Professional Documents
Culture Documents
Articles: Cilostazol: Treatment of Intermittent Claudication
Articles: Cilostazol: Treatment of Intermittent Claudication
Uploaded by
Shandy JonnerOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Articles: Cilostazol: Treatment of Intermittent Claudication
Articles: Cilostazol: Treatment of Intermittent Claudication
Uploaded by
Shandy JonnerCopyright:
Available Formats
ARTICLES
Formulary Forum
Cilostazol: Treatment of Intermittent Claudication
Muredach P Reilly and Emile R Mohler III
OBJECTIVE:
To review the pharmacology and clinical utility of cilostazol, an antiplatelet and vasodilator agent approved for the
management of intermittent claudication.
DATA SOURCES: Primary literature on cilostazol was identified from a comprehensive MEDLINE literature search (1980–February
2000). Selected meeting abstracts and manufacturer literature were also used as source material. Indexing terms included
cilostazol, intermittent claudication, platelet inhibitors, and restenosis.
STUDY SELECTION: Human clinical, pharmacokinetic and randomized comparative trials performed in the US and Asia were
reviewed. Selected in vitro, ex vivo, and animal studies were evaluated when human data were not available.
DATA SYNTHESIS: Intermittent claudication, defined as reproducible discomfort of a muscle group induced by exercise and relieved
by rest, is the most common clinical manifestation of peripheral arterial disease (PAD). Cilostazol, a specific inhibitor of cyclic
adenosine monophosphate phosphodiesterase in platelets and vascular smooth-muscle cells, is a potent antiplatelet agent and
vasodilator that reduces vascular proliferation and has lipid-lowering effects in vivo. Recent multicenter, randomized, placebo-
controlled trials have led to approval of cilostazol by the Food and Drug Administration for relief of intermittent claudication in patients
with stable PAD. Cilostazol doubled walking distances and improved quality of life compared with placebo in these studies. One trial
found that cilostazol was more effective than pentoxifylline, the only alternative pharmacologic therapy for claudication. Although
frequent (~50%) minor adverse effects, including headache, diarrhea, and palpitations, may occur in clinical practice, cilostazol has
not been associated with major adverse events or increased mortality. Small, nonblind studies suggest that cilostazol may prove
useful in preventing thrombosis and restenosis following percutaneous coronary interventions, although these remain unlabeled
uses.
CONCLUSIONS: The unique combination of antiplatelet, vasodilatory, and antiproliferative effects of cilostazol appear to make it an
attractive agent for use in patients with PAD. Clinical trials demonstrating a significant improvement in walking distances with
cilostazol therapy suggest that it will be an important tool in improving symptoms and quality of life in patients with intermittent
claudication.
KEY WORDS: cilostazol, intermittent claudication, peripheral arterial disease, antiplatelet, vasodilator, restenosis.
Ann Pharmacother 2001;35:48-56.
ACPE UNIVERSAL PROGRAM NUMBER: 407-000-01-001-H01
ntermittent claudication is defined as reproducible dis- (PAD) is by far the most common cause of intermittent
Ilieved
comfort of a muscle group induced by exercise and re-
by rest. Symptoms develop because of reduced blood
claudication. However, up to 40% of people with PAD are
asymptomatic, and many patients with claudication do not
supply, which fails to meet the metabolic demands of the seek medical attention.1 The clinical importance of PAD,
muscle group. Peripheral arterial obstructive disease which often goes unrecognized and may affect up to 5% of
elderly patients in the US, is highlighted by an associated
sixfold increased risk of death from cardiac and cere-
Author information provided at the end of the text. brovascular causes. Improved detection of PAD through
Cilostazol (Pletal, Otsuka America Pharmaceutical). more widespread use of the ankle–brachial index (ABI;
48 ■ The Annals of Pharmacotherapy ■ 2001 January, Volume 35 www.theannals.com
Downloaded from aop.sagepub.com by guest on August 12, 2015
Doppler-determined ankle/arm blood pressure ratio of hanced protein kinase A– dependent substrate phosphory-
<0.9 is diagnostic of PAD) and more aggressive secondary lation and sequestration of calcium.21 Endothelial cells,
preventive measures are expected to improve cardiovascu- probably through the release of prostacyclin, an activator
lar outcomes in this population. of adenylate cyclase, enhance the antiplatelet activity of
Intermittent claudication is associated with a reduced cilostazol in vitro.18 This suggests that increased sensitivity
quality of life, and there are limited treatment options for to adenylate cyclase stimuli may contribute to the anti-
this often debilitating symptom.1,2 Cilostazol, an agent em- platelet effect of cilostazol at the blood vessel wall.
ployed in the treatment of PAD in Japan for over a decade, In a double-blind, crossover study19 of three antiplatelet
was recently approved by the Food and Drug Administra- agents, cilostazol was a more potent inhibitor of adenosine
tion (FDA) for the management of intermittent claudica- diphosphate, collagen, and arachidonic acid–induced plate-
tion.3-7 Although its precise mechanism of action is not ful- let aggregation ex vivo than aspirin or ticlopidine.17 Cilo-
ly understood, cilostazol is a type-III phosphodiesterase in- stazol suppressed thrombin-induced platelet calcium in-
hibitor with antiplatelet, vasodilatory, and antiproliferative creases, thromboxane A2 formation, and platelet factor- 4
actions.8-10 Preliminary clinical data11,12 indicate that cilo- release, in addition to inhibition of platelet aggregation and
stazol may be useful as an antithrombotic and antiprolifer- agonist-induced procoagulant activity.19 Cilostazol, but not
ative agent following percutaneous coronary interventions, aspirin, also inhibits high shear-stress–induced platelet ag-
although these remain unlabeled uses. In this article, we re- gregation both in vitro and in vivo.20 Shear-stress during
view the current understanding of the pharmacology and exercise is believed to be an important mechanism of plate-
clinical utility of cilostazol. let activation at points of arterial bifurcation in patients
with atherosclerosis,22 and thus may be of particular rele-
Pharmacology vance to the reported benefits of cilostazol in patients with
intermittent claudication.
At least nine distinct genes for phosphodiesterases
(PDEs I–IX) have been identified in mammalian tis- VASODILATORY/HEMODYNAMIC EFFECTS
sues.13,14 Cyclic adenosine monophosphate (cAMP), a sec-
ond messenger generated by adenylate cyclase in response Inhibition of smooth-muscle cell PDE-III with resultant
to a variety of extracellular stimuli, undergoes degradation arterial vasodilation is thought to play a role in the benefi-
by specific phosphodiesterases. PDE-III (cyclic guanosine cial effects of cilostazol in intermittent claudication.23 In
monophosphate [GMP]–inhibited cAMP-PDE) is one of a whole organ studies,24 cilostazol produced vasodilation of
number of isozymes present in platelets, vascular smooth- human coronary and renal arteries. Intravenous infusion in
muscle cells, cardiomyocytes, and endothelial cells.8,10,14 a canine coronary reperfusion model resulted in a 25% de-
cAMP mediates many of the known agonist-induced crease in mean blood pressure at plasma concentrations
platelet inhibitory, vasodilatory and vascular
antiproliferative responses in vivo.14,15
Cilostazol (6-[4-(1-cyclohexyl-1H-tetrazol-
5-yl) butoxy]-3- 4-dihydro-2(1H)-quinolone)
is a potent, reversible PDE-III isozyme–selec-
tive inhibitor. All available evidence points to-
ward increased responsiveness to cAMP-stim-
ulating agents as its mechanism of action.8-10
Cilostazol has minimal inhibitory effects on
other PDEs, demonstrates no significant activ-
ity against calcium-calmodulin–activated PDEs,
and does not modulate the guanylate cyclase/
cyclic GMP–signaling pathway.8-10
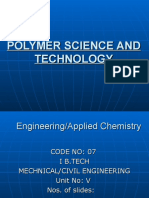
ANTIPLATELET EFFECT
Cilostazol inhibits both primary and sec-
ondary phases of platelet aggregation induced
by adenosine diphosphate, collagen, epineph-
rine, arachidonic acid, and thrombin (Figure
Figure 1. Intracellular mechanism of the antiplatelet and vasodilatory effects of cilostazol.
1).8,16-19 Platelet cAMP concentrations and Phosphodiesterase III inhibition results in increased cyclic adenosine monophosphate in
platelet inhibitory responses to agonists that response to adenylate cyclase agonists. This leads to attenuation of calcium-mediated
platelet activation and smooth-muscle cell contraction. Solid line = stimulation; broken line
stimulate adenylate cyclase were greatly in- = inhibition; AC = adenylate cyclase; ADP = adenosine diphosphate; AMP = adenosine
creased in the presence of cilostazol.8,10,20 In- monophosphate; ATP = adenosine triphosphate; DAG = diacyl glycerol; insP = inositol phos-
phate; PDE III = phosphodiesterase III; PGE2 = prostaglandin E2; PGI2 = prostacyclin; PKC
creased platelet cAMP concentrations attenu- = protein kinase C; PLC = phospholipase C; SMC = smooth muscle cell; TxA2 = thrombox-
ate activation by many agonists through en- ane A2.
www.theannals.com The Annals of Pharmacotherapy ■ 2001 January, Volume 35 ■ 49
Downloaded from aop.sagepub.com by guest on August 12, 2015
MP Reilly and ER Mohler III
similar to those in human clinical studies.25 Chronic oral metabolites found in human plasma are the dehydrocilo-
administration (6 mo) of cilostazol in human clinical trials6 stazol derivative, OPC-13015, and the monohydroxycilo-
resulted in a small increase in heart rate (<10 beats/min). stazol, OPC-13213.39-41 Both are active metabolites and
This observation, in addition to animal studies26 demon- produce threefold more and threefold less platelet inhibi-
strating a sustained hemodynamic response after two tion, respectively, than cilostazol. Cilostazol and OPC-
weeks of cilostazol therapy, suggests that cilostazol thera- 13015 are excreted in the liver; urinary excretion of OPC-
py may not induce tachyphylaxis to its pharmacologic ef- 13213 and conjugated glucuronide metabolites account for
fect. approximately 30% of the orally administered dose. The
plasma concentration (5–10 µM) produced by standard
VASCULAR EFFECTS doses of cilostazol in humans is similar to the concentra-
tion required to inhibit platelet and vascular smooth-mus-
Cilostazol inhibits vascular smooth-muscle cell PDE-III cle cell PDE-III activity in vitro and ex vivo.10,16,37 The
and attenuates proliferative response to a variety of growth pharmacologic activity of cilostazol and its metabolites
factors including platelet-derived growth factor and in- was similar in subjects with mild hepatic disease and mild
sulin-like growth factor-I.27,28 Cilostazol-induced increases to moderate renal impairment compared with healthy con-
in cAMP may inhibit cell growth by inhibition of mitogen- trols.42 Severe renal impairment increases serum cilostazol
activated protein kinase activity,28 induction of nitric oxide concentrations, but pharmacologic activity appeared to be
synthesis,29 and suppression of platelet-derived growth fac- little changed.
tor expression.30 It is noteworthy that increased PDE-III ac-
tivity and reduced cAMP concentrations have been de- Clinical Studies
scribed in studies of atherosclerosis31 and that PDE-III in-
hibitors, including cilostazol, have been shown to suppress INTERMITTENT CLAUDICATION
neointimal formation in a rat vascular injury model.15,32
The primary medical management of patients with PAD
should be aimed at reducing the risk of cardiovascular
LIPOPROTEIN EFFECTS
complications including myocardial infarction and stroke.1
Cilostazol has beneficial effects on lipid metabolism in This includes smoking cessation, antiplatelet therapy, and
patients with intermittent claudication and diabetes.5,6,33 aggressive management of lipid concentrations and other
The mechanism of this activity is unclear, but may be relat- risk factors. However, there are few medical options for
ed to cAMP-mediated enhancement of peripheral lipopro- the management of stable but sometimes debilitating inter-
tein lipase activity or attenuation of hepatic triglyceride se- mittent claudication.2 Most clinical trials have used stan-
cretion.34,35 In a randomized, placebo-controlled trial33 of dardized treadmill testing to assess the effect of interven-
189 patients with PAD, cilostazol 200 mg/d for 12 weeks tions on initial claudication distance (ICD), the walking
resulted in a 15% reduction in plasma triglycerides and distance before the onset of claudication pain, or absolute
10% increase in high-density cholesterol without a signifi- claudication distance (ACD), the total walking distance be-
cant change in low-density cholesterol. Effects appeared to fore intolerable claudication pain. Smoking cessation and
be greatest in patients with the highest baseline triglyceride supervised exercise programs can result in small but sig-
concentrations. It is unclear whether cilostazol has benefi- nificant improvement in walking distances. Pentoxifylline,
cial effects on lipid parameters when used in conjunction a rheologic agent thought to improve skeletal muscle oxy-
with aggressive lipid-lowering agents (including hydroxy- gen delivery, also increases walking distances, but the clin-
methyl gluataryl coenzyme A reductase inhibitors), which ical significance of these small improvements has been
is advocated in patients with PAD. questioned. Clinical studies9 conducted in Japanese pa-
tients with PAD suggested that cilostazol increased dermal
Pharmacokinetics blood flow and could improve claudication. A series of
multicenter clinical trials4-7,33 in the US (Table 1) has led to
Pharmacokinetic studies36-38 in humans showed that sin- FDA approval of cilostazol for the relief of intermittent
gle oral doses of cilostazol resulted in peak plasma concen- claudication in patients with PAD.
trations after three to four hours and an elimination half- Money et al.4 assessed the effect of cilostazol 100 mg
life of 11–13 hours. Steady-state concentrations are achieved twice daily for 16 weeks in a multicenter, randomized, dou-
by day 4 following multiple oral dosing of 100 mg twice ble-blind, placebo-controlled trial on treadmill walking
daily in adults.38 In the presence of a fatty meal, the rate of distance, functional status, and ABIs in 239 patients with
absorption and AUC (bioavailability) were increased com- intermittent claudication. The ACD improved significantly
pared with the fasting state.39 In vitro studies40 suggest that in cilostazol-treated patients (47% vs. 12.9%; p < 0.001)
95% of cilostazol is plasma protein bound, particularly to compared with those who received placebo after 16 weeks.
albumin. Subjective functional status measures and ABIs were also
Cilostazol undergoes extensive hepatic metabolism in significantly better in cilostazol-treated patients. Thus,
humans by CYP3A4, to a lesser extent by CYP2C19, and findings were consistent across all end points, although im-
to a relatively minor extent by CYP1A2.8,40,41 The major provements in ABIs have not generally been associated
50 ■ The Annals of Pharmacotherapy ■ 2001 January, Volume 35 www.theannals.com
Downloaded from aop.sagepub.com by guest on August 12, 2015
Cilostazol
with improved walking distance in other claudication tri- placebo in this trial were similar to those reported in previ-
als. Dawson et al.5 demonstrated that cilostazol 100 mg ous studies of this agent.2
twice daily for 12 weeks improved ICD and ACD by 35% Cilostazol produced modest but highly consistent in-
(p < 0.01) and 41% (p < 0.005), respectively, compared creases in walking distances in all claudication trials pub-
with placebo in 81 patients. Patient and physician assess- lished to date, which have included over 1500 patients in
ment of improvement corroborated the measured improve- the US. In one trial,33 cilostazol produced greater benefit
ments in walking performance observed in cilostazol-treat- than pentoxifylline, the only alternative pharmacologic
ed patients. In this relatively small study, significant differ- therapy for intermittent claudication. Furthermore, in three
ences between cilostazol and placebo became apparent of these studies,4-6 subjective quality-of-life assessments
only after 12 weeks of treatment. by patients and physicians corroborated the measured im-
A multicenter study conducted by Beebe et al.6 random- provements in walking performance. This suggests that
ized 516 patients with moderately severe, stable intermit- cilostazol will indeed produce clinically meaningful im-
tent claudication in a double-blind study to receive cilosta- provement in the quality of life of PAD patients with inter-
zol 50 mg, 100 mg, or placebo twice daily for 24 weeks. mittent claudication. Cilostazol had no effect on the cardio-
Improvements in ICD and ACD with cilostazol compared vascular system in these trials, but they were not designed
with placebo were seen as early as four weeks and contin- to examine this end point. The effect of cilostazol on limb
ued throughout the study. By week 24, there was a 51% salvage in patients with critical limb ischemia is unknown,
improvement in maximal walking distance in patients tak- as only patients with chronic stable PAD were included in
ing cilostazol 100 mg twice daily compared with a 15% these studies. The major criticisms of the claudication trials
improvement in the placebo group (p < 0.001). Improved include the relatively small numbers of patients and their
global and disease-specific quality-of-life assessments were short duration in addition to the withholding of optimal
observed with both doses of cilostazol. medical therapies for PAD — antiplatelet agents including
In a placebo-controlled study lasting 24 weeks, Dawson aspirin were disallowed in all studies4-7,33 and lipid-lower-
et al.7 compared the effect of cilostazol 100 mg twice daily ing therapy was discontinued in one.33
and pentoxifylline 400 mg three times daily in 698 patients
with stable intermittent claudication. Despite a large place- UNLABELED USES
bo effect (a feature seen in many claudication studies), sig-
Coronary Stenting
nificant improvements in ICD and ACD were seen with
cilostazol, but not pentoxifylline. This is an important find- The use of high-pressure balloon inflation and the com-
ing given the modest impact of pentoxifylline on the relief bination of aspirin and ticlopidine therapy markedly re-
of claudication seen in clinical practice.2 The small in- duced the incidence of thrombotic complications following
creases in walking distances with pentoxifylline relative to coronary stenting.43 However, serious adverse events relat-
Table 1. Randomized, Controlled Trials of Cilostazol in Patients with Intermittent Claudication
No. ICD (meters) ACD (meters)
Dose Pts. D ▲ p ▲ p ABI Functional
Reference Design (mg/d) (n) (wk) Pre Post (%) Valuea Pre Post (%) Valuea Pre Post p Valuea Status
Money RCT placebo 120 16 NR 244.3 281.1 12.9 0.68 0.69 NS SF-36 +
et al. CLZ 200 119 236.9 332.6 47 <0.001 0.64 0.70 0.0125 WIQ +
(1998)4
Dawson RCT placebo 25 12 77.7 84.6 –2.5 NS 244.3 152.1 –9.3 NR Pat/Phy +/+
et al. CLZ 200 52 71.2 112.5 31.7 <0.01 141.9 231.7 30.5 <0.005
(1998)5
Beebe RCT placebo 170 24 72.4 95.5 20 147.8 174.6 15 SF-36 +
et al. CLZ 100 171 66.5 115.1 48 <0.001 131.5 198.8 38 <0.001 NR WIQ +
(1999)6 CLZ 200 175 70.4 137.9 59 <0.001 129.7 258.8 51 <0.001 COM +
Pat/Phy +/+
Dawson RCT placebo 239 24 55.1 33.5
et al. PTX 1200 232 68.4 NS 30.4 NS NR NR
(1998)7 CLZ 200 227 98.3 <0.05 53.9 <0.05
Elam et al. RCT placebo 94 12 NR 244 304 24.3 0.65 0.65 NS NR
(1998)33 CLZ 200 95 262 335 35.5 <0.004 0.66 0.73 <0.001
+ = significant improvement in measure of functional status; ▲ = percent change in geometric means between baseline and follow-up; ABI = ankle–
brachial index; ACD = absolute claudication distance; CLZ = cilostazol; COM = Claudication Outcome Measures; D = duration; ICD = initial claudication
distance; NR = not reported; Pat/Phy = subjective assessment of improvement by patient and physician; PTX = pentoxifylline; RCT = randomized,
controlled trial; SF-36 = Medical Outcomes Scale Short Form-36; WIQ = Walking Impairment Questionnaire.
a
p Value for comparison between active treatment and placebo.
www.theannals.com The Annals of Pharmacotherapy ■ 2001 January, Volume 35 ■ 51
Downloaded from aop.sagepub.com by guest on August 12, 2015
MP Reilly and ER Mohler III
ing to ticlopidine use44 have prompted an examination of nosis with cilostazol following coronary angioplasty at six
potentially safer antiplatelet agents such as clopidogrel, an months in a study of 68 patients compared with ticlopidine
agent with a similar mode of action but less serious adverse (n = 8) or aspirin (n = 25). In a randomized study of 35 pa-
effects than ticlopidine.45 The recent report46 of an extreme- tients (43 lesions) undergoing elective Palmaz–Schatz stent
ly rare association between clopidogrel and thrombotic implantation, Yamasaki et al.52 showed reduced late lumen
thrombocytopenic purpura supports ongoing efforts to dis- loss at six months in patients receiving cilostazol 200 mg/d
cover new, safe, and effective antiplatelet regimens for compared with aspirin 243 mg/d. Tsuchikane et al., in a se-
coronary stenting. Given its broad range of antiplatelet ac- ries of distinct percutaneous transluminal coronary angiog-
tivity, cilostazol is a potential alternative in poststenting an- raphy (n = 211; 273 lesions),12 directional coronary
tiplatelet regimens. In two small, prospective, nonrandom- atherectomy (n = 39),50 and stent implantation (n = 29; 41
ized Japanese studies,47,48 cilostazol 200 mg/d appeared to stents)49 studies at a single center, reported reduced reste-
be as safe and efficacious as aspirin 243 mg/d following nosis rates in patients randomized to receive cilostazol 200
stent implantation. Park et al.11 compared the effects of mg/d compared with aspirin 250 mg/d. In a four-armed
cilostazol 200 mg/d for six months with ticlopidine 500 study of cilostazol 200 mg/d, probucol 500 mg/d, the com-
mg/d for four weeks in a randomized, controlled trial in bination of both drugs, and placebo in 126 patients (165 le-
490 patients undergoing elective stent implantation. All pa- sions) undergoing elective stenting, Sekiya et al.51 found
tients received aspirin 200 mg/d and treatment was started significantly lower rates of restenosis at six months in the
two days prior to the procedure. At 30 days follow-up, combination therapy and cilostazol-treated patients com-
rates of stent thrombosis (0.8% vs. 0.4%; p = NS) and my- pared with those who received probucol alone or placebo.
ocardial infarction (0.8% vs. 0.4%; p = NS) were similar The effect of cilostazol on restenosis has not yet been test-
with cilostazol and ticlopidine, respectively. No deaths oc- ed in a large, randomized, double-blind trial, and its effica-
curred in either group, and there were no serious adverse cy in the setting of concomitant glycoprotein IIβ/IIIα an-
events in cilostazol-treated patients. Currently, aspirin/ tagonism, which may also reduce restenosis,54 is presently
cilostazol has not been directly compared with aspirin/ unknown.
clopidogrel, the presently favored antiplatelet regimen fol-
lowing coronary stenting. Safety and Adverse Events
RESTENOSIS
Minor adverse effects occurred more frequently (~50%
vs. 25%) with cilostazol than placebo during clinical trials.4-7
Given its antiproliferative properties and promising re- The most common adverse effects reported included head-
sults in animal models of vascular injury, cilostazol has ache (25–35% vs. 10–16%), diarrhea (25–30% vs. 5–8%),
been tested for its efficacy in preventing restenosis follow- dizziness (10–13% vs. 2–6%), and palpitations (11–18%
ing coronary interventions in a series of small, nonblind vs. 0 –3%). In most cases, these symptoms were mild or
studies (Table 2).12,49-53 Take et al.53 reported reduced reste- transient, responded to symptomatic treatment or dose re-
Table 2. Trials Examining the Effect of Cilostazol on Restenosis Following Percutaneous Coronary Interventions
Dose No. D Restenosis p MLD p TLR p
Reference Design Intervention (mg/d) Pts./Lesions (mo) (%) Valuea (mm ± SD) Valuea (%) Valuea
Tsuchikane et al. ORCT PTCA ASA 250 99/129 3 39.5 1.37 ± 0.58 28.7
(1999)12 CLZ 200 94/123 17.9 <0.001 1.65 ± 0.55 <0.0001 11.4 <0.001
Nakamura et al. ORCT P–S stent ASA 250 /14 6 NAb –31.81% NR
(1998)49 CLZ 200 /15 NAb –21.85% <0.05
Tsuchikane et al. ORCT DCA ASA 250 19/19 6 26 1.81 ± 0.68 16
(1998)50 CLZ 200 20/20 0 0.02 2.33 ± 0.6 0.016 0 NS
Sekiya et al. ORCT Wiktor–Stent (106) control 32/41 6 31.7 1.92 ± 0.73 NR
(1998)51 P–S stent (59) PRB 500 31/42 16.7 NS 2.19 ± 0.83 NS
CLZ 200 31/40 12.5 <0.05 2.38 ± 0.7 <0.05
PRB/CLZ 32/42 9.5 <0.05 2.62 ± 0.66 <0.01
Yamasaki et al. ORCT P–S stent ASA 243 17/21 6 NR 1.99 ± 0.51 NR
(1998)52 CLZ 200 18/22 2.49 ± 0.4 <0.05
Take et al. ORCT PTCA ASA or TCL 33/40 4–6 40 1.5 ± 0.9 NR
(1997)53 CLZ 100 35/42 16.7 <0.05 1.7 ± 0.8 <0.05
ASA = aspirin; CLZ = cilostazol; D = duration; DCA = directional coronary atherectomy; MLD = minimal lumen diameter; NR = not reported; ORCT =
open-label, randomized, controlled trial; PRB = probucol; PRB/CLZ = combination of probucol and cilostazol; P–S stent = Palmaz–Shatz stent; PTCA
= percutaneous coronary balloon angioplasty; TCL = ticlopidine; TLR = target lesion revascularization.
a
p Value for comparison between active treatment and placebo.
b
Neointimal area (%) at intravascular ultrasound.
52 ■ The Annals of Pharmacotherapy ■ 2001 January, Volume 35 www.theannals.com
Downloaded from aop.sagepub.com by guest on August 12, 2015
Cilostazol
duction (50 mg twice daily), and rarely required discontin- ly) and its active metabolites in humans.40,57 The combination
uation of the drug (<5%). In contrast to ticlopidine, an of cilostazol and more potent CYP3A4 inhibitors, such as
agent with somewhat similar antiplatelet effects as cilosta- ketoconazole, itraconazole, fluconazole, and grapefruit
zol, there have been no reports of significant liver function juice, has not been studied in humans. Distinct CYP3A4
test abnormality, neutropenia, or thrombocytopenia with inhibitors that could potentially interact with cilostazol in-
cilostazol. Cilostazol has not been associated with any sig- clude cimetidine, ranitidine, clarithromycin, danazole, flu-
nificant bleeding complications. oxetine, metronidazole, quinidine, indinavir, and related
The use of oral milrinone or vesnarinone, distinct PDE- antiretroviral agents.59 Omeprazole, a CYP2C19 inhibitor,
III inhibitors, in clinical trials of patients with severe con- produced a modest increase (18%) in plasma cilostazol
gestive heart failure55,56 has been associated with increased concentrations.58 Other drugs that inhibit CYP2C19 and
cardiac mortality (primarily due to arrhythmias). The effect therefore could interact with cilostazol include amio-
of cilostazol on mortality in patients with a history of con- darone, clopidogrel, ketoprofen, fluvastatin, and sulfon-
gestive heart failure is unknown due to the exclusion of amides.59 Thus, a reduced dose of 50 mg twice daily is rec-
this patient population from claudication clinical trials. ommended when using cilostazol with agents known to in-
There was no evidence of increased mortality in eight pla- hibit these cytochrome isoforms; grapefruit juice should be
cebo-controlled clinical trials3 involving >2200 patients re- avoided during cilostazol therapy. Cilostazol does not ap-
ceiving cilostazol for periods of up to six months. Howev- pear to inhibit CYP3A4 in humans, as there was no in-
er, the calculated relative risk of death of 1.2 has a wide crease in plasma concentrations of lovastatin or its metabo-
95% confidence interval (0.5 to 3.1), and there are no data lites following cilostazol coadministration. It is not known
on the long-term risk or the risk in patients with more se- whether cilostazol affects P-glycoprotein transport in the
vere underlying heart disease. This may be particularly im- gastrointestinal tract or kidney. No significant change in
portant in patients with intermittent claudication given the platelet aggregation or bleeding time was observed follow-
prevalence of concomitant coronary artery disease1 and the ing concomitant administration of cilostazol and aspirin.
likelihood of prolonged cilostazol treatment. In one study,6 Furthermore, there was no apparent increase in hemor-
cilostazol was associated with significant increases in heart rhagic events in patients (n = 201) taking cilostazol who
rate (5.1 beats/min with 50 mg and 7.4 beats/min with 100 required aspirin therapy in randomized, controlled trials.4-7
A single dose of warfarin showed no interaction with
mg) and reductions in PR, QRS, and QT intervals on elec-
cilostazol with respect to the effect on platelet aggregation,
trocardiographs compared with placebo, consistent with
bleeding time, or prothrombin time.40
inhibition of cardiac PDE-III in vivo. It is worth noting that
the FDA has required the manufacturer to perform Phase
IV studies examining the long-term safety of and drug in- Pharmacoeconomics
teractions with cilostazol. To date, cilostazol and pentoxifylline are the only two
Cilostazol is contraindicated in patients with heart fail- drugs approved for the relief of intermittent claudication in
ure. Patients with arrhythmias or a recent history of myo- the US.2,3 Although improvement in walking distances with
cardial infarction, myocardial revascularization, or unsta- pentoxifylline has been demonstrated,2,7 the clinical rele-
ble angina were excluded from the intermittent claudica- vance of the small increases in walking distances that it
tion clinical trials. Therefore, caution should be exercised produces remains unclear and the benefit appears to be less
when using cilostazol in subjects with established coronary than with cilostazol. When cilostazol is used for intermit-
artery disease, as the long-term effects of this agent in this tent claudication, recommended doses (100 mg twice dai-
population, in which asymptomatic left-ventricular dys- ly) cost approximately $95/month compared with $60/
function is prevalent, is unknown. Cilostazol has not been month for pentoxifylline 400 mg three times daily.60 No
studied in patients with moderate to severe hepatic impair- studies examining the cost-effectiveness of cilostazol in
ment or in patients on dialysis and therefore should be clinical practice have been reported.
avoided in these situations. The use of this agent in pedi-
atric populations has not been studied. Geriatric popula- Dosing, Administration, and Patient Counseling
tions have been included in cilostazol studies,4-7,38 and nei-
ther the pharmacokinetic characteristics nor clinical effects Cilostazol is available in 50- or 100-mg tablets. The
were affected by age. recommended dosage of cilostazol for intermittent claudi-
cation is 100 mg twice daily taken at least half an hour be-
Drug Interactions fore or two hours after meals. No dose titration is neces-
sary and no limit to the duration of treatment has been rec-
Significant interactions have been reported9,40,57,58 between ommended, although clinical trials lasted a maximum of
cilostazol and drugs that inhibit CYP3A4 and CYP2C19, six months. Patients should be advised to avoid drinking
the predominant metabolic pathways for cilostazol. Coad- grapefruit juice while taking cilostazol. A reduced cilosta-
ministration of cilostazol with diltiazem or erythromycin, zol dose of 50 mg twice daily should be considered during
moderate inhibitors of CYP3A4, led to increased plasma coadministration of CYP3A4 and CYP2C19 inhibitors. A
concentrations of cilostazol (by 53% and 47%, respective- reduced dose can also be used if minor adverse effects per-
www.theannals.com The Annals of Pharmacotherapy ■ 2001 January, Volume 35 ■ 53
Downloaded from aop.sagepub.com by guest on August 12, 2015
MP Reilly and ER Mohler III
sist despite the institution of preventive measures such as References
the use of simple analgesics for headache. Patients with in-
1. Criqui MH, Denenberg JO, Langer RD, Fronek A. The epidemiology of
termittent claudication may respond as early as two to four peripheral arterial disease: importance of identifying the population at
weeks after initiation, but treatment for up to 12 weeks risk. Vasc Med 1997;2:221-6.
may be needed before a beneficial effect is experienced. 2. Girolami B, Bernardi E, Prins MH, ten Cate JW, Hettiarachchi R, Pran-
doni P, et al. Treatment of intermittent claudication with physical train-
Patients should be instructed about the possibility of minor ing, smoking cessation, pentoxifylline or nafronyl. Arch Intern Med
adverse reactions including headache, diarrhea, dizziness, 1999;159:337- 45.
and palpitations. 3. FDA approval of cilostazol. Rockville, MD: Food and Drug Administra-
tion, August 11, 1999.
4. Money SR, Herd JA, Isaacsohn JL, Davidson M, Cutler B, Heckman J,
Formulary Recommendations et al. Effect of cilostazol on walking distances in patients with intermit-
tent claudication caused by peripheral vascular disease. J Vasc Surg
Cilostazol represents a useful addition to the formulary. 1998;27:267-75.
5. Dawson DL, Cutler BS, Hiatt WR, Hobson RW, Martin JD, Bortey ED,
Based on limited data, cilostazol offers an advantage over et al. A comparison of cilostazol and pentoxifylline for intermittent clau-
pentoxifylline, the only alternative drug for the treatment dication. Am J Med 2000;109:523-30.
of intermittent claudication. However, the everyday clini- 6. Beebe HG, Dawson DL, Cutler BS, Herd JA, Strandness DE, Bortey
cal importance of the moderate improvement in walking EB, et al. A new pharmacological treatment for intermittent claudication:
results of a randomized, multicenter trial. Arch Intern Med 1999;159:
distances and quality-of-life scores in the clinical trials will 2041-50.
only be determined with more extensive clinical experi- 7. Dawson DL, Beebe HG, Davidson MH, Chinoy DA, Herd JA, Hiatt
ence. The fact that cilostazol is well tolerated and has not WR, et al. Cilostazol or pentoxifylline for claudication (abstract)? Circu-
lation 1998;98:12.
been associated with any serious complications should fa- 8. Umekaya H, Tanaka T, Kimura Y, Hidaka H. Purification of cyclic
cilitate more widespread use. adenosine monophosphate phosphodiesterase from human platelets
using new-inhibitor sepharose chromatography. Biochem Pharmacol
1984;33:3339- 44.
Summary 9. Okuda Y, Kimura Y, Yamashita K. Cilostazol. Cardiovasc Drug Rev
1993;11:452-65.
PAD may affect up to 5% of Americans over age 55, of- 10. Cone J, Wang S, Tandon N, Fong M, Sun B, Sakurai K, et al. Compari-
ten goes unrecognized, and carries a sixfold increased risk son of the effects of cilostazol and milrinone on intracellular cAMP lev-
of death from cardiovascular events, predominantly my- els and cellular function in platelets and cardiac cells. J Cardiovasc Phar-
macol 1999;34:497-504.
ocardial infarction and stroke.1 Cilostazol, a specific in- 11. Park SW, Lee CW, Kim H-S, Lee H-J, Park H-K, Hong MK, et al. Com-
hibitor of cAMP–PDE-III activity in platelets and vascular parison of cilostazol versus ticlopidine therapy after stent implantation.
smooth-muscle cells, is a potent antiplatelet agent and va- Am J Cardiol 1999;84:511- 4.
12. Tsuchikane E, Fukuhara A, Kobayashi T, Kirino M, Yamasaki K, Ko-
sodilator, and reduces vascular proliferation in vivo. Re- bayashi T, et al. Impact of cilostazol on restenosis after percutaneous
cent multicenter, randomized, placebo-controlled trials coronary balloon angioplasty. Circulation 1999;100:21-6.
have shown its benefit in improving intermittent claudica- 13. Beavo JA, Reifsnyder DH. Primary sequence of cyclic nucleotide phos-
tion in patients with stable PAD compared with placebo phodiesterase isozymes and the design of selective inhibitors. Trends
Pharmacol Sci 1990;11:150-5.
and pentoxifylline. There is no evidence that cilostazol re- 14. Haslam RJ, Dickinson NT, Jang EK. Cyclic nucleotides and phosphodi-
duces cardiovascular events in patients with PAD, al- esterases in platelets. Thromb Haemost 1999;82:412-23.
though clinical trials were not designed to address this hy- 15. Indolfi C, Avvedimento EV, Lorenzo ED, Esposito G, Rapacciuolo A,
Giuliano P, et al. Activation of cAMP-PKA signaling in vivo inhibits
pothesis. More importantly, cilostazol has not been shown smooth muscle cell proliferation induced by vascular injury. Natl Med
to increase cardiovascular mortality, which is a concern 1997;3:775-9.
with distinct phosphodiesterase inhibitors. Despite the lack 16. Yasunaga K, Mase K. Clinical effects of oral cilostazol on suppression of
of serious adverse events from cilostazol to date, its long- platelet function in patients with cerebrovascular disease. Arzneimit-
telforschung 1985;35:1186-8.
term safety, particularly in patients with more severe un- 17. Ikeda Y, Kikuchi M, Murakami H, Satoh K, Murata M, Watanabe K, et
derlying heart disease, remains unknown. Frequent minor al. Comparison of the inhibitory effects of cilostazol, acetyl-salicylic acid
adverse effects, particularly headache, palpitations, and di- and ticlopidine on platelet functions ex vivo: randomized double blind
crossover study. Arzneimittelforschung 1987;37:563-6.
arrhea, may occur in clinical practice. In conclusion, the 18. Igawa T, Tani T, Chijiwa T, Shiragiku T, Shimizu S, Kawamura K, et al.
unique combination of antiplatelet, vasodilatory, antiprolif- Potentiation of anti-platelet aggregating activity of cilostazol with vascu-
erative, and lipid-modifying effects of cilostazol make it an lar endothelial cells. Thromb Res 1990;57:617-23.
attractive agent for use in PAD patients with intermittent 19. Matsumoto Y, Marakuwa K, Okumura H, Adachi T, Tani T, Kimura Y,
et al. Comparative study of anti-platelet drugs in vitro: distinct effects of
claudication. cAMP-elevating drugs and GPIIb/IIIa antagonists on thrombin-induced
platelet responses. Thromb Res 1999;95:19-29.
Muredach P Reilly MB, Cardiovascular Division, Department of 20. Minami N, Suzuki Y, Yamamoto M, Kihira H, Imai E, Wada H, et al. In-
Medicine, School of Medicine, University of Pennsylvania, Philadel- hibition of shear stress-induced platelet aggregation by cilostazol, a spe-
phia, PA cific inhibitor of cGMP-inhibited phosphodiesterase, in vitro and ex
Emile R Mohler III MD, Director of Vascular Medicine, Cardiovas- vivo. Life Sci 1997;61:383-9.
cular Division, Department of Medicine, School of Medicine, Uni- 21. Siess W, Lapetina EG. Functional relationship between cyclic AMP– de-
versity of Pennsylvania pendent protein phosphorylation and platelet inhibition. Biochem J
Reprints: Emile R Mohler III MD, Department of Medicine, School 1990;271:815-9.
of Medicine, University of Pennsylvania, 432 PHI Bldg., 51 North 22. Konstantopoulos K, Grotta JC, Sills C, Wu KK, Hellums JD. Shear-in-
39th St., Philadelphia, PA 19104-2699, FAX 215/662-9866, E-mail duced platelet-aggregation in normal subjects and stroke patients. Thromb
emmd@mail.med.upenn.edu Haemost 1995;74:1329-34.
54 ■ The Annals of Pharmacotherapy ■ 2001 January, Volume 35 www.theannals.com
Downloaded from aop.sagepub.com by guest on August 12, 2015
Cilostazol
23. Tanaka T, Ishikawa T, Hagiwara M, Onoda K, Hidaka H. Effect of 45. Mishkel GJ, Aguirre FV, Ligon RW, Rocha-Singh KJ, Lucore CL. Clopi-
cilostazol, a selective cAMP phosphodiesterase inhibitor on the contrac- dogrel as adjunctive antiplatelet therapy during coronary stenting. J Am
tion of vascular smooth muscle. Pharmacology 1988;36:313-20. Coll Cardiol 1999;34:1884-90.
24. Lindgren S, Andersson KE. Effects of selective phosphodiesterase in- 46. Bennett CL, Connors JM, Carwile JM, Moake JL, Bell WR, Tarantolo
hibitors on isolated coronary, lung and renal arteries from man and rat. SR, et al. Thrombotic thrombocytopenic purpura associated with clopi-
Acta Physiol Scand 1991;142:77-82. dogrel. N Engl J Med 2000;342:1773-7.
25. Saitoh S, Otake T, Owada M, Mitsugi H, Hashimoto H, Maruama Y. 47. Ochiai M, Isshiki T, Takeshita S, Eto K, Toyoizumi H, Sato T, et al. Use
Cilostazol, a novel cyclic AMP phosphodiesterase inhibitor, prevents re- of cilostazol, a novel antiplatelet agent, in a post-Palmaz–Schatz stenting
occlusion after coronary arterial thrombolysis with recombinant tissue- regimen. Am J Cardiol 1997;79:1471- 4.
type plasminogen activator. Arterioscleros Thromb 1993;13:563-70. 48. Yoshitomi Y, Kojima T, Yano M, Matsumoto Y, Kuramochi M. An-
26. Nakazawa T, Tani T, Matsumoto Y, Yoshikawa T, Kimura Y. Change in tiplatelet treatment with cilostazol after stent implantation. Heart 1998;
anti-platelet and vasodilating effects after chronic administration of 80:393-6.
cilostazol and beraprost (abstract). Thromb Haemost 1997:77:691. 49. Nakamura T, Tsuchikane E, Sumitsuji S, Awata N, Kobayashi T. Impact
27. Takahashi S, Oida K, Fujiwara R, Maeda H, Hayashi S, Tkai H, et al. Ef- of cilostazol on neointimal proliferation following Palmaz–Schatz stent
fect of cilostazol, a cyclic AMP phosphodiesterase inhibitor, on the pro- implantation: a prospective randomized trial (abstract). J Am Coll Cardi-
liferation of rat aortic smooth muscle cells in culture. J Cardiovasc ol 1998;31:404A.
Pharm 1992;20:900-6. 50. Tsuchikane E, Katoh O, Fukuhara A, Funamoto M, Otsuji S, Tateyama
28. Matousovic K, Grande JP, Chini CCS, Chini EN, Dousa TP. Inhibitors of H, et al. Impact of cilostazol on intimal proliferation after directional
cyclic nucleotide phosphodiesterase isozymes type-III and type-IV sup- coronary atherectomy. Am Heart J 1998;135:495-502.
press mitogenesis of rat mesangial cells. J Clin Invest 1995;96:401-10. 51. Sekiya M, Funada J, Watanabe K, Miyagawa M, Akutso H. Effects of
29. Ikeda U, Ikeda M, Kano S, Kanbe T, Shimada K. Effect of cilostazol, a probucol and cilostazol alone and in combination on the frequency of
cAMP phosphodiesterase inhibitor, on nitric oxide production by vascu- poststenting restenosis. Am J Cardiol 1998;82:144-7.
lar smooth muscle cells. Eur J Pharmacol 1996;314:197-202. 52. Yamasaki M, Hara K, Ikari Y, Kobayashi N, Kozuma K, Ohmoto Y, et
30. Kayanoki Y, Che W, Kawata S, Matsuzawa Y, Higashiyama S, Tani- al. Effects of cilostazol on late lumen loss after Palmaz–Schatz stent im-
guchi N. The effect of cilostazol, a cyclic nucleotide phosphodiesterase plantation. Cath Cardiovasc Diag 1998;44:387-91.
III inhibitor, on heparin-binding EGF-like growth factor expression in 53. Take S, Matsutani M, Ueda H, Hamaguchi H, Konishi H, Baba Y, et al.
macrophages and vascular smooth muscle cells. Biochem Biophys Res Effect of cilostazol in preventing restenosis after percutaneous translumi-
Commun 1997;238:478-81. nal coronary angioplasty. Am J Cardiol 1997;79:1097-9.
31. Numano F, Maezawa H, Shimamoto T, Adachi K. Change of cyclic- 54. Topol EJ, Califf RM, Weisman HF, Ellis SG, Tcheng JE, Worley S, et al.
AMP and cyclic-AMP phosphodiesterase in the progression and regres- Randomized trial of coronary intervention with antibody against platelet
sion of experimental atherosclerosis. Ann N Y Acad Sci 1976;275:311- GP IIβ/IIIα integrin for reduction of clinical restenosis: results at six
20. months. Lancet 1994;343:881-6.
32. Ishizaka N, Taguchi J, Kimura Y, Ikaari Y, Aizawa T, Togo M, et al. Ef- 55. Packer M, Carver JR, Rodeheffer RJ, Ivanhoe RJ, Dibianco R, Zeldis
fects of single local administration of cilostazol on neointimal formation SM, et al. Effect of oral milrinone on mortality in severe chronic heart
in balloon-injured rat carotid artery. Atherosclerosis 1999;142:41-6. failure: the PROMISE Study Research Group. N Engl J Med 1991;325:
33. Elam MB, Heckman JR, Crouse DB, Hunninghake JA, Herd M, David- 1468-75.
son IL, et al. Effect of the novel antiplatelet agent, cilostazol, on plasma 56. Cohn JN, Goldstein SO, Greenberg BH, Lorell BH, Bourge RC, Jaski
lipoproteins in patients with intermittent claudication. Arterscleros BE, et al. A dose-dependent increase in mortality with vesnarinone
Thromb Vasc Biol 1998;18:1942-7. among patients with severe heart failure. Vesnarinone Trial Investigators.
34. Motoyashiki T, Morita T, Ueki H. Involvement of the rapid increase in N Engl J Med 1998;339:1848-50.
cAMP content in the vandate-stimulated release of lipoprotein lipase ac- 57. Suri A, Forbes WP, Bramer SL. Effect of CYP3A inhibition on the me-
tivity from rat fat pads. Biol Pharm Bull 1996;19:1412-6. tabolism of cilostazol. Clin Pharmacokinet 1999;37(suppl 2):61-8.
35. Bjornsson OG, Sparks JD, Sparks CE, Gibbons GF. Regulation of 58. Suri A, Bramer SL. Effect of omeprazole on the metabolism of cilosta-
VLDL secretion in primary culture of rat hepatocytes: involvement of zol. Clin Pharmacokinet 1999;37(suppl 2):53-9.
cAMP and cAMP-dependent protein kinases. Eur J Clin Invest 1994;24:
59. Michalets EL. Update: clinically significant cytochrome P- 450 drug in-
137- 48.
teractions. Pharmacotherapy 1998;18:84-112.
36. Niki T, Mori H. Phase I study of cilostazol. Safety evaluation at increas-
60. Drug topics redbook. Montvale, NJ: Medical Economics, 2000.
ing single doses in healthy volunteers. Arzneimittelforschung 1985;35:
1173-85.
37. Akiyama H, Kubo S, Shimuzu T. The absorption, distribution and excre-
tion of a new antithrombotic and vasodilating agent, cilostazol, in rat,
rabbit, dog and man. Arzneimittelforschung 1985;35:1124-32. EXTRACTO
38. Suri A, Forbes WP, Bramer SL. Pharmacokinetics of multiple-dose oral
cilostazol in middle-age and elderly men and women. J Clin Pharm OBJETIVO: Repasar la farmacología y la utilidad clínica de cilostazol, un
1998;38:144-50. agente antiplaquetario y vasodilatador aprobado recientemente para el
39. Bramer SL, Forbes WP. Relative bioavailability and effects of a high fat manejo de claudicación intermitente.
meal on single dose cilostazol pharmacokinetics. Clin Pharmacokinet FUENTES DE INFORMACIÓN: Búsqueda de la literatura primaria de
1999;37(suppl 2):13-23. cilostazol en MEDLINE de enero de 1980 a febrero de 2000. Extractos
40. Advisory Committee Meeting Dossier. Cilostazol for use in patients with seleccionados de presentaciones y literatura del fabricante se usaron
intermittent claudication. Rockville, MD: Otsuka America Pharmaceuti- también como fuente. Los términos de catalogar utilizados incluyen
cal, June 3, 1998. cilostazol, claudicación intermitente, inhibidor de plaquetas, y restenosis.
41. Akiyama H, Kubo S, Shimuzu T. The metabolism of a new antithrom-
SELECCIÓN DE ESTUDIOS: Se revisaron estudios clínicos,
botic and vasodilating agent, cilostazol, in rat, dog and man. Arzneimit-
farmacocinéticos, y comparativos aleatorios llevados a cabo en Estados
telforschung 1985;35:1133- 40.
Unidos y Asia. También se examinaron estudios selectos in vitro, ex
42. Mallikaarjun S, Forbes WP, Bramer SL. Effect of renal impairment on
vivo, y en animales cuando no habían disponibles datos humanos.
the pharmacokinetics of cilostazol and its metabolites. Clin Pharma-
cokinet 1999;37(suppl 2):33- 40. SÍNTESIS: Claudicación intermitente, definido como una molestia
43. Schomig A, Neumann FJ, Kastrati A, Schuhlen H. A randomized com- repetitiva de un grupo de músculos inducida por ejercicio y aliviada con
parison of anti-platelet and anticoagulant therapy after placement of descanso, es la manifestación clínica más común de enfermedad de
coronary-artery stent. N Engl J Med 1996;334:1084-9. arterias periféricas (PAD, por sus siglas en inglés). Cilostazol, un
44. Hass WK, Easton JD, Adams HP, Pryse-Phillips W, Molony BA, Ander- inhibidor específico de la fosfodiesterasa de monofosfato de adenosina
son S, et al. A randomized trial comparing ticlopidine hydrochloride cíclica (PDE-III, por sus siglas en inglés) en plaquetas y en las células
with aspirin for the prevention of stroke in high risk patients. N Engl J del músculo liso vascular, es un agente antiplaquetario y vasodilatador
Med 1989;321:501-7. potente, reduce la proliferación vascular y tiene efectos reductores en
www.theannals.com The Annals of Pharmacotherapy ■ 2001 January, Volume 35 ■ 55
Downloaded from aop.sagepub.com by guest on August 12, 2015
MP Reilly and ER Mohler III
lípidos in vivo. Estudios aleatorios, controlado por placebo, randomisées réalisées aux États-Unis et en Asie ont été évaluées.
contribuyeron a la aprobación de cilostazol por la Administración de Lorsque certaines données chez l’humain n’étaient pas disponibles, des
Alimentos y Fármacos para el alivio de claudicación intermitente en études animales, in vivo et ex vivo choisies ont aussi été examinées.
pacientes con PAD estable. Cilostazol permite que se duplique las RÉSUMÉ: La claudication intermittente se définit comme un inconfort
distancias caminadas y mejora la calidad de vida en comparación con reproductible au niveau d’un groupe de muscles, induit par l’exercice et
placebo. Uno de los estudios encontró que cilostazol es más efectivo que soulagé par le repos. Elle constitue la manifestation la plus fréquente de
pentoxifilina, la única alternativa en terapia farmacológica para la maladie vasculaire périphérique (MVP). Le cilostazol, un inhibiteur
claudicación. A pesar de que en la práctica clínica pueden ocurrir efectos spécifique de l’adénosine monophosphate cyclique phosphodiestérase
adversos menores, incluyendo dolor de cabeza, diarrea y palpitaciones, (PDE-III) contenue dans les plaquettes et dans le muscle lisse vasculaire,
con frecuencia (casi un 50%), cilostazol no ha sido asociado a eventos est un agent antiplaquettaire puissant et un vasodilatateur. De plus, il
adversos mayores o a un aumento en mortalidad. Estudios pequeños, no réduit la prolifération vasculaire et possède un effet hypolipémiant in
ciegos, sugieren que cilostazol puede ser de utilidad en prevenir vivo. De récentes études multicentriques, randomisées, et contrôlées par
trombosis y estenosis recurrente después de intervenciones coronarias placebo ont conduit à son approbation par l’Administration des Drogues
percutáneas, aunque éstas no están incluidas en la etiqueta. et Alimentaires, pour le traitement de la claudication intermittente chez
CONCLUSIONES: La combinación única de efectos antiplaquetarios, les patients atteints de MVP stable. Comparativement au placebo, ces
vasodilatadores y antiproliferativos de cilostazol lo hacen un agente études ont démontré que le cilostazol permet de doubler la distance
atractivo para usar en pacientes con PAD. Los estudios clínicos que parcourue à la marche et d’améliorer la qualité de vie des sujets. Une
demuestran una mejoría significativa en distancia caminada con étude a démontré que le cilostazol était plus efficace que la
cilostazol sugieren que éste se convertirá en una herramienta importante pentoxifylline, la seule alternative actuellement disponible pour le
para mejorar los síntomas y la calidad de vida de los pacientes con traitement pharmacologique de la claudication intermittente. Malgré
claudicación intermitente. l’apparition clinique de fréquents effets secondaires mineurs
Sonia I Lugo (approximativement 50%), incluant les céphalées, la diarrhée, et les
palpitations, le cilostazol n’a pas été associé à aucun effet indésirable
majeur, ni à un accroissement de la mortalité. De petites études ouvertes
RÉSUMÉ suggèrent que le cilostazol pourrait être utile dans la prévention de la
OBJECTIF: Réviser la pharmacologie et l’utilité clinique du cilostazol, un thrombose et de la resténose à la suite d’interventions coronariennes
agent antiplaquettaire et un vasodilatateur récemment approuvé dans le percutanées (ICP), une indication qui demeure non approuvée.
traitement de la claudication intermittente. CONCLUSIONS: La combinaison unique des effets antiplaquettaire,
REVUE DE LITTÉRATURE: Une recherche exhaustive dans la banque de vasodilatateur, et antiprolifératif du cilostazol en fait un agent attrayant
données MEDLINE (janvier 1980 à février 2000) a permis d’identifier pour le traitement des patients atteints de MVP. Comme les études
la littérature primaire pertinente concernant le cilostazol. De cliniques ont démontré qu’il procure une amélioration significative de la
l’information additionnelle a été extraite des résumés présentés lors de distance parcourue à la marche, le cilostazol deviendra un outil
conférences scientifiques et de la documentation du manufacturier. Les important pour améliorer les symptômes et la qualité de vie des patients
mot-clés utilisés étaient: cilostazol, claudication intermittente, inhibiteurs atteints de claudication intermittente.
plaquettaires, et resténose. Pierre Martineau
SÉLECTION DES ÉTUDES: Les études humaines cliniques et
pharmacocinétiques, de même que les études comparatives et
56 ■ The Annals of Pharmacotherapy ■ 2001 January, Volume 35 www.theannals.com
Downloaded from aop.sagepub.com by guest on August 12, 2015
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- TL-4 Textured Surface DepthDocument2 pagesTL-4 Textured Surface DepthpaulenewNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A2-Organic Reactions Spider Diagram HANDOUT (Colour)Document1 pageA2-Organic Reactions Spider Diagram HANDOUT (Colour)udaymohur100% (1)
- Dodigen 2808 TDSDocument1 pageDodigen 2808 TDSRashid SaleemNo ratings yet
- Paul M. Mcneill, MD Facs Capitol Vein and Laser Center Bethesda, Maryland Frederick, MarylandDocument28 pagesPaul M. Mcneill, MD Facs Capitol Vein and Laser Center Bethesda, Maryland Frederick, MarylandShandy JonnerNo ratings yet
- Sidik-Chaula Urethroplasty and The Manset Flap For Non-Glanular Hypospadias RepairDocument8 pagesSidik-Chaula Urethroplasty and The Manset Flap For Non-Glanular Hypospadias RepairShandy JonnerNo ratings yet
- Jurnal AkpDocument9 pagesJurnal AkpShandy JonnerNo ratings yet
- EN Acute Pancreatitis As A Complication ofDocument5 pagesEN Acute Pancreatitis As A Complication ofShandy JonnerNo ratings yet
- Emergency Duty Report Wednesday, 31 July 2019Document10 pagesEmergency Duty Report Wednesday, 31 July 2019Shandy JonnerNo ratings yet
- Craniomaxillofacial Trauma: Tutorial of Basic SurgeryDocument42 pagesCraniomaxillofacial Trauma: Tutorial of Basic SurgeryShandy JonnerNo ratings yet
- Evaluation of Swelling Properties of Shale For Design of Underground StructuresDocument8 pagesEvaluation of Swelling Properties of Shale For Design of Underground StructuresSen HuNo ratings yet
- Deka-Unigy High Rate Series HR7500ETDocument2 pagesDeka-Unigy High Rate Series HR7500ETFernandoEscaleraNo ratings yet
- Ozone in WineriesDocument18 pagesOzone in Wineriesdali20080% (1)
- PerkinElmer Analytical Consumables and Accessories Catalogue 2015 2016Document334 pagesPerkinElmer Analytical Consumables and Accessories Catalogue 2015 2016Hector ChamateNo ratings yet
- Concentric EccentricDocument4 pagesConcentric EccentricGabbar SinghNo ratings yet
- One-Step Synthesis of A 12CaO7Al2O3 Electride Via The SparkDocument3 pagesOne-Step Synthesis of A 12CaO7Al2O3 Electride Via The Sparkshazna203No ratings yet
- Manual Compressor CSD 102, EnglishDocument108 pagesManual Compressor CSD 102, EnglishАлександр ЩербаковNo ratings yet
- Trelleborg Elastomeric Bridge Bearings PDFDocument4 pagesTrelleborg Elastomeric Bridge Bearings PDFMad WonderNo ratings yet
- C10 Chemical Bonding IIDocument64 pagesC10 Chemical Bonding IIJay-pee BarronNo ratings yet
- Quantium 310 UHS Brochure AW 2018 DFS Design UpdateDocument4 pagesQuantium 310 UHS Brochure AW 2018 DFS Design UpdatengdeshpandeNo ratings yet
- The Veritable Clavicles of SolomonDocument20 pagesThe Veritable Clavicles of SolomonDonald AristorNo ratings yet
- Float Board Level GaugeDocument6 pagesFloat Board Level GaugeanaismariaNo ratings yet
- Sika Viscocrete 8030S Rev1Document3 pagesSika Viscocrete 8030S Rev1muhammad ridwan zuhriNo ratings yet
- Thermosetting PolymerDocument10 pagesThermosetting PolymerArghya MondalNo ratings yet
- AC Aluminum Pulse (GMAW) Weld Process GuideDocument11 pagesAC Aluminum Pulse (GMAW) Weld Process GuideFirstLast100% (1)
- Polymer ScienceDocument101 pagesPolymer SciencereddyNo ratings yet
- Dialysis Reverse OsmosisDocument9 pagesDialysis Reverse OsmosisK.D. PatelNo ratings yet
- Compro DauDocument98 pagesCompro DauIsmail KarmanaNo ratings yet
- Section 09260Document60 pagesSection 09260y2kareinNo ratings yet
- Analysis of UrineDocument28 pagesAnalysis of UrineDi ako SiNo ratings yet
- Sika Antisol e WpiDocument2 pagesSika Antisol e WpiMd. Mominul IslamNo ratings yet
- Pompe À Eun Honda WMP20XDocument100 pagesPompe À Eun Honda WMP20XLaure GarnierNo ratings yet
- (SiC-En-2013-22) Molding Compounds Adhesion and Influence On Reliability of Plastic Packages For SiC-Based Power MOS DevicesDocument13 pages(SiC-En-2013-22) Molding Compounds Adhesion and Influence On Reliability of Plastic Packages For SiC-Based Power MOS Devicesnuaa_qhhNo ratings yet
- Notes On Hole Cleaning: Manual 2.0)Document8 pagesNotes On Hole Cleaning: Manual 2.0)JesusJesusNo ratings yet
- Autoimmune ThyroiditisDocument7 pagesAutoimmune Thyroiditiskumar23No ratings yet
- SPM Biology Form 4 Nutrition NotesDocument12 pagesSPM Biology Form 4 Nutrition NotesArthur IsaacNo ratings yet
- Exp 7. Liquid Diffusion CoefficientDocument2 pagesExp 7. Liquid Diffusion Coefficient김승민No ratings yet