Download as pdf or txt
You might also like
- Connectors in FPDDocument3 pagesConnectors in FPDSatya AsatyaNo ratings yet
- Properties of Dental MaterialsDocument8 pagesProperties of Dental MaterialsSatya Asatya100% (1)
- OxygenationDocument57 pagesOxygenationscent0730100% (3)
- Expt 2-Planaria 2014Document9 pagesExpt 2-Planaria 2014Sarah HarringtonNo ratings yet
- ISSA Personal Trainer Certification Course Quizzes Ninth EditionDocument35 pagesISSA Personal Trainer Certification Course Quizzes Ninth Editionscorpion99938% (8)
- Mandibular Rest Position and ElectricalDocument6 pagesMandibular Rest Position and ElectricalPaula GuerreroNo ratings yet
- BCR 1976Document15 pagesBCR 1976Tia YuandaNo ratings yet
- 4 The Upper Cervical AdjustmentDocument19 pages4 The Upper Cervical Adjustmentanibalpomi9351100% (1)
- Functional Occlusal Forces - An Investigation by Telemetry PDFDocument8 pagesFunctional Occlusal Forces - An Investigation by Telemetry PDFZardasht NajmadineNo ratings yet
- Some Physiologic Consideration of Centric and Other Jaw RelationsDocument12 pagesSome Physiologic Consideration of Centric and Other Jaw RelationsMartha Lia Castaño EcheverryNo ratings yet
- tmp5092 TMPDocument8 pagestmp5092 TMPFrontiersNo ratings yet
- Artificial Gravity Head Movements DuringDocument8 pagesArtificial Gravity Head Movements Duringkanchan7choubeyNo ratings yet
- Pap Athanasiou 2014Document48 pagesPap Athanasiou 2014Caio LeônidasNo ratings yet
- 1179 FullDocument17 pages1179 FullSamsung UserNo ratings yet
- ThesisDocument51 pagesThesisIsabella MariaNo ratings yet
- PNAS 2010 Breshears 1011949107Document6 pagesPNAS 2010 Breshears 1011949107vlmwarrenNo ratings yet
- The Australian Journal of Physiotherapy: Electrodiagnostic TechniquesDocument4 pagesThe Australian Journal of Physiotherapy: Electrodiagnostic TechniquesumangNo ratings yet
- Multimodal Intraoperative Monitoring 1017 Cases - Spine 2007Document10 pagesMultimodal Intraoperative Monitoring 1017 Cases - Spine 2007manuel valeraNo ratings yet
- Emg Conceptos - Nerve Conduction StudiesDocument23 pagesEmg Conceptos - Nerve Conduction StudiesDeborah SalinasNo ratings yet
- Kam 2018Document11 pagesKam 2018JT DanielsNo ratings yet
- Ecomiografia Funzionale - Analisi Di Spessori EcostrutturaDocument8 pagesEcomiografia Funzionale - Analisi Di Spessori EcostrutturaDavideSilvestriNo ratings yet
- Graded Activation of The Intrinsic Laryngeal Muscles For Vocal Fold PosturingDocument7 pagesGraded Activation of The Intrinsic Laryngeal Muscles For Vocal Fold PosturingDaniel AlonsoNo ratings yet
- Neuromonitoring SyllabusDocument9 pagesNeuromonitoring SyllabuspablocotanNo ratings yet
- Spinal Cord Stimulation in Chronic Pain ManagementDocument10 pagesSpinal Cord Stimulation in Chronic Pain ManagementnaimNo ratings yet
- Altered Sensorimotor Integration in Parkinson's DiseaseDocument11 pagesAltered Sensorimotor Integration in Parkinson's Diseaseadit020586No ratings yet
- Clinical Neurophysiology: Derek M. Miller, James F. Baker, W. Zev RymerDocument9 pagesClinical Neurophysiology: Derek M. Miller, James F. Baker, W. Zev RymerMiguelNo ratings yet
- Neuropathies - EMG 2007 PDFDocument312 pagesNeuropathies - EMG 2007 PDFSusanaBravoDueñas100% (2)
- Development and Evaluation of A Bio Ion Measureme - 2013 - Journal of AcupuncturDocument9 pagesDevelopment and Evaluation of A Bio Ion Measureme - 2013 - Journal of AcupuncturMatias DamiánNo ratings yet
- Yong-Hyun 2011Document7 pagesYong-Hyun 2011GorkaBuesaNo ratings yet
- Spinal and Supraspinal Effects of Activity in Ligament AfferentsDocument10 pagesSpinal and Supraspinal Effects of Activity in Ligament AfferentsItai IzhakNo ratings yet
- Cuddon - Electrophysiology in Neuromuscular Disease - 2002Document32 pagesCuddon - Electrophysiology in Neuromuscular Disease - 2002paula gonzalezNo ratings yet
- Journal Pre-Proof: Clinical BiomechanicsDocument34 pagesJournal Pre-Proof: Clinical BiomechanicsZouhour MiladiNo ratings yet
- Electrophysiology of LarynxDocument12 pagesElectrophysiology of LarynxNehasish SahuNo ratings yet
- Double Crush SyndromeDocument6 pagesDouble Crush SyndromemesrickNo ratings yet
- Tutorial 5. Nov 6 - Lajoie&Al1996Document8 pagesTutorial 5. Nov 6 - Lajoie&Al1996jaxter2002No ratings yet
- Capacitive Aspects of Diagnosis by Oriental Traditional Medicine. Regard On Electrography Through ElectroluminiscenceDocument6 pagesCapacitive Aspects of Diagnosis by Oriental Traditional Medicine. Regard On Electrography Through Electroluminiscencemamulasioan9675No ratings yet
- 3 Chiropractic Subluxation IndicatorsDocument46 pages3 Chiropractic Subluxation IndicatorsMário Ornelas100% (3)
- Kaklo RegionasDocument13 pagesKaklo RegionasVizaNo ratings yet
- Sagittal Spine Posture Assessment: Feasibility of A Protocol Based On Intersegmental MomentsDocument5 pagesSagittal Spine Posture Assessment: Feasibility of A Protocol Based On Intersegmental MomentsVizaNo ratings yet
- Laryngeal ElectromyographyDocument21 pagesLaryngeal Electromyographyapi-19500641No ratings yet
- (2000) Kiernan MK. Multiple Measures of Axonal Excitability - A New Approach in Clinical TestingDocument11 pages(2000) Kiernan MK. Multiple Measures of Axonal Excitability - A New Approach in Clinical TestingLucía del ValleNo ratings yet
- Integração Sensoriomotora No Controle PosturalDocument23 pagesIntegração Sensoriomotora No Controle PosturalcursosNo ratings yet
- Peterka - 2002 - J NeurophysDocument23 pagesPeterka - 2002 - J NeurophysKarem TuctoNo ratings yet
- CV4 EfectDocument21 pagesCV4 EfectNicole HermosillaNo ratings yet
- 1 s2.0 S1877065715000779 MainDocument7 pages1 s2.0 S1877065715000779 Mainxian karachiNo ratings yet
- Electromiografic Effects of Fatigue and Task RepetitionDocument15 pagesElectromiografic Effects of Fatigue and Task RepetitionAlberto BeskowNo ratings yet
- ADIE 2011 - Pulsed Electromagnetic Field Stimulation For Acute Tibial Shaft FracturesDocument8 pagesADIE 2011 - Pulsed Electromagnetic Field Stimulation For Acute Tibial Shaft FracturesMauricio ZeniNo ratings yet
- TMP 9 C82Document7 pagesTMP 9 C82FrontiersNo ratings yet
- Electromyography and Its Applications in OrthodonticsDocument5 pagesElectromyography and Its Applications in Orthodonticsmehdi chahrourNo ratings yet
- Kinematics of Rotational Mobilisation of The Lumbar SpineDocument8 pagesKinematics of Rotational Mobilisation of The Lumbar SpinePablo RdzNo ratings yet
- 2016 Effect of Laser Acupuncture On Heart Rate Variability of Nonpatients and Patients With Spinal Cord InjuryDocument2 pages2016 Effect of Laser Acupuncture On Heart Rate Variability of Nonpatients and Patients With Spinal Cord Injuryenfermeironilson6321No ratings yet
- SD MiofascialDocument5 pagesSD MiofascialMarGarciaNo ratings yet
- EMG For OpthalmographyDocument30 pagesEMG For OpthalmographyhurahuriNo ratings yet
- Spinal Myo After InjuryDocument12 pagesSpinal Myo After InjuryVincentius Michael WilliantoNo ratings yet
- NeedleEMG Fundamentals (David Shapiro)Document36 pagesNeedleEMG Fundamentals (David Shapiro)Shauki AliNo ratings yet
- Sensorimotor Integracion in Human Postural ControlDocument23 pagesSensorimotor Integracion in Human Postural ControlDaniela Nayem Fuentes MarínNo ratings yet
- Force-Controlled Biting Alters Postural Control in BipedalDocument13 pagesForce-Controlled Biting Alters Postural Control in BipedalSamNo ratings yet
- Infleunce of Group Function Canine Guidance On Elevator MuscleDocument8 pagesInfleunce of Group Function Canine Guidance On Elevator MuscleHossam BarghashNo ratings yet
- Chulbae 1996Document15 pagesChulbae 1996M4shroomNo ratings yet
- The Role of The Dorsal Anterior Insula in Ecstatic Sensation Revealed by Direct Electrical Brain Stimulation F Bartolomei S Lagarde D Scavarda R Carron C G Benar F Picard Full ChapterDocument42 pagesThe Role of The Dorsal Anterior Insula in Ecstatic Sensation Revealed by Direct Electrical Brain Stimulation F Bartolomei S Lagarde D Scavarda R Carron C G Benar F Picard Full Chaptersally.rogers984100% (9)
- Dorsal RhizotomyDocument13 pagesDorsal RhizotomyAiman MaidanNo ratings yet
- Position Paper For Orthogonally-Based Upper Cervical Chiropractic CareDocument11 pagesPosition Paper For Orthogonally-Based Upper Cervical Chiropractic CareRodrigo LimaNo ratings yet
- Neurophysiological Effects of Spinal ManipulationDocument15 pagesNeurophysiological Effects of Spinal ManipulationBojan AnticNo ratings yet
- Pharmacology of Medical Cannabis - Ruhul AminDocument11 pagesPharmacology of Medical Cannabis - Ruhul AminjuciarampNo ratings yet
- 10 11607@ijp 6726Document12 pages10 11607@ijp 6726Satya AsatyaNo ratings yet
- DM Second Internal MarksDocument2 pagesDM Second Internal MarksSatya AsatyaNo ratings yet
- Histology of OsseointegrationDocument3 pagesHistology of OsseointegrationSatya AsatyaNo ratings yet
- Recognition MDS ProsthoDocument16 pagesRecognition MDS ProsthoSatya AsatyaNo ratings yet
- Die-Materials classEDITDocument45 pagesDie-Materials classEDITSatya AsatyaNo ratings yet
- Department EquipmentDocument4 pagesDepartment EquipmentSatya AsatyaNo ratings yet
- Adobe Scan 21 Jan 2021Document2 pagesAdobe Scan 21 Jan 2021Satya AsatyaNo ratings yet
- ANSWERS Cont.: QuestionsDocument3 pagesANSWERS Cont.: QuestionsSatya AsatyaNo ratings yet
- Self Study Report: 1 Cycle of AccreditationDocument120 pagesSelf Study Report: 1 Cycle of AccreditationSatya AsatyaNo ratings yet
- AP PG - 30 - Microbiology - AnswersDocument9 pagesAP PG - 30 - Microbiology - AnswersSatya AsatyaNo ratings yet
- Dental Materials - Key: Guidance Program - 2017 Toppers Guidance ClassesDocument2 pagesDental Materials - Key: Guidance Program - 2017 Toppers Guidance ClassesSatya AsatyaNo ratings yet
- Q.P. CODE:421-NR/402-OR: Dental MaterialsDocument41 pagesQ.P. CODE:421-NR/402-OR: Dental MaterialsSatya AsatyaNo ratings yet
- Management of Hypertensive Elderly in Clinical Dentistry: Patcharaphol Samnieng, Kantapong PloydanaiDocument9 pagesManagement of Hypertensive Elderly in Clinical Dentistry: Patcharaphol Samnieng, Kantapong PloydanaiSatya AsatyaNo ratings yet
- 17th Session Grand Test-2 Qus. 26-Feb-2017Document10 pages17th Session Grand Test-2 Qus. 26-Feb-2017Satya AsatyaNo ratings yet
- Dentin Bonding AgentsDocument35 pagesDentin Bonding AgentsSatya Asatya0% (1)
- ANSWERS Cont New 2Document15 pagesANSWERS Cont New 2Satya AsatyaNo ratings yet
- 4Th Lec. Preparing Master Casts For Duplication: July 2015Document8 pages4Th Lec. Preparing Master Casts For Duplication: July 2015Satya AsatyaNo ratings yet
- 1.notification For Recruitment of CAS Specialists & DAS Under APVVP PDFDocument2 pages1.notification For Recruitment of CAS Specialists & DAS Under APVVP PDFSatya AsatyaNo ratings yet
- Bio Materials For Dental Implants An OverviewDocument13 pagesBio Materials For Dental Implants An OverviewSatya AsatyaNo ratings yet
- Implant Biomaterials: A Comprehensive Review: January 2015Document8 pagesImplant Biomaterials: A Comprehensive Review: January 2015Satya AsatyaNo ratings yet
- 0922-ENG-EU-5300 Pro-210285X6P-20230822Document2 pages0922-ENG-EU-5300 Pro-210285X6P-20230822bikouvoNo ratings yet
- Her Best Friend's LoverDocument2 pagesHer Best Friend's LoverTess Javelosa JimeneaNo ratings yet
- Report On Stress - NymaDocument26 pagesReport On Stress - Nymannaima100% (1)
- OTC Medication For Common Gastrointestinal ProblemsDocument3 pagesOTC Medication For Common Gastrointestinal Problemsnishanthprasad24No ratings yet
- Hematemesis and Melena - ChapterDocument6 pagesHematemesis and Melena - ChapterNuryantriPuspitasariNo ratings yet
- Exercise and Sport Sciences Reviews PDFDocument2 pagesExercise and Sport Sciences Reviews PDFMatt100% (1)
- S V ExercisesDocument2 pagesS V ExercisesAljake Llanes SalesNo ratings yet
- Oxalate Ion in GuavaDocument9 pagesOxalate Ion in GuavaCiandeb GracianoNo ratings yet
- DrugDocument6 pagesDrugRose Ann MirafloresNo ratings yet
- Plant Nutrition & TransportDocument21 pagesPlant Nutrition & TransportKim-Elaine Pohatu100% (1)
- Surviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedDocument32 pagesSurviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedAdli Wafi Jabbar100% (1)
- Factors Affecting Body TemperatureDocument3 pagesFactors Affecting Body TemperaturenvhnygNo ratings yet
- 4BI0 1B Que 20130523Document28 pages4BI0 1B Que 20130523traphouse982No ratings yet
- Lab 4 Microbial MetabolismDocument21 pagesLab 4 Microbial MetabolismEzgi TanılNo ratings yet
- 1316323815-Fabius GS ManualDocument312 pages1316323815-Fabius GS ManualJose De Abreu100% (1)
- Madison Solomon ResumeDocument2 pagesMadison Solomon Resumeapi-321571692No ratings yet
- Blood and Clotting MechanismDocument63 pagesBlood and Clotting MechanismRahul PandeyNo ratings yet
- The Cardiovascular System: Jomar P. Ronquillo, RN, Manc Anatomy and Physiology InstructorDocument133 pagesThe Cardiovascular System: Jomar P. Ronquillo, RN, Manc Anatomy and Physiology InstructorHypothalamus1No ratings yet
- AnthropometricDocument11 pagesAnthropometricdrrebaNo ratings yet
- Influence of Aerobic Exercise Training On Cardiovascular and Endocrine Inflammatory Biomarkers in Hypertensive Postmenopausal WomenDocument7 pagesInfluence of Aerobic Exercise Training On Cardiovascular and Endocrine Inflammatory Biomarkers in Hypertensive Postmenopausal WomenNemo SecretNo ratings yet
- Cardiopulmonary Bypass: DR R Sri Devi Assistant ProfessorDocument36 pagesCardiopulmonary Bypass: DR R Sri Devi Assistant ProfessorSanthi Swetha PudhotaNo ratings yet
- (New & Improved) TDEE Calculator (Insanely Accurate)Document4 pages(New & Improved) TDEE Calculator (Insanely Accurate)Karin SasuNo ratings yet
- Neurociencia Clínica AfectivaDocument5 pagesNeurociencia Clínica AfectivaKimum KimúmNo ratings yet
- The Largest Organ of The Body IsDocument10 pagesThe Largest Organ of The Body IsDip Ayan MNo ratings yet
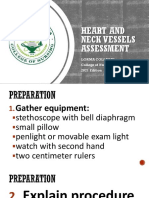
- 8 Heart and Neck Vessels AssessmentDocument61 pages8 Heart and Neck Vessels AssessmentPrincess VanquirayNo ratings yet
- Cell Biology Part IDocument66 pagesCell Biology Part IdesaishantiNo ratings yet
- Neuromythology of EINSTEIN BriainDocument5 pagesNeuromythology of EINSTEIN BriainrorozainosNo ratings yet