Download as pdf or txt
You might also like
- Informative Oral PresentationDocument3 pagesInformative Oral Presentationapi-303321512No ratings yet
- Professional Practice - Lippincott'sDocument91 pagesProfessional Practice - Lippincott'sJincy JoseNo ratings yet
- 2003NBDE 1 ExplanationsDocument110 pages2003NBDE 1 Explanationsfly_jfz100% (3)
- ps04 2006 Recommendations For The Post Anaesthesia Recovery RoomDocument6 pagesps04 2006 Recommendations For The Post Anaesthesia Recovery RoomJane KoNo ratings yet
- Abdomen and ThoraxDocument7 pagesAbdomen and ThoraxchadNo ratings yet
- Analgesia For Iliac Crest Bone GraftDocument9 pagesAnalgesia For Iliac Crest Bone GraftDominik Chirito PastorNo ratings yet
- 239 Transversus Abdominus Plane BlockDocument12 pages239 Transversus Abdominus Plane BlockRamesh lal ShahNo ratings yet
- Transversus Abdominis Plane (Tap) BlockDocument6 pagesTransversus Abdominis Plane (Tap) BlockSuresh KumarNo ratings yet
- Peretul AbdominalDocument9 pagesPeretul AbdominalBotond LukacsNo ratings yet
- Hayes 2015Document10 pagesHayes 2015dyahpuspardaniNo ratings yet
- GRSANA - Lec5 Temporal Fossa, Infratemporal Fossa, and TMJ - WongDocument9 pagesGRSANA - Lec5 Temporal Fossa, Infratemporal Fossa, and TMJ - WongRainier Raul Echipare100% (1)
- Parks 1976Document12 pagesParks 1976EunikeSetiyantoWijayaNo ratings yet
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument18 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherApridey ParindingNo ratings yet
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument18 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherApridey ParindingNo ratings yet
- Miller2018 PDFDocument15 pagesMiller2018 PDFAnis BergerNo ratings yet
- Nerve Blocks of The Anterior AbdominalDocument5 pagesNerve Blocks of The Anterior AbdominalBinas GirmaNo ratings yet
- Musl of CHESTDocument4 pagesMusl of CHESTVrushab ManojNo ratings yet
- Anatomy of The Thoracic Wall, Pulmonary Cavities, and MediastinumDocument26 pagesAnatomy of The Thoracic Wall, Pulmonary Cavities, and Mediastinumearly intervention centre thudiylu trerNo ratings yet
- TAP Block 2Document5 pagesTAP Block 2Parvathy R NairNo ratings yet
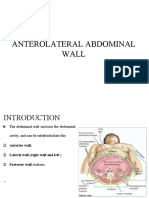
- Anterolateral Abdominal WallDocument22 pagesAnterolateral Abdominal Wallvalerie obehiNo ratings yet
- Anatomia y Fisiologia Del DiafragmaDocument11 pagesAnatomia y Fisiologia Del Diafragmaflechudo1235408No ratings yet
- Nervio Trigemino Articulo 2019Document8 pagesNervio Trigemino Articulo 2019Wendy Alejandra NarvaezNo ratings yet
- BOOK II ... Surgical Department Book Part II 2024Document291 pagesBOOK II ... Surgical Department Book Part II 2024alexandermason2003No ratings yet
- Abdominal Wall Sonography: A Pictorial ReviewDocument14 pagesAbdominal Wall Sonography: A Pictorial Reviewhypebeast dopeNo ratings yet
- Structures of The Spinal CanalDocument7 pagesStructures of The Spinal CanalveronicalovirgenNo ratings yet
- Thoracic and Lumbar Sympathetic Nerve Block and NeurolysisDocument12 pagesThoracic and Lumbar Sympathetic Nerve Block and NeurolysisNitin HayaranNo ratings yet
- Snell AbdomenDocument43 pagesSnell AbdomenBenNo ratings yet
- 10.1007@s40140 019 00333 0Document10 pages10.1007@s40140 019 00333 0TM AnNo ratings yet
- Spinal Anesthesia - Technique - UpToDateDocument37 pagesSpinal Anesthesia - Technique - UpToDateSamir Perez CasadiegoNo ratings yet
- Chapter 2 Maternal AnatomyDocument9 pagesChapter 2 Maternal AnatomyRem Alfelor100% (2)
- BMS301, L11, Histology, Structure of White Matter of Spinal CordDocument38 pagesBMS301, L11, Histology, Structure of White Matter of Spinal Cordkareemosama9916No ratings yet
- Muscles of UL: Pectoral Region General Instructions For Dissection BreastDocument46 pagesMuscles of UL: Pectoral Region General Instructions For Dissection BreastABc abcNo ratings yet
- Louka S 2006Document6 pagesLouka S 2006Dr LAUMONERIENo ratings yet
- Anterior Abdominal Wall SonaliiiDocument36 pagesAnterior Abdominal Wall Sonaliiisonali swainNo ratings yet
- Anatomy, Head and Neck, Temporoparietal Fascia - StatPearls - NCBI BookshelfDocument3 pagesAnatomy, Head and Neck, Temporoparietal Fascia - StatPearls - NCBI BookshelfPranave P100% (1)
- P ('t':'3', 'I':'3053926525') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document14 pagesP ('t':'3', 'I':'3053926525') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Ni Wayan Ana PsNo ratings yet
- Continuum Spinal Cord AnatomyDocument25 pagesContinuum Spinal Cord AnatomyslojnotakNo ratings yet
- Placing A Lumbar Epidural CatheterDocument4 pagesPlacing A Lumbar Epidural CatheterGus LionsNo ratings yet
- AnatomyDocument5 pagesAnatomyBRENDA VALDEZ 190291No ratings yet
- Torso - Thorax Overview - Cherchi - 1999Document17 pagesTorso - Thorax Overview - Cherchi - 1999clubstarNo ratings yet
- Radius and Ulna: PPP Jazlan Bin Mohamad (Posbasic Ortho 1/2018)Document17 pagesRadius and Ulna: PPP Jazlan Bin Mohamad (Posbasic Ortho 1/2018)Jazlan MohamadNo ratings yet
- Hernia Inguinal 1, Anatomia, SCNA 2018Document15 pagesHernia Inguinal 1, Anatomia, SCNA 2018Angie Cristina Hoyos EcheverriNo ratings yet
- Gastro Anatomy: (1) Abdominal CavityDocument6 pagesGastro Anatomy: (1) Abdominal CavityZhenNo ratings yet
- riccardo,+OP03845 IJAE 2019 2 176-181 20191122 0833Document6 pagesriccardo,+OP03845 IJAE 2019 2 176-181 20191122 0833researchnnnnNo ratings yet
- Ultrasound-Guided Fascial PlaneDocument19 pagesUltrasound-Guided Fascial PlaneEnano Narigudo TresNo ratings yet
- Anatomy of The Abdomen and PelvisDocument20 pagesAnatomy of The Abdomen and PelvishanifsharNo ratings yet
- Oxford Handbooks Online: Central Nervous System Pain PathwaysDocument34 pagesOxford Handbooks Online: Central Nervous System Pain Pathwayssukses belajarNo ratings yet
- Abdominal Wall Nerve BlocksDocument49 pagesAbdominal Wall Nerve BlocksTaupik RahmanNo ratings yet
- Anatomy of Larynx Lecture 7Document21 pagesAnatomy of Larynx Lecture 7sallykamareddine100% (1)
- 8 Surgical Anatomy of TMJDocument11 pages8 Surgical Anatomy of TMJArchanaShenoyNo ratings yet
- Anatomy and Localization of Spinal Cord DisordersDocument23 pagesAnatomy and Localization of Spinal Cord DisordersMichael RojasNo ratings yet
- Ecr2016 C-0757Document28 pagesEcr2016 C-0757mloureiro17No ratings yet
- Anatomy - Upper LimbDocument9 pagesAnatomy - Upper LimbjainilNo ratings yet
- 263 Lumbar Plexus Block - Psoas Compartment BlockDocument9 pages263 Lumbar Plexus Block - Psoas Compartment Blockarif AjiNo ratings yet
- 2005 10 24 Review AnswersDocument30 pages2005 10 24 Review Answersaip1000No ratings yet
- The Mandibular Nerve: The Anatomy of Nerve Injury and EntrapmentDocument18 pagesThe Mandibular Nerve: The Anatomy of Nerve Injury and EntrapmentEXPRESSIONS A KEY TO SOULNo ratings yet
- Acb 49 213Document4 pagesAcb 49 213Haru SahaNo ratings yet
- Ear ProsthesisDocument16 pagesEar ProsthesisMohammed HassanNo ratings yet
- Thoracic and Coracoid Arteries In Two Families of Birds, Columbidae and HirundinidaeFrom EverandThoracic and Coracoid Arteries In Two Families of Birds, Columbidae and HirundinidaeNo ratings yet
- High Resolution and High Definition Anorectal ManometryFrom EverandHigh Resolution and High Definition Anorectal ManometryMassimo BelliniNo ratings yet
- Practices of Anorectal SurgeryFrom EverandPractices of Anorectal SurgeryDong Keun LeeNo ratings yet
- Neuromodulation in Headache and Facial Pain Management: Principles, Rationale and Clinical DataFrom EverandNeuromodulation in Headache and Facial Pain Management: Principles, Rationale and Clinical DataGiorgio LambruNo ratings yet
- 07.03.40 Neonatal Pediatric Arterial PunctureDocument7 pages07.03.40 Neonatal Pediatric Arterial PunctureFariz A JaNo ratings yet
- Most Requested Items/locations: Emergency Department Elevators Pedway Path Welcome CenterDocument2 pagesMost Requested Items/locations: Emergency Department Elevators Pedway Path Welcome CenterTERRENCENo ratings yet
- The National Birth Center Study IIDocument12 pagesThe National Birth Center Study IIapi-38108107No ratings yet
- Laws and Regulations Affecting NursingDocument4 pagesLaws and Regulations Affecting Nursingpolo24No ratings yet
- Spinal Anaesthesia - Wikipedia, The Free EncyclopediaDocument4 pagesSpinal Anaesthesia - Wikipedia, The Free EncyclopediafujiNo ratings yet
- Resume Brittany Gee GanDocument3 pagesResume Brittany Gee GanSlahuddin KhanNo ratings yet
- Fibrocystic Breast ChangesDocument11 pagesFibrocystic Breast ChangesDeasy MirayashiNo ratings yet
- Evelina BalzhykDocument1 pageEvelina Balzhykapi-509642710No ratings yet
- QwewqeDocument1 pageQwewqeMuneeb ShahzadNo ratings yet
- Graduate School 3 Trimester, Academic Year 2020-2021: St. Paul University Philippines Tuguegarao City, Cagayan 3500Document3 pagesGraduate School 3 Trimester, Academic Year 2020-2021: St. Paul University Philippines Tuguegarao City, Cagayan 3500Danica Lorine Robino TaguinodNo ratings yet
- Oxytocin, Dinoprostone, Cefuroxime Drug StudyDocument3 pagesOxytocin, Dinoprostone, Cefuroxime Drug StudyMary Shane MoraldeNo ratings yet
- Prone Vs Supine PCNLDocument20 pagesProne Vs Supine PCNLvera182sjNo ratings yet
- Health Management Information SystemDocument6 pagesHealth Management Information SystemNimco gureeyNo ratings yet
- Sample Pages of Koncpt 20 Authors 2nd EditionDocument25 pagesSample Pages of Koncpt 20 Authors 2nd EditionvkNo ratings yet
- Implementing Optimal Team-Based Care To Reduce Clinician BurnoutDocument13 pagesImplementing Optimal Team-Based Care To Reduce Clinician BurnoutfreteerNo ratings yet
- A Comprehensive Scheme of Health Manpower Development For NepalDocument6 pagesA Comprehensive Scheme of Health Manpower Development For NepalKhadga ShresthaNo ratings yet
- English Correct Network Update September 2019Document151 pagesEnglish Correct Network Update September 2019samar RamadanNo ratings yet
- Vulvovaginitis in CowDocument3 pagesVulvovaginitis in CowSbastian PratamaNo ratings yet
- Paediatric Physician Training - FAQ 2017Document4 pagesPaediatric Physician Training - FAQ 2017DrSajid BuzdarNo ratings yet
- CekDocument3 pagesCekNasrudin EfendiNo ratings yet
- Guidelines On Male InfertilityDocument60 pagesGuidelines On Male InfertilityYane Aulia YasminNo ratings yet
- The Beacon - March 22, 2012Document18 pagesThe Beacon - March 22, 2012schaffnerpubNo ratings yet
- Scheuermann's Disease: A Review: IncidenceDocument5 pagesScheuermann's Disease: A Review: IncidenceFlorian AlexandruNo ratings yet
- COMPARISON BETWEEN ULTRASONOGRAPHIC AND CLINICAL FINDINGS IN 43 DOGS WITH GB MUCOCELEchoi2013Document6 pagesCOMPARISON BETWEEN ULTRASONOGRAPHIC AND CLINICAL FINDINGS IN 43 DOGS WITH GB MUCOCELEchoi2013Thaís ChouinNo ratings yet
- Sri Siddhartha Medical College - Tumkur Provisional List of PG Degree / Diploma Students Admitted During 2011-12 Academic YearDocument23 pagesSri Siddhartha Medical College - Tumkur Provisional List of PG Degree / Diploma Students Admitted During 2011-12 Academic YearAnonymous Ub9nEDlNo ratings yet
- CHN1 Lec Session #19 SASDocument8 pagesCHN1 Lec Session #19 SASRetiza EllaNo ratings yet
- WtArGuNkER McCrea VmacncirteyaDocument83 pagesWtArGuNkER McCrea VmacncirteyaJk McCreaNo ratings yet