of ProgressnomdeplumNo ratings yet
- State Journal - 2017 - Ben Jann Award For Code That Makes Useful Inequality OutputsDocument7 pagesState Journal - 2017 - Ben Jann Award For Code That Makes Useful Inequality OutputsnomdeplumNo ratings yet
- REPLY in Opposition To Barry MargolisDocument9 pagesREPLY in Opposition To Barry MargolisSLAVEFATHERNo ratings yet
- How Will 'Chipageddon' Affect You ?Document50 pagesHow Will 'Chipageddon' Affect You ?Satyaki DuttaNo ratings yet
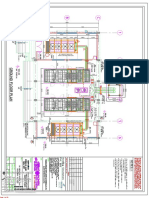
- Dg-1 (Remote Radiator) Above Control Room Slab: 05-MAR-2018 Atluri Mohan Krishna (B845)Document32 pagesDg-1 (Remote Radiator) Above Control Room Slab: 05-MAR-2018 Atluri Mohan Krishna (B845)Shaik AbdullaNo ratings yet
- Working Capital Management Maruti SuzukiDocument76 pagesWorking Capital Management Maruti SuzukiAmit singhNo ratings yet
- Knowledge of Cervical Cancer and Acceptance of HPVDocument6 pagesKnowledge of Cervical Cancer and Acceptance of HPVALIF FITRI BIN MOHD JASMINo ratings yet
- Space Planning Guidelines: Edition 2Document29 pagesSpace Planning Guidelines: Edition 2Nur Nabilah SyazwaniNo ratings yet
- FRACTAL MARKETS POI Selection)Document1 pageFRACTAL MARKETS POI Selection)malik kondoNo ratings yet
- Memoria Proyecto Informativo de Alcantarillado Domiciliario Miguel CorralDocument7 pagesMemoria Proyecto Informativo de Alcantarillado Domiciliario Miguel CorralCarlos MoralesNo ratings yet
- Course Guide For Simplified Accounting For Entrepreneurs & Professionals (Safe&P)Document7 pagesCourse Guide For Simplified Accounting For Entrepreneurs & Professionals (Safe&P)Darwin Dionisio ClementeNo ratings yet
- MPTH Reviewer Part 1Document27 pagesMPTH Reviewer Part 1Hani VitalesNo ratings yet
- English For Nursing Topic 12 Reinforcing A Dietary ProgramDocument6 pagesEnglish For Nursing Topic 12 Reinforcing A Dietary ProgramEha Huwaida HayatiNo ratings yet
- SAS Macro Tutorial ImpDocument27 pagesSAS Macro Tutorial ImpArijit DasNo ratings yet
- BFI E BrochureADocument6 pagesBFI E BrochureAAnuj JainNo ratings yet
- Oops (Object Oriented Programming Structure)Document10 pagesOops (Object Oriented Programming Structure)MANOJ SNo ratings yet
- Experimental and CFD Resistance Calculation of A Small Fast CatamaranDocument7 pagesExperimental and CFD Resistance Calculation of A Small Fast CatamaranChandra SibaraniNo ratings yet
- The Role of The School Psychologist in The Inclusive EducationDocument20 pagesThe Role of The School Psychologist in The Inclusive EducationCortés PameliNo ratings yet
- Triangle BreakoutDocument3 pagesTriangle BreakoutHarun MamatNo ratings yet
- Lyrics - More Than AbleDocument2 pagesLyrics - More Than AbleZarita CarranzaNo ratings yet
- Database Teach IctDocument3 pagesDatabase Teach IctMushawatuNo ratings yet
- Grade 8 Skeletal System Enhanced SciDocument126 pagesGrade 8 Skeletal System Enhanced SciCin TooNo ratings yet
- CH 2 Climate of PakistanDocument29 pagesCH 2 Climate of PakistanZeeshan HassanNo ratings yet
- John Champagne - The Ethics of Marginality - A New Approach To Gay Studies (1995)Document267 pagesJohn Champagne - The Ethics of Marginality - A New Approach To Gay Studies (1995)Ildikó HomaNo ratings yet
- Angela SolikovaDocument10 pagesAngela SolikovaGirisha PathakNo ratings yet
- 1 SMDocument12 pages1 SMasdNo ratings yet
- MUSIC10 Q2 (Latin American Music, Jazz and Pop Music) Week 2 - CardelDocument5 pagesMUSIC10 Q2 (Latin American Music, Jazz and Pop Music) Week 2 - CardelJeff Nieva CardelNo ratings yet
- Final Management Project On Geo TVDocument35 pagesFinal Management Project On Geo TVAli Malik100% (1)
- Scopes of Marketing AssignmentDocument4 pagesScopes of Marketing AssignmentKhira Xandria AldabaNo ratings yet
- Shoppers StopDocument35 pagesShoppers StopAditi JindalNo ratings yet