Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Treatment Planning of Teeth With Compromised Clinical Crowns Endodontic, Reconstructive, and Surgical StrategyDocument20 pagesTreatment Planning of Teeth With Compromised Clinical Crowns Endodontic, Reconstructive, and Surgical Strategyfloressam2000No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- EPQ On The Mental Health SystemDocument15 pagesEPQ On The Mental Health SystemAdam100% (2)
- Microbiology Pharm D 2nd Year Question BankDocument13 pagesMicrobiology Pharm D 2nd Year Question Bankshasvina05No ratings yet
- Dressing and Bandaging in First Aid: Wound Healing BandageDocument8 pagesDressing and Bandaging in First Aid: Wound Healing BandageRosalouise P. UngabNo ratings yet
- Biomedicines: The Role of IL-6 in Skin Fibrosis and Cutaneous Wound HealingDocument18 pagesBiomedicines: The Role of IL-6 in Skin Fibrosis and Cutaneous Wound Healingka waiiNo ratings yet
- Ncbi List of Books and Dental ArticlesDocument6 pagesNcbi List of Books and Dental ArticlesIulia Isacov0% (1)
- Failure To Thrive - AAPDocument11 pagesFailure To Thrive - AAPAlexNo ratings yet
- Placenta AcretaDocument5 pagesPlacenta AcretaFrancisca MoennigNo ratings yet
- Clove Overview of Potential Health Benefits.9Document18 pagesClove Overview of Potential Health Benefits.9Dr-Akash SanthoshNo ratings yet
- BiopsyDocument22 pagesBiopsysrai60584No ratings yet
- Protap NTG DripDocument4 pagesProtap NTG DripAinil MardiahNo ratings yet
- Urinary IncontinenceDocument5 pagesUrinary IncontinencefakrulnersmudaNo ratings yet
- Enf Tiroidea y Embarazo Lancet 2018Document12 pagesEnf Tiroidea y Embarazo Lancet 2018Jair Alexander Quintero PanucoNo ratings yet
- Artificial IntelligenceDocument21 pagesArtificial Intelligenceaditya bNo ratings yet
- NCP (Gonzales) Mar 29 - Ventura PDFDocument3 pagesNCP (Gonzales) Mar 29 - Ventura PDFJian VenturaNo ratings yet
- Mcgraw-Hill Companies, IncDocument2 pagesMcgraw-Hill Companies, IncLu LubNaNo ratings yet
- Attention Deficit-Hyperactive DisorderDocument3 pagesAttention Deficit-Hyperactive Disorderadan oladiveNo ratings yet
- Active Assisted and Passive Movement in TreatmentDocument4 pagesActive Assisted and Passive Movement in TreatmentshravaniNo ratings yet
- CCO NSCLC Practical Guidance DownloadableDocument109 pagesCCO NSCLC Practical Guidance DownloadableKhai Diệp HoàngNo ratings yet
- General Principles of Clinical ToxicologyDocument34 pagesGeneral Principles of Clinical ToxicologySigita KazūneNo ratings yet
- HNF 42 Case StudyDocument25 pagesHNF 42 Case StudyDana SablanNo ratings yet
- Magnetic Therapy The Alternative Magnetic Therapy HealingDocument22 pagesMagnetic Therapy The Alternative Magnetic Therapy Healingnfarah100% (1)
- Antivenom Reactions IntroductionDocument14 pagesAntivenom Reactions IntroductionppgpcsNo ratings yet
- Gingivitis & PeriodontitisDocument24 pagesGingivitis & PeriodontitisHafid Nur ArzanudinNo ratings yet
- Pediatrics in Review - February2011Document86 pagesPediatrics in Review - February2011Manuel AlvaradoNo ratings yet
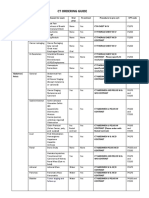
- CT Ordering Guide: Tumor Staging and Follow UpDocument2 pagesCT Ordering Guide: Tumor Staging and Follow UpanonNo ratings yet
- Cardiac Inspection and Palpation CardiologyDocument25 pagesCardiac Inspection and Palpation CardiologyMohamed El SayedNo ratings yet
- Hypertension in PregnancyDocument29 pagesHypertension in PregnancyArchana KumariNo ratings yet
- 6th March 2020 Plab 1 MockDocument32 pages6th March 2020 Plab 1 MockZoha QureshiNo ratings yet
- GlaucomaDocument18 pagesGlaucomaOncología CdsNo ratings yet