Download as docx, pdf, or txt
You might also like
- Psych Drugs Cheat SheetDocument4 pagesPsych Drugs Cheat SheetSunel100% (43)
- Antidepressant Comparison ChartDocument3 pagesAntidepressant Comparison Chartiggyputtty100% (29)
- 966baf PDFDocument86 pages966baf PDFkaw gd100% (2)
- 1000 MCQ Book Pain MedicineDocument215 pages1000 MCQ Book Pain Medicineihtisham1100% (16)
- PEAC DepressionDocument47 pagesPEAC DepressionSd100% (2)
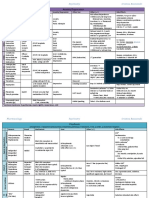
- Photosensitizing Medication ListDocument3 pagesPhotosensitizing Medication ListDimas RfNo ratings yet
- Psychiatry Pharmacology J. Psychiatry' AntidepressantsDocument9 pagesPsychiatry Pharmacology J. Psychiatry' AntidepressantssumithjalyNo ratings yet
- Hypothyroidism - Harrison Copy-PasteDocument4 pagesHypothyroidism - Harrison Copy-PasteJoseph De Joya100% (1)
- Antipsychotic or Neuroleptic DrugsDocument12 pagesAntipsychotic or Neuroleptic Drugscamile buhanginNo ratings yet
- Psychopharmacology NewestDocument43 pagesPsychopharmacology NewestRegina PunNo ratings yet
- Drug ListDocument30 pagesDrug ListKristineNo ratings yet
- 4.2 Psychotropic Drugs Used in PsychiatryDocument32 pages4.2 Psychotropic Drugs Used in PsychiatryAmar Nur Arif ZazuliNo ratings yet
- Short Guide To Psychiatric DrugsDocument17 pagesShort Guide To Psychiatric Drugsjaume1010No ratings yet
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsDocument29 pagesPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaNo ratings yet
- Pharmacology - (5) Psychotic DrugsDocument8 pagesPharmacology - (5) Psychotic DrugsSamantha DiegoNo ratings yet
- Psychotropics NotesDocument5 pagesPsychotropics NotesJulianna Rheaven JoreNo ratings yet
- Common Psych DrugsDocument3 pagesCommon Psych Drugsrexinne noahNo ratings yet
- Crisis Evaluation of The Perinatal Woman PPT. Ouellette MDDocument42 pagesCrisis Evaluation of The Perinatal Woman PPT. Ouellette MDmanjuskkNo ratings yet
- Dementia & DeliriumDocument7 pagesDementia & DeliriumSudesna Roy ChowdhuryNo ratings yet
- Antidepressants Comparison Guide Most Commonly Prescribed: Recommend GenericsDocument3 pagesAntidepressants Comparison Guide Most Commonly Prescribed: Recommend GenericsCarina ColtuneacNo ratings yet
- Laboratory Monitoring When Prescribing PsychotropicsDocument5 pagesLaboratory Monitoring When Prescribing PsychotropicswaleskacrzNo ratings yet
- Psycho PharmaDocument8 pagesPsycho PharmaMark JosephNo ratings yet
- Dr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityDocument41 pagesDr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American Universityredderdat100% (1)
- Final Coaching DrugsDocument8 pagesFinal Coaching DrugsSherlyn BesasNo ratings yet
- Lecture 29 30 Thyroid TherapeuticsDocument3 pagesLecture 29 30 Thyroid TherapeuticsAhmed MashalyNo ratings yet
- Antidepressants and Mood StabilizersDocument4 pagesAntidepressants and Mood Stabilizers우정은No ratings yet
- Anxiety/Depression: S AlprazolamDocument2 pagesAnxiety/Depression: S AlprazolamleesaNo ratings yet
- Sudden Onset (Within 2 Weeks) of at Least One of TheDocument2 pagesSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaNo ratings yet
- Fig psychiatricAssessmentFormDocument4 pagesFig psychiatricAssessmentFormabbey jane mallillin100% (1)
- I. Anxiolytic and Hypnotic AgentsDocument32 pagesI. Anxiolytic and Hypnotic AgentsDanica Abarquez100% (1)
- Psych Ch. 5 NotesDocument7 pagesPsych Ch. 5 NotesHaylle ThomasNo ratings yet
- Perinatal Mood and Anxiety Disorders: What Are They?Document2 pagesPerinatal Mood and Anxiety Disorders: What Are They?Maranda BartschiNo ratings yet
- Treatment Resistant OCD .Document55 pagesTreatment Resistant OCD .Dr viren SolankiNo ratings yet
- Pharmacological Management of DepressionDocument66 pagesPharmacological Management of DepressionPriyash JainNo ratings yet
- Just Getting The Main RX Names Down : Antidepressants Mood StabilizersDocument1 pageJust Getting The Main RX Names Down : Antidepressants Mood StabilizersCarlos Eduardo LinaresNo ratings yet
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationDocument6 pagesAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord Verazon100% (1)
- Assessment in Forensic PsychiatryDocument32 pagesAssessment in Forensic PsychiatryRahelAdmasuNo ratings yet
- 10 Cognitive DisordersDocument16 pages10 Cognitive DisordersFarrah MaeNo ratings yet
- Pharmacology 2 NotesDocument18 pagesPharmacology 2 NotesAnna ConigraveNo ratings yet
- Mneumonics PsychDxDocument7 pagesMneumonics PsychDxSuraj MukatiraNo ratings yet
- Drug List Psych Optho NeuroDocument22 pagesDrug List Psych Optho NeuroAshley BarrileNo ratings yet
- Pharmacology Test 1Document39 pagesPharmacology Test 1Niki BolinNo ratings yet
- 1: Adhd: Scientific Name Dose CommentsDocument4 pages1: Adhd: Scientific Name Dose CommentsSadiq Abdo92No ratings yet
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Adrenergic PharmacologyDocument6 pagesAdrenergic Pharmacologyjess6001No ratings yet
- Adjuvant AnalgesicsDocument44 pagesAdjuvant AnalgesicsZulfan EfendiNo ratings yet
- Description of Location Description of FunctionDocument2 pagesDescription of Location Description of FunctionbrendaNo ratings yet
- Geriatric Giants - DR SeymourDocument108 pagesGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Adrenergic AgentsDocument57 pagesAdrenergic AgentsAn Lo100% (1)
- Of Angina Pectoris. Decreased Rate of Cardiovascular Mortality and Hospitalization in Patients With Heart FailureDocument31 pagesOf Angina Pectoris. Decreased Rate of Cardiovascular Mortality and Hospitalization in Patients With Heart Failurenaikram420No ratings yet
- Interview Pa Tool.Document5 pagesInterview Pa Tool.Raisah Bint AbdullahNo ratings yet
- 504 - Pediatric Psychopharmacology - General PrinciplesDocument54 pages504 - Pediatric Psychopharmacology - General PrinciplesAlvaro HuidobroNo ratings yet
- Geriatric Psychiatry Group CDocument77 pagesGeriatric Psychiatry Group Cchew weijianNo ratings yet
- A Nurse PractitionerDocument4 pagesA Nurse PractitionerN.DanielaNo ratings yet
- 5 Internalizing Behaviors Anxiety OCD 20032023 102919amDocument57 pages5 Internalizing Behaviors Anxiety OCD 20032023 102919amayesha kamalNo ratings yet
- Anidepressant Drugs: Pratik KhanalDocument37 pagesAnidepressant Drugs: Pratik KhanalPratik Khanal100% (1)
- Mechanisms of Drug Interactions: A. AbsorptionDocument4 pagesMechanisms of Drug Interactions: A. AbsorptionAnne Geleen BraganzaNo ratings yet
- Handy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Document3 pagesHandy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Mariya ZhekovaNo ratings yet
- Pharmacology Review For FinalsDocument9 pagesPharmacology Review For FinalsJaya ReyesNo ratings yet
- Initial Interview TemplateDocument4 pagesInitial Interview TemplateJoan ChoiNo ratings yet
- Electroconvulsive Therapy: Aban, Katherine Maebelle G. Esguerra, Dianne Carmela RDocument46 pagesElectroconvulsive Therapy: Aban, Katherine Maebelle G. Esguerra, Dianne Carmela REdgar ManoodNo ratings yet
- Neurotransmitters Cuadro PDFDocument2 pagesNeurotransmitters Cuadro PDFCarina Castillo Valdiviezo100% (1)
- Antipsychotic DrugsDocument47 pagesAntipsychotic DrugsIkram UddinNo ratings yet
- Ethical Issues in Clinical Forensic PsychiatryFrom EverandEthical Issues in Clinical Forensic PsychiatryArtemis IgoumenouNo ratings yet
- Teenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenFrom EverandTeenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenNo ratings yet
- Hyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Adjuvant Analgesics (2015) PDFDocument177 pagesAdjuvant Analgesics (2015) PDFsatriomega100% (1)
- Desipramine (RX) : Patient HandoutDocument4 pagesDesipramine (RX) : Patient HandoutWilliam OmarNo ratings yet
- Desipramine Drug Information - UpToDateDocument32 pagesDesipramine Drug Information - UpToDateWilliam OmarNo ratings yet
- Pharmacology Module Answers Quizzes and Test Bank 1Document228 pagesPharmacology Module Answers Quizzes and Test Bank 1Justine Rabanes100% (2)
- Quick Reference BWDocument2 pagesQuick Reference BWmcbermudezNo ratings yet
- Active Metabolites As Antidepressant Drugs: The Role of Norquetiapine in The Mechanism of Action of Quetiapine in The Treatment of Mood DisordersDocument8 pagesActive Metabolites As Antidepressant Drugs: The Role of Norquetiapine in The Mechanism of Action of Quetiapine in The Treatment of Mood DisordersNath miaounNo ratings yet
- Psychiatric and Behavioral DisordersDocument26 pagesPsychiatric and Behavioral DisordersismailcemNo ratings yet
- Management of Migraine Headache: An Overview of Current PracticeDocument7 pagesManagement of Migraine Headache: An Overview of Current Practicelili yatiNo ratings yet
- Antihistamine MedicationsDocument1 pageAntihistamine MedicationsCora GougeNo ratings yet
- H01043-Hoá Dư C 2-Lecture 6-AntidepressantsDocument26 pagesH01043-Hoá Dư C 2-Lecture 6-AntidepressantsKTrọng NghĩaNo ratings yet
- AntidepressantsDocument3 pagesAntidepressantsA HNo ratings yet
- Psychiatric Disorders in Medical Practice: Specific SyndromesDocument14 pagesPsychiatric Disorders in Medical Practice: Specific SyndromesEduard TomițaNo ratings yet
- Desipramine (RX) : WarningsDocument2 pagesDesipramine (RX) : WarningsWilliam OmarNo ratings yet
- Dan J. Stein - Philosophy of Psychopharmacology - Smart Pills, Happy Pills, and Pep Pills (2008) PDFDocument224 pagesDan J. Stein - Philosophy of Psychopharmacology - Smart Pills, Happy Pills, and Pep Pills (2008) PDFAve ClaudiuNo ratings yet
- Preferentially Block Uptake of 5-HT Preferentially Block Uptake of NADocument3 pagesPreferentially Block Uptake of 5-HT Preferentially Block Uptake of NAThư Phạm100% (1)
- Antipsychotic DrugsDocument9 pagesAntipsychotic DrugsMel SevillaNo ratings yet
- Slides Antidepressants CNS PharmacologyDocument39 pagesSlides Antidepressants CNS PharmacologyRuva Oscass JimmyNo ratings yet
- 1 Mood Disorders Whole Document 1Document10 pages1 Mood Disorders Whole Document 1Myles Zen Dieta EaNo ratings yet
- Desipramine (RX) : ImagesDocument6 pagesDesipramine (RX) : ImagesWilliam OmarNo ratings yet
- JBC-Article-Vol-14-Issue-2 5-What You Should Know About Attention Deficit Disorder-WelchDocument6 pagesJBC-Article-Vol-14-Issue-2 5-What You Should Know About Attention Deficit Disorder-WelchtghsilvaNo ratings yet
- Dr. Moch. Bahrudin, SP.S: Bagian Neurologi Fakultas Kedokteran Universitas Muhammadiyah MalangDocument34 pagesDr. Moch. Bahrudin, SP.S: Bagian Neurologi Fakultas Kedokteran Universitas Muhammadiyah MalangputrimeilissaNo ratings yet
- Chapter 2 Neurobiologic Theories and Psycho PharmacologyDocument36 pagesChapter 2 Neurobiologic Theories and Psycho PharmacologyPrecious Pearl Tadena100% (1)
- Psychopharmacology in PsychiatryDocument94 pagesPsychopharmacology in PsychiatryOslo Saputra100% (1)
- Psychopharma 1Document7 pagesPsychopharma 1Mitchee Zialcita100% (1)