Download as pdf or txt
You might also like
- Amazon Business Strategy 2019Document30 pagesAmazon Business Strategy 2019Mary Annjaynette I. Dalupang100% (1)
- Compressor Valves and Unloaders For Reciprocating CompressorsDocument19 pagesCompressor Valves and Unloaders For Reciprocating CompressorsGeorge Dom100% (2)
- Concept Map - HyponatremiaDocument9 pagesConcept Map - HyponatremiaElleNo ratings yet
- Addison's DiseaseDocument15 pagesAddison's DiseaseRonald A. Ogania50% (4)
- Metabolic EncephalopathyDocument26 pagesMetabolic Encephalopathywirdahaja100% (3)
- AnatomyDocument6 pagesAnatomyKadulum100% (1)
- Acute Renal FailureDocument33 pagesAcute Renal FailureAqsa Akbar AliNo ratings yet
- Acute Renal FailureDocument34 pagesAcute Renal Failureaibaloca67% (9)
- Evolution of Investment Banking in IndiaDocument3 pagesEvolution of Investment Banking in IndiaChsudarshanDhaveji100% (2)
- NationDocument88 pagesNationJustin Luu0% (1)
- Diabetes InsipidusDocument10 pagesDiabetes InsipidusRahul K. JagaNo ratings yet
- Renal FailureDocument41 pagesRenal Failure12046No ratings yet
- LevofloxacinDocument3 pagesLevofloxacinapi-3797941100% (2)
- Addison'sDocument4 pagesAddison'sKoRnflakesNo ratings yet
- HydroxyzineDocument4 pagesHydroxyzineGeorge Smith AbeledaNo ratings yet
- Drug Mode of Action Indication Contraindication Side Effects Nursing ResponsibilityDocument3 pagesDrug Mode of Action Indication Contraindication Side Effects Nursing Responsibilitykristel_nicole18yahoNo ratings yet
- Acute Kidney InjuryDocument43 pagesAcute Kidney InjuryIwan ToniroNo ratings yet
- Chronic Renal FailureDocument54 pagesChronic Renal FailureAkia Cayasan BayaNo ratings yet
- SiadhDocument10 pagesSiadhehjing75% (4)
- KaliumDocument2 pagesKaliumJustine Kaye Iballa HarligaNo ratings yet
- Case Presentation: Alcoholic GastritisDocument18 pagesCase Presentation: Alcoholic Gastritisstancy thomas100% (1)
- Chronic Kidney DiseaseDocument15 pagesChronic Kidney Diseaseapi-270623039No ratings yet
- Upper GI Bleed - SymposiumDocument38 pagesUpper GI Bleed - SymposiumSopna ZenithNo ratings yet
- Drug Profile - AmantadinDocument14 pagesDrug Profile - AmantadinAna TanNo ratings yet
- The Renin Angiotensin Aldosterone System (RAAS)Document22 pagesThe Renin Angiotensin Aldosterone System (RAAS)Chandra pranataNo ratings yet
- Course in The Ward Date, Doctor'S Order AnalysisDocument8 pagesCourse in The Ward Date, Doctor'S Order AnalysisbillyktoubattsNo ratings yet
- 14.malabsorption SyndromesDocument5 pages14.malabsorption SyndromesPriyaNo ratings yet
- TizanidineDocument2 pagesTizanidinebhawanisrNo ratings yet
- DEFINITION: Abortion Is The Expulsion or Extraction From Its MotherDocument10 pagesDEFINITION: Abortion Is The Expulsion or Extraction From Its MothermOHAN.SNo ratings yet
- DextroseDocument2 pagesDextroseSanket TelangNo ratings yet
- Drug Study RivastigmineDocument6 pagesDrug Study RivastigmineRaijenne VersolaNo ratings yet
- PHEOCHROMOCYTOMADocument25 pagesPHEOCHROMOCYTOMAKristian Dave Diva100% (1)
- Drug Study ColestipolDocument3 pagesDrug Study ColestipolAbby AngNo ratings yet
- Cretenism Case StudyDocument8 pagesCretenism Case StudyMonica Marie MoralesNo ratings yet
- Gastroesophageal Reflux Disease (Gerd) : By: Therese Jane TimbalopezDocument14 pagesGastroesophageal Reflux Disease (Gerd) : By: Therese Jane Timbalopezjoyrena ochondraNo ratings yet
- PEPTIC ULCER DISEASE 2018 EdittedDocument43 pagesPEPTIC ULCER DISEASE 2018 EdittedJumbe MohamedNo ratings yet
- Anemia in ChildrenDocument67 pagesAnemia in ChildrenDenny BimatamaNo ratings yet
- Hypertension: Colegio de San Juan de LetranDocument13 pagesHypertension: Colegio de San Juan de LetranJenna AbuanNo ratings yet
- Heart FailureDocument4 pagesHeart FailureDane WrightNo ratings yet
- Upper Gastrointestinal BleedingDocument69 pagesUpper Gastrointestinal Bleedingeliza luisNo ratings yet
- Acute Renal FailureDocument17 pagesAcute Renal FailureDina Rasmita100% (1)
- Different Iv FluidsDocument2 pagesDifferent Iv FluidsBeverly DatuNo ratings yet
- ANAMEIA PPT BY SandeepDocument32 pagesANAMEIA PPT BY SandeepSandeep ChakravarthyNo ratings yet
- Case Study 18Document4 pagesCase Study 18api-271284613No ratings yet
- Serum ElectrolytesDocument2 pagesSerum ElectrolytesKervin CablaidaNo ratings yet
- Vidconf Diuretic Antidiuretic 2014Document51 pagesVidconf Diuretic Antidiuretic 2014naltrisilvianNo ratings yet
- PrevacidDocument2 pagesPrevacidianecunar100% (2)
- Learning Objectives:: Pathophysiology & Therapeutics, I (MSPR 521) Lecture No. 14Document9 pagesLearning Objectives:: Pathophysiology & Therapeutics, I (MSPR 521) Lecture No. 14adzhangNo ratings yet
- Aplastic AnemiaDocument21 pagesAplastic AnemiaJennifer DixonNo ratings yet
- Acute GlomerulonephritisDocument21 pagesAcute Glomerulonephritisbrinda johnNo ratings yet
- Drug StudyDocument4 pagesDrug StudyCharlayne AnneNo ratings yet
- Trifluoperazine Drug StudyDocument5 pagesTrifluoperazine Drug Studyshadow gonzalezNo ratings yet
- Pathophysiology CKDDocument2 pagesPathophysiology CKDSugar Capule - ManuelNo ratings yet
- Acute Post-Streptococcal GlomerulonephritisDocument15 pagesAcute Post-Streptococcal GlomerulonephritisJeanne Marie ValesNo ratings yet
- Diabetic NephropathyDocument6 pagesDiabetic NephropathyZulfadliZulfadliNo ratings yet
- MoxifloxacinDocument23 pagesMoxifloxacinKaaghu Raghu Micha0% (1)
- Case Study 1Document6 pagesCase Study 1rajambal_ayyasamy0% (1)
- Case Presentation On Chronic Kidney Disease1Document18 pagesCase Presentation On Chronic Kidney Disease1d100% (1)
- Diabetic KetoacidosisDocument22 pagesDiabetic KetoacidosismartinNo ratings yet
- Chronic Renal FailureDocument46 pagesChronic Renal Failurestepharry08100% (1)
- Syndrome of Inappropriate Vasopressin Sexretion (Siadh)Document22 pagesSyndrome of Inappropriate Vasopressin Sexretion (Siadh)Moni RethNo ratings yet
- Diabetes Insipidus, Siadh and Cerebral Salt-WastingDocument33 pagesDiabetes Insipidus, Siadh and Cerebral Salt-WastingEuphrasiaNo ratings yet
- Diabetes Insipidus HandoutDocument4 pagesDiabetes Insipidus HandoutllianNo ratings yet
- By: Irwan Subekti, Skep, NersDocument26 pagesBy: Irwan Subekti, Skep, NersEric Juan MaldiniNo ratings yet
- Syndrome of Inappropriate Vasopressin Sexretion (Siadh)Document22 pagesSyndrome of Inappropriate Vasopressin Sexretion (Siadh)Moni RethNo ratings yet
- Hypothyroidism (2016)Document23 pagesHypothyroidism (2016)Moni RethNo ratings yet
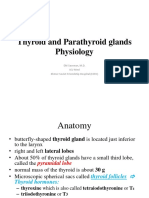
- Thyroid Gland (2015-16)Document49 pagesThyroid Gland (2015-16)Moni RethNo ratings yet
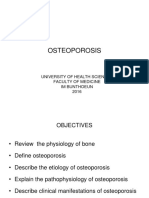
- Osteoporosis: University of Health Sciences Faculty of Medicine Im Bunthoeun 2016Document17 pagesOsteoporosis: University of Health Sciences Faculty of Medicine Im Bunthoeun 2016Moni RethNo ratings yet
- House Beautiful 2010 Spring SummerDocument124 pagesHouse Beautiful 2010 Spring SummerAnnabel Lee100% (2)
- Revit Architecture - FCP Questions & AnswersDocument14 pagesRevit Architecture - FCP Questions & AnswersMohan Kumar100% (1)
- Navya MVH HCQDocument13 pagesNavya MVH HCQhosur mvNo ratings yet
- Notes Industrial Security ConceptsDocument40 pagesNotes Industrial Security ConceptsAC GonzagaNo ratings yet
- 4 Lista Teme Disertatie 2020-2021 BSCMC EnglezaDocument3 pages4 Lista Teme Disertatie 2020-2021 BSCMC EnglezaqawsfawsfNo ratings yet
- DBX PA Cut SheetA2Document2 pagesDBX PA Cut SheetA2Willy WakkerNo ratings yet
- Academic Year 2019-2020: St. John College of Humanities & SciencesDocument78 pagesAcademic Year 2019-2020: St. John College of Humanities & SciencesRinkesh SoniNo ratings yet
- Understanding Order ProcessDocument7 pagesUnderstanding Order ProcessfilipNo ratings yet
- GCED GraphDocument1 pageGCED GraphWan Redzwan KadirNo ratings yet
- F.Y. B.Tech. (Semester - I) (Revised) Examination, December - 2018 Fundamentals of Electronics and Computers (All Branches)Document2 pagesF.Y. B.Tech. (Semester - I) (Revised) Examination, December - 2018 Fundamentals of Electronics and Computers (All Branches)Saurabh BhiseNo ratings yet
- Mill Test A36Document3 pagesMill Test A36Dang TranNo ratings yet
- Power Apps Deployment Using ADODocument25 pagesPower Apps Deployment Using ADOSameer Wadkar32No ratings yet
- Blue-Eyes White Dragon DeckDocument1 pageBlue-Eyes White Dragon DeckJad hack'sNo ratings yet
- P To P CycleDocument5 pagesP To P CycleJaved AhmadNo ratings yet
- Guidelinefor CentreSuperintendentPrac9.02.2013Document120 pagesGuidelinefor CentreSuperintendentPrac9.02.2013JasmineNo ratings yet
- Linux IPv6 How ToDocument164 pagesLinux IPv6 How ToAri SetianiNo ratings yet
- Peter Wicke - Rock Music Culture Aesthetic and SociologyDocument121 pagesPeter Wicke - Rock Music Culture Aesthetic and SociologyFelipeNo ratings yet
- Lesson Plan For TlsDocument7 pagesLesson Plan For TlsAini NordinNo ratings yet
- Iso 30400-2016Document12 pagesIso 30400-2016Shekhar100% (3)
- Unit 1 Basic Principles of Communication: StructureDocument18 pagesUnit 1 Basic Principles of Communication: Structuresastrylanka_1980No ratings yet
- 1967 1 EngDocument17 pages1967 1 EngTateNo ratings yet
- Passing Package PDFDocument10 pagesPassing Package PDFAddds Muhammmed100% (1)
- Dh3 Generation Lototo Plan Phase 1 RGC 08sep2023Document8 pagesDh3 Generation Lototo Plan Phase 1 RGC 08sep2023Borislav VulicNo ratings yet
- DDocument17 pagesDAlaa ElghazalyNo ratings yet
- As 1767.2.3-1999 Insulating Liquids Test Methods - Method of Sampling Liquid DielectricsDocument8 pagesAs 1767.2.3-1999 Insulating Liquids Test Methods - Method of Sampling Liquid DielectricsSAI Global - APACNo ratings yet
- MICFL Annual Report 2017-18Document147 pagesMICFL Annual Report 2017-18Hasan Mohammad MahediNo ratings yet