
C5 Palsy After Cervical Spine Surgery - A Multicenter Retrospective Review of 59 Cases
C5 Palsy After Cervical Spine Surgery - A Multicenter Retrospective Review of 59 Cases
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Gunn Approach To The Treatment of Chronic PainDocument185 pagesThe Gunn Approach To The Treatment of Chronic PainSamuelSeto75% (12)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- HSS - Summer 2020 - Syllabus - ANTH 1667Document7 pagesHSS - Summer 2020 - Syllabus - ANTH 1667Bruce JobseNo ratings yet
- Cervical Orthopedic Tests: WSCC Clinics ProtocolDocument31 pagesCervical Orthopedic Tests: WSCC Clinics ProtocolRana Amgad100% (1)
- A Year of Blessings: Regina Coeli ReportDocument12 pagesA Year of Blessings: Regina Coeli ReportBruce JobseNo ratings yet
- Vexilliod Tabloid - 73Document12 pagesVexilliod Tabloid - 73Bruce JobseNo ratings yet
- Metal Gods: Dominic Covey Chris DavisDocument66 pagesMetal Gods: Dominic Covey Chris DavisBruce JobseNo ratings yet
- Charles Rice: Cover: EditingDocument11 pagesCharles Rice: Cover: EditingBruce JobseNo ratings yet
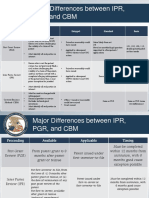
- Major Differences Between IPR, PGR, and CBM: Inter Partes Review (IPR) Petitioner Estoppel Standard BasisDocument2 pagesMajor Differences Between IPR, PGR, and CBM: Inter Partes Review (IPR) Petitioner Estoppel Standard BasisBruce JobseNo ratings yet
- Freeway Warrior 02 PDFDocument301 pagesFreeway Warrior 02 PDFBruce Jobse100% (1)
- Ischiofemoral Impingement SyndromeDocument5 pagesIschiofemoral Impingement SyndromeMmg Biggy KNo ratings yet
- Clinically Organized Relevant Exam CORE Neck Tool EditedDocument9 pagesClinically Organized Relevant Exam CORE Neck Tool EditedGeorge wrightNo ratings yet
- Cervical Orthopedics Test/Sign Procedure (+) INDDocument39 pagesCervical Orthopedics Test/Sign Procedure (+) INDDesi SmithNo ratings yet
- Diagnosis and Treatment of Sciatica2Document6 pagesDiagnosis and Treatment of Sciatica2Hayyu F RachmadhanNo ratings yet
- Various Use of Lingu - Dabai Point Combination BY MK Sastry: No. Symptoms Affected Side Opposite Side Other PointsDocument3 pagesVarious Use of Lingu - Dabai Point Combination BY MK Sastry: No. Symptoms Affected Side Opposite Side Other PointsAnonymous 5IUoLwGSdNo ratings yet
- Aaos Spine 2020.Document71 pagesAaos Spine 2020.ABUBAKER ZANBOUZINo ratings yet
- Musculoskeletal ICD-10-CM Coding Tip Sheet: Overview of Key Chapter 13 UpdatesDocument3 pagesMusculoskeletal ICD-10-CM Coding Tip Sheet: Overview of Key Chapter 13 UpdatesAneez Malik100% (1)
- AXIOM DRX9000 Ver 2 For UploadDocument14 pagesAXIOM DRX9000 Ver 2 For UploadNik Haniff HanafiNo ratings yet
- Hip Vs SpineDocument12 pagesHip Vs Spinevaibhav gowdaNo ratings yet
- Neck Hammock v. Does - ComplaintDocument89 pagesNeck Hammock v. Does - ComplaintSarah BursteinNo ratings yet
- Cervical Spondylosis HistoryDocument2 pagesCervical Spondylosis HistorycarinasheliapNo ratings yet
- Spondylosis, Cervical and LumbarDocument1 pageSpondylosis, Cervical and LumbarLuis HerreraNo ratings yet
- Traction NursingDocument75 pagesTraction NursingSujith KuttanNo ratings yet
- Carolyn O'Neal v. Fremont County Board of Commissioners, Et Al.Document40 pagesCarolyn O'Neal v. Fremont County Board of Commissioners, Et Al.Michael_Lee_RobertsNo ratings yet
- Tentative Ruling in Florencio Munguia v. County of San BernardinoDocument9 pagesTentative Ruling in Florencio Munguia v. County of San BernardinoBeau YarbroughNo ratings yet
- Late Responses: Table 4-1. Late Responses: F Response and H Reflex F Response H ReflexDocument11 pagesLate Responses: Table 4-1. Late Responses: F Response and H Reflex F Response H ReflexIzabella MihályNo ratings yet
- Bogduk 2009Document3 pagesBogduk 2009Borys100% (1)
- Cervical Disc ProlapseDocument27 pagesCervical Disc ProlapseMaroofAliNo ratings yet
- Neck Pain and Lower Back Pain. Med Clin N Am. 2019.Document14 pagesNeck Pain and Lower Back Pain. Med Clin N Am. 2019.Jose Fernando Diez100% (1)
- What Is Physiatry 2022Document2 pagesWhat Is Physiatry 2022Victoria GonzalezNo ratings yet
- Rios Vazquez v. SHHS, 45 F.3d 424, 1st Cir. (1995)Document6 pagesRios Vazquez v. SHHS, 45 F.3d 424, 1st Cir. (1995)Scribd Government DocsNo ratings yet
- Cervical RadiculopathyDocument7 pagesCervical Radiculopathyrhymescsf100% (1)
- Herniated Nucleus Pulposus TreatmentDocument19 pagesHerniated Nucleus Pulposus Treatmentvicky174No ratings yet
- Oscar Montalvo v. Secretary of Health and Human Services, 960 F.2d 143, 1st Cir. (1992)Document6 pagesOscar Montalvo v. Secretary of Health and Human Services, 960 F.2d 143, 1st Cir. (1992)Scribd Government DocsNo ratings yet
- Differential Diagnosis of Cervicobrachial PainDocument11 pagesDifferential Diagnosis of Cervicobrachial PainpuchioNo ratings yet
- Guidelines For Evaluation and Management of LBPDocument482 pagesGuidelines For Evaluation and Management of LBPShashi JainNo ratings yet
- Peripheral Neuropathy: Evaluation and Differential DiagnosisDocument8 pagesPeripheral Neuropathy: Evaluation and Differential DiagnosisBintu Searching-FriendNo ratings yet











































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Gunn Approach To The Treatment of Chronic PainDocument185 pagesThe Gunn Approach To The Treatment of Chronic PainSamuelSeto75% (12)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- HSS - Summer 2020 - Syllabus - ANTH 1667Document7 pagesHSS - Summer 2020 - Syllabus - ANTH 1667Bruce JobseNo ratings yet
- Cervical Orthopedic Tests: WSCC Clinics ProtocolDocument31 pagesCervical Orthopedic Tests: WSCC Clinics ProtocolRana Amgad100% (1)
- A Year of Blessings: Regina Coeli ReportDocument12 pagesA Year of Blessings: Regina Coeli ReportBruce JobseNo ratings yet
- Vexilliod Tabloid - 73Document12 pagesVexilliod Tabloid - 73Bruce JobseNo ratings yet
- Metal Gods: Dominic Covey Chris DavisDocument66 pagesMetal Gods: Dominic Covey Chris DavisBruce JobseNo ratings yet
- Charles Rice: Cover: EditingDocument11 pagesCharles Rice: Cover: EditingBruce JobseNo ratings yet
- Major Differences Between IPR, PGR, and CBM: Inter Partes Review (IPR) Petitioner Estoppel Standard BasisDocument2 pagesMajor Differences Between IPR, PGR, and CBM: Inter Partes Review (IPR) Petitioner Estoppel Standard BasisBruce JobseNo ratings yet
- Freeway Warrior 02 PDFDocument301 pagesFreeway Warrior 02 PDFBruce Jobse100% (1)
- Ischiofemoral Impingement SyndromeDocument5 pagesIschiofemoral Impingement SyndromeMmg Biggy KNo ratings yet
- Clinically Organized Relevant Exam CORE Neck Tool EditedDocument9 pagesClinically Organized Relevant Exam CORE Neck Tool EditedGeorge wrightNo ratings yet
- Cervical Orthopedics Test/Sign Procedure (+) INDDocument39 pagesCervical Orthopedics Test/Sign Procedure (+) INDDesi SmithNo ratings yet
- Diagnosis and Treatment of Sciatica2Document6 pagesDiagnosis and Treatment of Sciatica2Hayyu F RachmadhanNo ratings yet
- Various Use of Lingu - Dabai Point Combination BY MK Sastry: No. Symptoms Affected Side Opposite Side Other PointsDocument3 pagesVarious Use of Lingu - Dabai Point Combination BY MK Sastry: No. Symptoms Affected Side Opposite Side Other PointsAnonymous 5IUoLwGSdNo ratings yet
- Aaos Spine 2020.Document71 pagesAaos Spine 2020.ABUBAKER ZANBOUZINo ratings yet
- Musculoskeletal ICD-10-CM Coding Tip Sheet: Overview of Key Chapter 13 UpdatesDocument3 pagesMusculoskeletal ICD-10-CM Coding Tip Sheet: Overview of Key Chapter 13 UpdatesAneez Malik100% (1)
- AXIOM DRX9000 Ver 2 For UploadDocument14 pagesAXIOM DRX9000 Ver 2 For UploadNik Haniff HanafiNo ratings yet
- Hip Vs SpineDocument12 pagesHip Vs Spinevaibhav gowdaNo ratings yet
- Neck Hammock v. Does - ComplaintDocument89 pagesNeck Hammock v. Does - ComplaintSarah BursteinNo ratings yet
- Cervical Spondylosis HistoryDocument2 pagesCervical Spondylosis HistorycarinasheliapNo ratings yet
- Spondylosis, Cervical and LumbarDocument1 pageSpondylosis, Cervical and LumbarLuis HerreraNo ratings yet
- Traction NursingDocument75 pagesTraction NursingSujith KuttanNo ratings yet
- Carolyn O'Neal v. Fremont County Board of Commissioners, Et Al.Document40 pagesCarolyn O'Neal v. Fremont County Board of Commissioners, Et Al.Michael_Lee_RobertsNo ratings yet
- Tentative Ruling in Florencio Munguia v. County of San BernardinoDocument9 pagesTentative Ruling in Florencio Munguia v. County of San BernardinoBeau YarbroughNo ratings yet
- Late Responses: Table 4-1. Late Responses: F Response and H Reflex F Response H ReflexDocument11 pagesLate Responses: Table 4-1. Late Responses: F Response and H Reflex F Response H ReflexIzabella MihályNo ratings yet
- Bogduk 2009Document3 pagesBogduk 2009Borys100% (1)
- Cervical Disc ProlapseDocument27 pagesCervical Disc ProlapseMaroofAliNo ratings yet
- Neck Pain and Lower Back Pain. Med Clin N Am. 2019.Document14 pagesNeck Pain and Lower Back Pain. Med Clin N Am. 2019.Jose Fernando Diez100% (1)
- What Is Physiatry 2022Document2 pagesWhat Is Physiatry 2022Victoria GonzalezNo ratings yet
- Rios Vazquez v. SHHS, 45 F.3d 424, 1st Cir. (1995)Document6 pagesRios Vazquez v. SHHS, 45 F.3d 424, 1st Cir. (1995)Scribd Government DocsNo ratings yet
- Cervical RadiculopathyDocument7 pagesCervical Radiculopathyrhymescsf100% (1)
- Herniated Nucleus Pulposus TreatmentDocument19 pagesHerniated Nucleus Pulposus Treatmentvicky174No ratings yet
- Oscar Montalvo v. Secretary of Health and Human Services, 960 F.2d 143, 1st Cir. (1992)Document6 pagesOscar Montalvo v. Secretary of Health and Human Services, 960 F.2d 143, 1st Cir. (1992)Scribd Government DocsNo ratings yet
- Differential Diagnosis of Cervicobrachial PainDocument11 pagesDifferential Diagnosis of Cervicobrachial PainpuchioNo ratings yet
- Guidelines For Evaluation and Management of LBPDocument482 pagesGuidelines For Evaluation and Management of LBPShashi JainNo ratings yet
- Peripheral Neuropathy: Evaluation and Differential DiagnosisDocument8 pagesPeripheral Neuropathy: Evaluation and Differential DiagnosisBintu Searching-FriendNo ratings yet