Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ravengro Expanded CompleteDocument10 pagesRavengro Expanded Completeitsme5616No ratings yet
- Retail Management ProblemsDocument3 pagesRetail Management ProblemsshubhakarNo ratings yet
- SAP BW Business Blueprint Step by Step GuideDocument33 pagesSAP BW Business Blueprint Step by Step Guidekavya.nori0% (1)
- English Literacy NarrativeDocument4 pagesEnglish Literacy Narrativeapi-325516593No ratings yet
- Dominos StrategyDocument23 pagesDominos StrategySaqib RizviNo ratings yet
- Amro Ismail Kasht 200802124: Engineering EconomyDocument5 pagesAmro Ismail Kasht 200802124: Engineering EconomyAmroKashtNo ratings yet
- Matabuena vs. CervantesDocument1 pageMatabuena vs. CervantesAndrew GallardoNo ratings yet
- Legal Metrology Act: Analysis: Dhruv Sharma, 01319103516 BBALLB 9Document4 pagesLegal Metrology Act: Analysis: Dhruv Sharma, 01319103516 BBALLB 9dhruv sharmaNo ratings yet
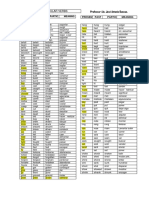
- Irregular Verbs Nueva Lista DuncanDocument2 pagesIrregular Verbs Nueva Lista DuncanAndrey Vargas MoralesNo ratings yet
- 01.worksheet-1 U1Document1 page01.worksheet-1 U1Jose Manuel AlcantaraNo ratings yet
- Waterfront Boundaries For Grants of Public Crown Lands - MNR - E000074 - 2001Document3 pagesWaterfront Boundaries For Grants of Public Crown Lands - MNR - E000074 - 2001Sen HuNo ratings yet
- OIPD in LinguisticsDocument7 pagesOIPD in LinguisticsBela AtthynaNo ratings yet
- (ACV-S01) Week 01 - Pre-Task - Quiz - Weekly Quiz (PA) - INGLES IV (37832)Document5 pages(ACV-S01) Week 01 - Pre-Task - Quiz - Weekly Quiz (PA) - INGLES IV (37832)Alicia PadillaNo ratings yet
- Wits Visual StorytellingDocument4 pagesWits Visual Storytellingapi-238364900No ratings yet
- MANISHDocument19 pagesMANISHAshutosh SaxenaNo ratings yet
- Book Decade SDocument555 pagesBook Decade STrey MaklerNo ratings yet
- AC3103 Seminar 19: Biosensors International Group (BIG) Valuation and Impairment Testing of IntangiblesDocument39 pagesAC3103 Seminar 19: Biosensors International Group (BIG) Valuation and Impairment Testing of IntangiblesTanisha GuptaNo ratings yet
- Ayobami Kehinde An Aesthetics of Realism The Image of Postcolonial Africa in Meja Mwangis Going Down River Road An EssayDocument31 pagesAyobami Kehinde An Aesthetics of Realism The Image of Postcolonial Africa in Meja Mwangis Going Down River Road An EssayMedara MosesNo ratings yet
- A Study On Adoption of Digital Payment Through Mobile Payment Application With Reference To Gujarat StateDocument6 pagesA Study On Adoption of Digital Payment Through Mobile Payment Application With Reference To Gujarat StateEditor IJTSRDNo ratings yet
- Action Research ProposalDocument4 pagesAction Research ProposalClarisse Chiu83% (6)
- Chfs ExamplesDocument4 pagesChfs ExamplescsdhimanNo ratings yet
- Equity EssayDocument8 pagesEquity EssayTeeruVarasuNo ratings yet
- CatalogueDocument230 pagesCatalogueOsama_Othman01100% (1)
- Graduation ScriptDocument2 pagesGraduation Scriptangela joy victoriaNo ratings yet
- LAKAS NG MANGGAGAWANG MAKABAYAN (LAKAS), vs. MARCELO ENTERPRISESDocument6 pagesLAKAS NG MANGGAGAWANG MAKABAYAN (LAKAS), vs. MARCELO ENTERPRISESRudith ann QuiachonNo ratings yet
- Venezuelan Food Glossary Ver6Document1 pageVenezuelan Food Glossary Ver6Peter BehringerNo ratings yet
- Emma J. Stafford - Greek Cults of Deified AbstractionsDocument269 pagesEmma J. Stafford - Greek Cults of Deified Abstractions21Tauri100% (1)
- Maruti Suzuki India Limited (Msil)Document7 pagesMaruti Suzuki India Limited (Msil)KARUN RAJ K MBA IB 2018-20No ratings yet
- Ebook An Introduction To Contemporary Islamic Philosophy 3Rd Edition Mohammad Fana I Eshkevari Online PDF All ChapterDocument69 pagesEbook An Introduction To Contemporary Islamic Philosophy 3Rd Edition Mohammad Fana I Eshkevari Online PDF All Chaptercarl.rojas572100% (9)
- Medha Suktam 2019 - 2020Document3 pagesMedha Suktam 2019 - 2020xs111No ratings yet