Download as doc, pdf, or txt
You might also like
- Nursing Cheat Sheets 76 Cheat Sheets For Nursing Students - Nodrm PDFDocument100 pagesNursing Cheat Sheets 76 Cheat Sheets For Nursing Students - Nodrm PDFAnnissa Larnard96% (56)
- Lab09 Therapy4 IronDeficiencyDocument5 pagesLab09 Therapy4 IronDeficiencyHayna Rose100% (1)
- Coventry 06.2012Document14 pagesCoventry 06.2012karan270No ratings yet
- Good Discharge Summary Sample - SurgeryDocument3 pagesGood Discharge Summary Sample - SurgeryRao Rizwan Shakoor100% (1)
- Biology Investigatory Project: Topic - DiabetesDocument19 pagesBiology Investigatory Project: Topic - Diabetesaditya gollakota83% (40)
- IM Platinum 3rd-EdDocument357 pagesIM Platinum 3rd-EdJust Some Files100% (2)
- Maternal Neonatal Facts Made Incredibly Quick! 2nd EdDocument112 pagesMaternal Neonatal Facts Made Incredibly Quick! 2nd Edmarione2489% (9)
- Toacs 2Document104 pagesToacs 2aliakbar178No ratings yet
- 1 PDFDocument5 pages1 PDFalejandrovesgaNo ratings yet
- Case 056: Common Bile Duct Stones (Choledocholithiasis)Document5 pagesCase 056: Common Bile Duct Stones (Choledocholithiasis)ZauzaNo ratings yet
- Heath Day 4 Care Plan 3Document12 pagesHeath Day 4 Care Plan 3api-639508852No ratings yet
- Liver Abscess Caused by Foreign BodyDocument5 pagesLiver Abscess Caused by Foreign BodyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- POMR FAH BAshori CMLDocument22 pagesPOMR FAH BAshori CMLIka AyuNo ratings yet
- Lab 10Document5 pagesLab 10Mira Mhsen KhaloufNo ratings yet
- Multiple System Organ FailureDocument16 pagesMultiple System Organ Failurerefika rahmiNo ratings yet
- Multiple System Organ Failure/Multiple Organ Dysfunction SyndromeDocument14 pagesMultiple System Organ Failure/Multiple Organ Dysfunction SyndromemalathiNo ratings yet
- DepartmentDocument7 pagesDepartmentmubarek abdurohemanNo ratings yet
- Modified CaseDocument22 pagesModified CaseAli HawamdeNo ratings yet
- Nephrorounds3 2015final 150907110921 Lva1 App6892 PDFDocument133 pagesNephrorounds3 2015final 150907110921 Lva1 App6892 PDFTabada NickyNo ratings yet
- Jha2 2 118Document3 pagesJha2 2 118Renato DantasNo ratings yet
- COPDDocument10 pagesCOPDChaudhary AbhishekNo ratings yet
- FINAL Endocrinology CaseDocument22 pagesFINAL Endocrinology CaseJude Micko Bunyi Alipit100% (1)
- Template Duty ReportDocument6 pagesTemplate Duty ReportJefri SusantoNo ratings yet
- Shiv DanDocument3 pagesShiv Danpulmonary dischargeNo ratings yet
- Module 17 Part 2 Ratio 19 22 EndoDocument102 pagesModule 17 Part 2 Ratio 19 22 EndoLA BriguelaNo ratings yet
- Wet Beriberi With Multiple Organ Failure Remarkably Reversed by Thiamine Administration - A Case Report and Literature ReviewDocument5 pagesWet Beriberi With Multiple Organ Failure Remarkably Reversed by Thiamine Administration - A Case Report and Literature Reviewgwyneth.green.512No ratings yet
- KannanDocument4 pagesKannanShivaS SNo ratings yet
- Name-Age/Sex - MRD No. - Date of Admission - Ward - Address - Diagnosis - History Taking History of Present IllnessDocument17 pagesName-Age/Sex - MRD No. - Date of Admission - Ward - Address - Diagnosis - History Taking History of Present IllnessMeena KoushalNo ratings yet
- Diabetes MellitusDocument64 pagesDiabetes MellitusCris Tine67% (6)
- Mortality-conference-2022.03.24 FINAL (自動儲存)Document51 pagesMortality-conference-2022.03.24 FINAL (自動儲存)許誌元No ratings yet
- MR AlimuddinDocument10 pagesMR AlimuddinNur Farmawati Humayrah HassaniNo ratings yet
- Complex Care Plan 1Document12 pagesComplex Care Plan 1api-496883420No ratings yet
- CLINICAL CASE 8 - Endocrinology, Diabetes & Metabolism Case Reports) Recurrent Primary Hyperparathyroidism - A Diagnostic and Management DilemmaDocument5 pagesCLINICAL CASE 8 - Endocrinology, Diabetes & Metabolism Case Reports) Recurrent Primary Hyperparathyroidism - A Diagnostic and Management DilemmaAthul IgnatiusNo ratings yet
- GroupA RenalDisordersDocument13 pagesGroupA RenalDisordersPaulNo ratings yet
- IM AdconDocument28 pagesIM AdconCla SantosNo ratings yet
- CMC Cns Infection 2023Document5 pagesCMC Cns Infection 2023Juan RecyNo ratings yet
- Ahmad Basori VidiDocument30 pagesAhmad Basori VidiIka AyuNo ratings yet
- Manajemen Pasien CKD Di Instalasi Gawat DaruratDocument48 pagesManajemen Pasien CKD Di Instalasi Gawat DaruratUmar MukhNo ratings yet
- Renal PacesDocument4 pagesRenal PacesRebecca Teng Siew YanNo ratings yet
- Care Plan 4Document31 pagesCare Plan 4Chelsea RuthrauffNo ratings yet
- Two Cases of BRASH Syndrome: A Diagnostic Challenge: European Journal Internal MedicineDocument4 pagesTwo Cases of BRASH Syndrome: A Diagnostic Challenge: European Journal Internal MedicineDesi MeliaNo ratings yet
- Ijccm 26 239Document5 pagesIjccm 26 239DidiNo ratings yet
- The CaseDocument33 pagesThe CasemarunxNo ratings yet
- Renal TransplantationDocument50 pagesRenal Transplantationregie cuaresmaNo ratings yet
- ICU Management of Acute PancreatitisDocument77 pagesICU Management of Acute PancreatitisAndriy SubieNo ratings yet
- CARDIAC CATHETERIZATION LABORATORY AN INTRODUCTORY MANUAL, University of TennesseeDocument29 pagesCARDIAC CATHETERIZATION LABORATORY AN INTRODUCTORY MANUAL, University of TennesseeNavojit ChowdhuryNo ratings yet
- English Version-SubmitDocument10 pagesEnglish Version-Submit5211119No ratings yet
- Mesenteric Venous Thrombosis As A Rare Complication of Decompression SicknessDocument5 pagesMesenteric Venous Thrombosis As A Rare Complication of Decompression SicknessVan Cuong TranNo ratings yet
- CMJ 130 2011Document2 pagesCMJ 130 2011studentstoma61No ratings yet
- Shared RX Modules For FinalsDocument11 pagesShared RX Modules For FinalsOdyNo ratings yet
- Tuberculous Pericarditis Leading To Cardiac Tamponade Importance of Screening Prior To ImmunosuppressionDocument3 pagesTuberculous Pericarditis Leading To Cardiac Tamponade Importance of Screening Prior To ImmunosuppressionLink BuiNo ratings yet
- CHF CASE + Problem Based LearningDocument13 pagesCHF CASE + Problem Based LearningYarfa KhurramNo ratings yet
- Program Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaDocument17 pagesProgram Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaIka AyuNo ratings yet
- NCM 118 - Lesson 15 (Chronic Renal Failure and Dialysis)Document7 pagesNCM 118 - Lesson 15 (Chronic Renal Failure and Dialysis)Bobby Christian DuronNo ratings yet
- Carrick 2018Document7 pagesCarrick 2018Edwin AlvarezNo ratings yet
- Post Polypectomy Electrocoagulation Syndrome A Rare Cause of Acute Abdominal PainDocument5 pagesPost Polypectomy Electrocoagulation Syndrome A Rare Cause of Acute Abdominal PainCom DigfulNo ratings yet
- Artigo - Gitelman Syndrome ÍntegraDocument2 pagesArtigo - Gitelman Syndrome Íntegrasalvianolucas5No ratings yet
- Case Studies: Recurrent Fever, Chills, and Malaise in A 53-Year-Old ManDocument2 pagesCase Studies: Recurrent Fever, Chills, and Malaise in A 53-Year-Old Mansreeja maragoniNo ratings yet
- Ancylostoma Duodenale Presented As Severe Anaemia: A Case Report in A Tertiary Care Centre, North-East IndiaDocument5 pagesAncylostoma Duodenale Presented As Severe Anaemia: A Case Report in A Tertiary Care Centre, North-East IndiaIJAR JOURNALNo ratings yet
- LeelaDocument11 pagesLeelaksaileela99No ratings yet
- Alcoholic Hepatitis-The Case For Intensive ManagementDocument4 pagesAlcoholic Hepatitis-The Case For Intensive ManagementSunita RaniNo ratings yet
- Rahmatia Efusi PleuraDocument14 pagesRahmatia Efusi PleuraJuli2022 Semnol-SemsaNo ratings yet
- Labs & Imaging for Primary Eye Care: Optometry In Full ScopeFrom EverandLabs & Imaging for Primary Eye Care: Optometry In Full ScopeNo ratings yet
- ValuCare Accredited Providers v012017Document66 pagesValuCare Accredited Providers v012017aeroren40% (5)
- Healthy Sleep FsDocument4 pagesHealthy Sleep Fsvivek_sharma13No ratings yet
- Record of Daily TreatmentDocument5 pagesRecord of Daily Treatmentann bernasyl vestalNo ratings yet
- Urbina Analysis in Articles BSMT2GDocument2 pagesUrbina Analysis in Articles BSMT2GCherith UrbinaNo ratings yet
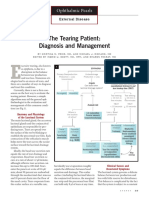
- The Tearing Patient: Diagnosis and Management: Ophthalmic PearlsDocument3 pagesThe Tearing Patient: Diagnosis and Management: Ophthalmic PearlsAnonymous otk8ohj9No ratings yet
- W2D3 DR - Yasa-Bacteremia Dan SepsisDocument54 pagesW2D3 DR - Yasa-Bacteremia Dan SepsisJaka BawaviNo ratings yet
- AcetazolamideDocument25 pagesAcetazolamideDiwan AyuNo ratings yet
- Journal of Oral Biology and Craniofacial Research 9 (2019) 340-346Document7 pagesJournal of Oral Biology and Craniofacial Research 9 (2019) 340-346laur112233No ratings yet
- Pharma IndustryDocument69 pagesPharma IndustryAnuj Tambe100% (1)
- Content I. Definition of Staffing IV. Staffing NeedsDocument5 pagesContent I. Definition of Staffing IV. Staffing NeedsTeal Otter100% (1)
- Comt Brochure 8 Days New FinalDocument12 pagesComt Brochure 8 Days New Finaljingluo educationNo ratings yet
- Perioperative Nursing EducationDocument3 pagesPerioperative Nursing Educationgeorgeloto12No ratings yet
- Rational Antibiotic Practice: Under IAP Action Plan 2014 Academic Grant From Delcure PharmaDocument164 pagesRational Antibiotic Practice: Under IAP Action Plan 2014 Academic Grant From Delcure PharmaGurmeet SinghNo ratings yet
- ACell Nir Hus MD. Regenerative Medicine.Document78 pagesACell Nir Hus MD. Regenerative Medicine.Nir Hus, MDNo ratings yet
- NCM 116: Care of Clients With Problems in Nutrition and Gastrointestinal, Metabolism and Endocrine,, Acute and ChronicDocument18 pagesNCM 116: Care of Clients With Problems in Nutrition and Gastrointestinal, Metabolism and Endocrine,, Acute and ChronicSIJINo ratings yet
- Noor Msallaty - 8 Pages of Research PaperDocument16 pagesNoor Msallaty - 8 Pages of Research Paperapi-445615356No ratings yet
- CHN 1 Topic 1. A Handout in Overview of Public Health Nursing in The Phils.Document11 pagesCHN 1 Topic 1. A Handout in Overview of Public Health Nursing in The Phils.DANIAH ASARI. SAWADJAANNo ratings yet
- Neurological Disorders Practice Test QuestionsDocument6 pagesNeurological Disorders Practice Test QuestionsBenedict AlvarezNo ratings yet
- Care of Patients With Traction NewDocument17 pagesCare of Patients With Traction Newjohnpantinople100% (18)
- Normalizing Advanced Practice in Public Health Nursing in The Philippines: A Foucauldian AnalysisDocument7 pagesNormalizing Advanced Practice in Public Health Nursing in The Philippines: A Foucauldian Analysiscj bariasNo ratings yet
- Forensic Med EntomologyDocument304 pagesForensic Med EntomologyCharish DanaoNo ratings yet
- Summary of Chapter 4 Diseases of The Immune System: Innate and Adaptive ImmunityDocument8 pagesSummary of Chapter 4 Diseases of The Immune System: Innate and Adaptive ImmunityBadda casNo ratings yet
- Cwu Ong TwinDocument14 pagesCwu Ong TwinAiman ArifinNo ratings yet
- MDC - Mariana ResumeDocument4 pagesMDC - Mariana Resumeapi-400182774No ratings yet
- 3 CHED Memorandum No.13 S. 2017 (Print Copy)Document51 pages3 CHED Memorandum No.13 S. 2017 (Print Copy)REYMAR VICU BRAVONo ratings yet
- HMIS User ManualDocument89 pagesHMIS User ManualDelelegn EmwodewNo ratings yet
- Colon CancerDocument14 pagesColon CancerCherrymae BenzonNo ratings yet