Download as pdf or txt
You might also like
- Peritoneum and Peritoneal CavityDocument26 pagesPeritoneum and Peritoneal CavitytuhinsinghNo ratings yet
- Peritoneum and Peritoneal CavityDocument26 pagesPeritoneum and Peritoneal CavitytuhinsinghNo ratings yet
- Case Incident OB MBADocument4 pagesCase Incident OB MBASahar Al-Jobury57% (7)
- Eppd-A Discourse CommunityDocument11 pagesEppd-A Discourse Communityapi-254655486No ratings yet
- Colorectal MalignancyDocument108 pagesColorectal MalignancySatishht SatishNo ratings yet
- Large Intestine.Document15 pagesLarge Intestine.Shimmering MoonNo ratings yet
- 4rd Lecture - AbdomenDocument26 pages4rd Lecture - AbdomenZainab Jamal SiddiquiNo ratings yet
- The PERITONEUMDocument27 pagesThe PERITONEUMEniola abdullahi AduagbaNo ratings yet
- Anatomy of PeritoneumDocument61 pagesAnatomy of PeritoneumFirdaus SeptiawanNo ratings yet
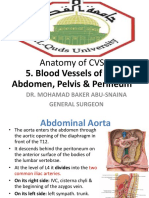
- Anatomy of CVS: 5. Blood Vessels of The Abdomen, Pelvis & PerineumDocument30 pagesAnatomy of CVS: 5. Blood Vessels of The Abdomen, Pelvis & Perineumsultan khabeebNo ratings yet
- 3 Major Arteries of GIDocument9 pages3 Major Arteries of GIbeia21No ratings yet
- Large Blood Vessels of The GutDocument61 pagesLarge Blood Vessels of The GutpoojaNo ratings yet
- Dr. Reynaldo V. Lopez Senior Lecturer Department of AnatomyDocument55 pagesDr. Reynaldo V. Lopez Senior Lecturer Department of AnatomyMohammad AliNo ratings yet
- AnatDocument119 pagesAnatGanesh RasalNo ratings yet
- Thursday, April 09, 2009 4:45 PMDocument266 pagesThursday, April 09, 2009 4:45 PMkcs2012No ratings yet
- Ana 201 (Axilla N Axillary Artery) - 1Document119 pagesAna 201 (Axilla N Axillary Artery) - 1Favour OnyeaboNo ratings yet
- Biomedic (Myology)Document19 pagesBiomedic (Myology)Sadam_fasterNo ratings yet
- Popliteal Fossa and LegDocument40 pagesPopliteal Fossa and LegRaj Shekhar SinghNo ratings yet
- Anatomi AbdomenDocument36 pagesAnatomi Abdomenari naNo ratings yet
- Anatomy (302) - 1Document82 pagesAnatomy (302) - 1Shehzad Noman SajidNo ratings yet
- Genital ProlapseDocument9 pagesGenital Prolapsesher singhNo ratings yet
- Pelvis and Perinium 2019Document59 pagesPelvis and Perinium 2019Vuluwa George100% (1)
- Thorax AllDocument174 pagesThorax Allravindra sharmaNo ratings yet
- 16-Genital ProlapseDocument37 pages16-Genital Prolapseapi-3703352No ratings yet
- A Sole 16 12 14Document51 pagesA Sole 16 12 14Mariam AymanNo ratings yet
- Anatomy VivaDocument5 pagesAnatomy Vivantege stuartNo ratings yet
- Anatomy, Lecture 9, Abdominal WallDocument22 pagesAnatomy, Lecture 9, Abdominal WallAli Al-QudsiNo ratings yet
- Femoral Region, Anterior and Medial Compartments of The ThighDocument49 pagesFemoral Region, Anterior and Medial Compartments of The ThighNolanNo ratings yet
- Adductor Canal LatestDocument18 pagesAdductor Canal LatestSaish100% (1)
- Femoral Sheath and Femoral TriangleDocument23 pagesFemoral Sheath and Femoral TriangleSamiha Haq100% (2)
- Anatomy of DiaphragmDocument21 pagesAnatomy of DiaphragmEniola abdullahi AduagbaNo ratings yet
- Upper Limb 1Document14 pagesUpper Limb 1faraNo ratings yet
- ANS Is para and SympatheticDocument34 pagesANS Is para and SympatheticAleem ZafarNo ratings yet
- Introduction To AnatomyDocument36 pagesIntroduction To AnatomyLailiyatur RofiqoNo ratings yet
- Anterior Abdominal Wall and Inguinal CanalDocument35 pagesAnterior Abdominal Wall and Inguinal Canalapi-3698357100% (3)
- 9 Anterior Triangle of The Neck E-LearningDocument22 pages9 Anterior Triangle of The Neck E-LearningHashim GhazoNo ratings yet
- Anatomy of Esophagus and StomachDocument65 pagesAnatomy of Esophagus and Stomachmackiecc100% (2)
- AXILLADocument8 pagesAXILLAImmunity RABOTANo ratings yet
- Adductor CanalDocument18 pagesAdductor CanalJanarthanan Sriram100% (1)
- Posterior Triangle of Neck and Its AppliedDocument34 pagesPosterior Triangle of Neck and Its AppliedsnehalkmNo ratings yet
- 4 AxillaDocument31 pages4 AxillaRamesh KumarNo ratings yet
- How I Evaluate The Neck Lymph NodesDocument29 pagesHow I Evaluate The Neck Lymph NodesMartín Avellaneda SantoméNo ratings yet
- Thoracic Wall.Document48 pagesThoracic Wall.Shimmering MoonNo ratings yet
- 2018 Med. Students-Lower Limb Lect.Document179 pages2018 Med. Students-Lower Limb Lect.Princewill SeiyefaNo ratings yet
- Posterior Compartment of ForearmDocument60 pagesPosterior Compartment of Forearmnickmirad2No ratings yet
- Upper LimbDocument54 pagesUpper LimbMar YNo ratings yet
- Chapter 6 Upper ExtremitiesDocument36 pagesChapter 6 Upper ExtremitiesVR VelusamyNo ratings yet
- Anatomy of Thoracic Wall: Disaripatikan Oleh Bagian Anatomi FK UnudDocument38 pagesAnatomy of Thoracic Wall: Disaripatikan Oleh Bagian Anatomi FK UnudCahyadi PermanaNo ratings yet
- Gluteal RegionDocument34 pagesGluteal Regionlion2chNo ratings yet
- The Human ThoraxDocument71 pagesThe Human Thoraxbayenn100% (2)
- AnatomyDocument74 pagesAnatomyhafeez khanNo ratings yet
- Snell AbdomenDocument43 pagesSnell AbdomenBenNo ratings yet
- Triangles of Neck (Anatomy)Document36 pagesTriangles of Neck (Anatomy)Dr Tahira Nihal100% (1)
- Abdomen Engl PDFDocument51 pagesAbdomen Engl PDFShuler0071No ratings yet
- 3-Inguinal Canal PDFDocument58 pages3-Inguinal Canal PDFN A0% (1)
- Upper Limb, Pectoral RegionDocument24 pagesUpper Limb, Pectoral Regiongtaha80No ratings yet
- 7th Week Femoral Sheath, Femoral Triangle and Adductor CanalDocument17 pages7th Week Femoral Sheath, Femoral Triangle and Adductor CanalShah NawazNo ratings yet
- 5 - Anatomy of The BreastDocument18 pages5 - Anatomy of The Breasthabtsh habshaNo ratings yet
- Upper Limb NotesDocument14 pagesUpper Limb NotesSwasChanCNo ratings yet
- Gross Anatomy of The Forearm: A CAL Package Designed By-Pratik SinhaDocument24 pagesGross Anatomy of The Forearm: A CAL Package Designed By-Pratik SinhaManvi JogiNo ratings yet
- The Lower Limb (Biomedic Unismuh 2012)Document65 pagesThe Lower Limb (Biomedic Unismuh 2012)Sadam_fasterNo ratings yet
- Arteries of Upper Limb.Document16 pagesArteries of Upper Limb.Shimmering Moon100% (1)
- Stenosing Tenosynovitis, (Trigger Finger) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandStenosing Tenosynovitis, (Trigger Finger) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Mobile Screen Sharing: 3-In-1 Cloud HD MeetingsDocument8 pagesMobile Screen Sharing: 3-In-1 Cloud HD MeetingstuhinsinghNo ratings yet
- Quality Matters - Simplicity and Ease-Of-Use - Innovating For Productivity and End-User Experience - Security - Exceptional AffordabilityDocument4 pagesQuality Matters - Simplicity and Ease-Of-Use - Innovating For Productivity and End-User Experience - Security - Exceptional AffordabilitytuhinsinghNo ratings yet
- Urinary Bladder: in Infants and Children It StartsDocument4 pagesUrinary Bladder: in Infants and Children It StartstuhinsinghNo ratings yet
- Development of UrogenitalDocument4 pagesDevelopment of UrogenitaltuhinsinghNo ratings yet
- Supplementary 4 Urinary Development LectureDocument8 pagesSupplementary 4 Urinary Development LecturetuhinsinghNo ratings yet
- Urinary Bladder: in Infants and Children It StartsDocument3 pagesUrinary Bladder: in Infants and Children It StartstuhinsinghNo ratings yet
- Development of Male Urinary BladderDocument4 pagesDevelopment of Male Urinary BladdertuhinsinghNo ratings yet
- Mikepowerpointpresentation1 130130153056 Phpapp01Document14 pagesMikepowerpointpresentation1 130130153056 Phpapp01tuhinsinghNo ratings yet
- StyloidapparatusDocument15 pagesStyloidapparatustuhinsinghNo ratings yet
- Subclavian Vessels Internal Carotid ArteryDocument26 pagesSubclavian Vessels Internal Carotid ArterytuhinsinghNo ratings yet
- PeritoneumDocument39 pagesPeritoneumtuhinsinghNo ratings yet
- PeritoneumDocument53 pagesPeritoneumtuhinsinghNo ratings yet
- Ana 2 LecDocument32 pagesAna 2 LectuhinsinghNo ratings yet
- TMJDocument34 pagesTMJtuhinsinghNo ratings yet
- GastrocnemiusDocument3 pagesGastrocnemiustuhinsinghNo ratings yet
- 1 - Intro and Histo GraysDocument67 pages1 - Intro and Histo GraystuhinsinghNo ratings yet
- Cervical Plexua, Phrenic NerveDocument15 pagesCervical Plexua, Phrenic NervetuhinsinghNo ratings yet
- Eyelid-1 Anatomy, Physiology and Congenital Anomalies of EyelidsDocument30 pagesEyelid-1 Anatomy, Physiology and Congenital Anomalies of EyelidstuhinsinghNo ratings yet
- Lecture 4Document48 pagesLecture 4tuhinsinghNo ratings yet
- Menstrual DisordersDocument29 pagesMenstrual DisorderstuhinsinghNo ratings yet
- 1.1 Notion 1.1 Notion 1.1 Notion 1.1 Notion Ofaset Ofaset Ofaset OfasetDocument3 pages1.1 Notion 1.1 Notion 1.1 Notion 1.1 Notion Ofaset Ofaset Ofaset OfasetZora IdealeNo ratings yet
- Colas, Tessie Rose D. RESUMEDocument3 pagesColas, Tessie Rose D. RESUMETessie Rose ColasNo ratings yet
- JPPvol 3 No 23Document104 pagesJPPvol 3 No 23SrishtyNo ratings yet
- Civil Procedure CodeDocument7 pagesCivil Procedure CodeKshitij AsthanaNo ratings yet
- 이휘소 논문 PDFDocument4 pages이휘소 논문 PDFjemin12798No ratings yet
- Keshav Chouhan Vs Kiran Singh 23062014 MPHC6141284COM249905Document4 pagesKeshav Chouhan Vs Kiran Singh 23062014 MPHC6141284COM249905Jeremy ChristensenNo ratings yet
- V R Siddhartha Engineering College:: Vijayawada 17EC3701A: Antennas and Wave Propagation Questions Bank UNIT: I & II A.Y 2021-22Document2 pagesV R Siddhartha Engineering College:: Vijayawada 17EC3701A: Antennas and Wave Propagation Questions Bank UNIT: I & II A.Y 2021-22Narasimhareddy MmkNo ratings yet
- I TalmudicHermeneuticsDocument6 pagesI TalmudicHermeneuticsrefugioaguiasNo ratings yet
- Addiction Homework Planner PDFDocument6 pagesAddiction Homework Planner PDFafetadcpf100% (1)
- Adverbs of Manner and Adverbs Used in ComparisonsDocument10 pagesAdverbs of Manner and Adverbs Used in Comparisonsbáh_leeNo ratings yet
- The Doctrine of The Hypostatic Union AffDocument28 pagesThe Doctrine of The Hypostatic Union AffMeland NenoNo ratings yet
- Eth Adapter CN User ManualDocument34 pagesEth Adapter CN User Manualfahim47No ratings yet
- A Presentation Digital T.V-An Innovation by AirtelDocument19 pagesA Presentation Digital T.V-An Innovation by AirtelkdkripaNo ratings yet
- First Periodical Test Research IiDocument3 pagesFirst Periodical Test Research Iirussel100% (1)
- Talleres para Grado OctavoDocument4 pagesTalleres para Grado OctavoAlëx D's DpV LeonNo ratings yet
- Stresses in Soil 161208Document67 pagesStresses in Soil 161208Tuan Jalai100% (1)
- How To Get System Status, User Status and Long Text For An ObjectDocument13 pagesHow To Get System Status, User Status and Long Text For An ObjectPiedone64No ratings yet
- Etd PDFDocument180 pagesEtd PDFhola123456789jgNo ratings yet
- KERENDIA Doctor Discussion Guide - FINALDocument2 pagesKERENDIA Doctor Discussion Guide - FINALajaygajaNo ratings yet
- NSTP-CWTS 2 - Module 2 OutputsDocument5 pagesNSTP-CWTS 2 - Module 2 OutputsJULIANA PATRICE PEREZNo ratings yet
- A Hybrid Cutting Force Model For High-Speed Milling of Titanium AlloysDocument4 pagesA Hybrid Cutting Force Model For High-Speed Milling of Titanium Alloysabdsu75No ratings yet
- Olds Waste SonataDocument2 pagesOlds Waste SonataBecca RobertsNo ratings yet
- A Critically Compassionate ApproaDocument16 pagesA Critically Compassionate ApproaAna MariaNo ratings yet
- Bringing Life Back To Classrooms Through Smart TeachingDocument4 pagesBringing Life Back To Classrooms Through Smart TeachingRaj KumarNo ratings yet
- Reasoning Mathematical Conditinal Input Kanishk@MailDocument7 pagesReasoning Mathematical Conditinal Input Kanishk@MailKainshk Gupta100% (1)
- Semana 2Document1 pageSemana 2johanaNo ratings yet
- Using Mathcad For Statics and DynamicsDocument104 pagesUsing Mathcad For Statics and Dynamicskurishi88% (8)
- Ugly DucklingDocument18 pagesUgly DucklingMarliyza MamNo ratings yet