
DOSH Medical Evaluation Questionnaire Employer Instructions
DOSH Medical Evaluation Questionnaire Employer Instructions
You might also like
- Height Pass and Vertigo Test Report FormatDocument2 pagesHeight Pass and Vertigo Test Report Formatsyed khaja misbhuddin75% (4)
- Bultonoon PatDocument1 pageBultonoon PatErrol Llanes100% (1)
- Osha Appendix CDocument7 pagesOsha Appendix CGermán Cárdenas AlvarezNo ratings yet
- Respirator Medical Evaluation Questionnaire: To Be Filled Out by The EmployeeDocument5 pagesRespirator Medical Evaluation Questionnaire: To Be Filled Out by The Employeerustynail35209No ratings yet
- Pre-Employment OSHA Questionnaire 06.23.2022 PACE. WINDA 4Document2 pagesPre-Employment OSHA Questionnaire 06.23.2022 PACE. WINDA 4Joseph ThomasNo ratings yet
- Northwell Direct - Respirator Medical Evaluation QuestionnaireDocument5 pagesNorthwell Direct - Respirator Medical Evaluation QuestionnaireFaithNo ratings yet
- Attachment A - OSHA Questionnaire 29 CFR 1910.134, Appendix CDocument10 pagesAttachment A - OSHA Questionnaire 29 CFR 1910.134, Appendix CDarryl BrittNo ratings yet
- OSHA's Respirator Medical QuestionnaireDocument7 pagesOSHA's Respirator Medical QuestionnaireJeffNo ratings yet
- Annexure 1Document2 pagesAnnexure 1math anuNo ratings yet
- Revised-PhilPEN-12 28 18Document1 pageRevised-PhilPEN-12 28 18Kristine TanNo ratings yet
- CVD NCD Risk Assessment FormDocument2 pagesCVD NCD Risk Assessment Formsmoothp3akNo ratings yet
- Respiratory Assessment Form: Miner IdentificationDocument2 pagesRespiratory Assessment Form: Miner IdentificationMikaela Eris CortelloNo ratings yet
- Adakah Anda Mengalami Gejala-Gejala Respiratori Berikut?Document3 pagesAdakah Anda Mengalami Gejala-Gejala Respiratori Berikut?Eu JinnNo ratings yet
- Facility Risk Assessment Form v.2Document1 pageFacility Risk Assessment Form v.2Errol Llanes100% (1)
- ProposaForm Questionniare Linked CHRDocument1 pageProposaForm Questionniare Linked CHRPrachi DubeyNo ratings yet
- Facility Risk Assessement Form 2016Document1 pageFacility Risk Assessement Form 2016kojiki67% (3)
- 5.intertanko Health DeclarationDocument1 page5.intertanko Health DeclarationJohanna Catalan CantonesNo ratings yet
- Respiratory QuestionnaireDocument14 pagesRespiratory QuestionnaireFirsty Demy ChristantiNo ratings yet
- Screening Tool ColourDocument1 pageScreening Tool ColourMuhammad RamlanNo ratings yet
- Pre-Op Health History Questionnaire (Interactive PDFDocument6 pagesPre-Op Health History Questionnaire (Interactive PDFBrenda RaymondNo ratings yet
- FormatDocument3 pagesFormatchiragNo ratings yet
- Medical HistoryDocument3 pagesMedical HistorydjoiajgNo ratings yet
- Global COVID-19 Clinical PlatformDocument8 pagesGlobal COVID-19 Clinical PlatformMaria Do SocorroNo ratings yet
- Declaration - Return To Work Form (Covid 19) : EmployeeDocument2 pagesDeclaration - Return To Work Form (Covid 19) : EmployeeFahad Khalid100% (1)
- Interstitial Diffuse Lung Disease Patient QuestionnaireDocument4 pagesInterstitial Diffuse Lung Disease Patient QuestionnaireJamban08No ratings yet
- Case Study Comprehensive Geriatric AssessmentDocument15 pagesCase Study Comprehensive Geriatric Assessmentinfinite maskedNo ratings yet
- I. Confidential Medical Report Ii. Laboratory Report Iii. X-Ray FormDocument9 pagesI. Confidential Medical Report Ii. Laboratory Report Iii. X-Ray FormAlex BensonNo ratings yet
- Questions: Assessment of The Thorax and Lungs, Heart and Central Vessels, Peripheral Vascular System, Breast and AxillaeDocument1 pageQuestions: Assessment of The Thorax and Lungs, Heart and Central Vessels, Peripheral Vascular System, Breast and AxillaeHylerr PanggalatomNo ratings yet
- Anglo - Eastern Fleet Personnel Division Health Declaration FormDocument1 pageAnglo - Eastern Fleet Personnel Division Health Declaration Formamit kumarNo ratings yet
- Radio Medical RecordDocument6 pagesRadio Medical Recordanshul_sharma_5No ratings yet
- Medif Information Sheet For Passengers Requiring Medical Clearence - Part 1-2 - Tarom From 4122 - 2Document2 pagesMedif Information Sheet For Passengers Requiring Medical Clearence - Part 1-2 - Tarom From 4122 - 2ViolleteMorenaNo ratings yet
- BHHP 7-9 PDFDocument1 pageBHHP 7-9 PDFSiti MasturaNo ratings yet
- Health Declaration Form: Borang Pengisytiharan KesihatanDocument1 pageHealth Declaration Form: Borang Pengisytiharan Kesihatanhasan mamatNo ratings yet
- Screening FormDocument2 pagesScreening FormMarie I. RosalesNo ratings yet
- Declaration Initial IllnessDocument1 pageDeclaration Initial IllnessFahad KhalidNo ratings yet
- Medical History Questionnaire 01Document5 pagesMedical History Questionnaire 01Cleidy Claudio BanegasNo ratings yet
- MIT Medical Department Pediatrics History Form: AppointmentDocument5 pagesMIT Medical Department Pediatrics History Form: AppointmentGee Angela ZozobradoNo ratings yet
- Booty Fitness Par-Q & Liability Waiver: MEDICAL HISTORY (Please Circle Your Answers)Document1 pageBooty Fitness Par-Q & Liability Waiver: MEDICAL HISTORY (Please Circle Your Answers)api-192899910No ratings yet
- 25 3 2013 05 01 Pathare 200536 sdc1Document3 pages25 3 2013 05 01 Pathare 200536 sdc1Jenny Lyne LisayenNo ratings yet
- NCD Risk Assessment FormDocument1 pageNCD Risk Assessment Formruiza corcino100% (4)
- Au Pair Medical Record Verification FormDocument2 pagesAu Pair Medical Record Verification FormSamir Antonio Garcia BarrancoNo ratings yet
- HDF For MDC Projects Version 06052020Document1 pageHDF For MDC Projects Version 06052020Jude Bon Albao0% (1)
- Health CheckDocument9 pagesHealth Checkamoon08.arNo ratings yet
- Respiratory Distress Case ScenarioDocument23 pagesRespiratory Distress Case ScenarioRakeesh VeeraNo ratings yet
- OBGDocument112 pagesOBGNurlaily Sofia NazleeNo ratings yet
- Mimay MimaropaDocument1 pageMimay MimaropaErrol LlanesNo ratings yet
- Caregiving ExamDocument7 pagesCaregiving ExamMaiko TyNo ratings yet
- Borang Isytihar Kesihatan Fasa 3Document1 pageBorang Isytihar Kesihatan Fasa 3faris zainuddinNo ratings yet
- Kuesioner MenstruasiDocument7 pagesKuesioner MenstruasirerenNo ratings yet
- DiabetesDocument2 pagesDiabetessudhanshugst123No ratings yet
- NSG 120 Patient Care Plan ProjectDocument25 pagesNSG 120 Patient Care Plan Projectgodfreykaruku21No ratings yet
- Islamia College, Peshawar (Icp) Department of Zoology Thyroid Gland Health Assessement QuestionareDocument2 pagesIslamia College, Peshawar (Icp) Department of Zoology Thyroid Gland Health Assessement QuestionareJalil Hijazi AjsNo ratings yet
- Practical Exam Video Submission Instruction Guide Update-2Document10 pagesPractical Exam Video Submission Instruction Guide Update-2Personal TrainerNo ratings yet
- Dizziness Questionnaire: Name - DateDocument2 pagesDizziness Questionnaire: Name - DateRavi VarakalaNo ratings yet
- Chaitanya Godavari Grameena Bank:: Head Office:: Guntur Medical Examination ReportDocument2 pagesChaitanya Godavari Grameena Bank:: Head Office:: Guntur Medical Examination ReportbajibabuNo ratings yet
- COVID-19 Screening Form ... : Patient's Name: Date: DateDocument2 pagesCOVID-19 Screening Form ... : Patient's Name: Date: DateMichaelaKatrinaTrinidadNo ratings yet
- Wa0009.Document1 pageWa0009.enterluqNo ratings yet
- Dental and Medical History FormDocument1 pageDental and Medical History FormBon QuiapoNo ratings yet
- Compre 2018 Ipd 111-150Document9 pagesCompre 2018 Ipd 111-150Lemuel ValerioNo ratings yet
- Diaphragm Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiaphragm Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Ijlssr 1164 10 2015 PDFDocument4 pagesIjlssr 1164 10 2015 PDFmeiutaNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Gangguan Fungsi Paru Pada Pekerja Pembuat Kasur (Studi Kasus Di Desa Banjarkerta Karanganyar Purbalingga)Document5 pagesFaktor-Faktor Yang Berhubungan Dengan Gangguan Fungsi Paru Pada Pekerja Pembuat Kasur (Studi Kasus Di Desa Banjarkerta Karanganyar Purbalingga)meiutaNo ratings yet
- The Peak Ow Meter and Its Use in Clinical Practice: January 2011Document5 pagesThe Peak Ow Meter and Its Use in Clinical Practice: January 2011meiutaNo ratings yet
- Evaluating Individual and Program Outcomes: Clinical PearlsDocument1 pageEvaluating Individual and Program Outcomes: Clinical PearlsmeiutaNo ratings yet
- Primary Spontaneous Pneumothorax: Why All The Confusion Over First-Line Treatment?Document4 pagesPrimary Spontaneous Pneumothorax: Why All The Confusion Over First-Line Treatment?meiutaNo ratings yet
- Benzene Exposure Among Auto-Repair Workers From Workplace Ambience: A Pioneer Study From PakistanDocument10 pagesBenzene Exposure Among Auto-Repair Workers From Workplace Ambience: A Pioneer Study From PakistanmeiutaNo ratings yet
- Update On The Diagnosis and Treatment of Tracheal and Bronchial InjuryDocument7 pagesUpdate On The Diagnosis and Treatment of Tracheal and Bronchial InjurymeiutaNo ratings yet
- Bianda Axanditya 22010110130181 Bab2ktiDocument10 pagesBianda Axanditya 22010110130181 Bab2ktimeiutaNo ratings yet
- Dok Baru 2019-06-15 16.02.17 PDFDocument4 pagesDok Baru 2019-06-15 16.02.17 PDFmeiutaNo ratings yet
- Scanned With CamscannerDocument6 pagesScanned With CamscannermeiutaNo ratings yet
- The Regulation of Sleep and Wakefulness by The Hypothalamic Neuropeptide Orexin/HypocretinDocument8 pagesThe Regulation of Sleep and Wakefulness by The Hypothalamic Neuropeptide Orexin/HypocretinmeiutaNo ratings yet
- MedEdicus Insomnia CME and Test Questions PDFDocument20 pagesMedEdicus Insomnia CME and Test Questions PDFmeiutaNo ratings yet
- Sleep and Sleep Disorders: Velayudhan Mohan KumarDocument8 pagesSleep and Sleep Disorders: Velayudhan Mohan KumarmeiutaNo ratings yet
- 7217 Nihms690005Document17 pages7217 Nihms690005meiutaNo ratings yet
- Parasomnias: Wisconsin Medical JournalDocument5 pagesParasomnias: Wisconsin Medical JournalmeiutaNo ratings yet
- Roth2007 PDFDocument9 pagesRoth2007 PDFmeiutaNo ratings yet
- Riginal Rticle: J. O. Adeniran, J. O. Taiwo, L. O. Abdur-RahmanDocument4 pagesRiginal Rticle: J. O. Adeniran, J. O. Taiwo, L. O. Abdur-RahmanmeiutaNo ratings yet
- 02 - SegurançaDocument91 pages02 - SegurançaBelmiro BernardoNo ratings yet
- Sebu8224-08-00-3500c Omm-2014 PDFDocument160 pagesSebu8224-08-00-3500c Omm-2014 PDFMartin Franco100% (2)
- Safety Mobil Dte 24Document9 pagesSafety Mobil Dte 24Emrah BinayNo ratings yet
- Red Dye SDSDocument20 pagesRed Dye SDSalphadingNo ratings yet
- Kwik Grip Spray Adhesive: Material Safety Data SheetDocument8 pagesKwik Grip Spray Adhesive: Material Safety Data Sheetemre sönmezNo ratings yet
- Hempadur Mastic 45889: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingDocument9 pagesHempadur Mastic 45889: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingEmre ÖzbilgiNo ratings yet
- Cloralex Max MsdsDocument6 pagesCloralex Max MsdsnaranjerosNo ratings yet
- DPI PPE For Schools COVID VersionDocument43 pagesDPI PPE For Schools COVID VersionJitesh ThakurNo ratings yet
- SDS - HHI Pyrolysis Oil - Flash Point 10CDocument11 pagesSDS - HHI Pyrolysis Oil - Flash Point 10CKelly LimNo ratings yet
- Material Safety Data Sheet Oct Page 1 of XDocument5 pagesMaterial Safety Data Sheet Oct Page 1 of XMarcus BessinNo ratings yet
- GMP WHO For Hormone Product PDFDocument17 pagesGMP WHO For Hormone Product PDFphamuyenthuNo ratings yet
- Caustic Soda Liquid 48-50%Document12 pagesCaustic Soda Liquid 48-50%wongpengchiong7205No ratings yet
- SC 255435Document12 pagesSC 255435Nguyễn Sỹ Thế AnhNo ratings yet
- 3M 6059 ABEK1 Filter-Data SheetDocument1 page3M 6059 ABEK1 Filter-Data SheetMichael TadrosNo ratings yet
- Molykote G - Rapid PlusDocument9 pagesMolykote G - Rapid PlusNICKYNo ratings yet
- Safety Catalog 2015 Arrange - WurthDocument52 pagesSafety Catalog 2015 Arrange - WurthNithin Basheer50% (2)
- MSDS For PaintDocument10 pagesMSDS For Paintcem jakartaNo ratings yet
- Hempel's Curing Agent 9705000000 En-UsDocument10 pagesHempel's Curing Agent 9705000000 En-UsAnonymous HPlNDhM6ejNo ratings yet
- CGA Air Grade SpecificationsDocument4 pagesCGA Air Grade Specificationsal bauerNo ratings yet
- MSDS Multipox MX-94 Traffic YellowDocument4 pagesMSDS Multipox MX-94 Traffic Yelloweva andriana putriNo ratings yet
- Material Safety Data Sheet: Veolia Water Systems (Gulf) FZCDocument2 pagesMaterial Safety Data Sheet: Veolia Water Systems (Gulf) FZCJHUPEL ABARIAL100% (1)
- MM - 4a.pdf BREAK SYSTEME AXEL TECH PDFDocument16 pagesMM - 4a.pdf BREAK SYSTEME AXEL TECH PDFRachid SmailiNo ratings yet
- Pa66-G30 Ahbk003 Tds-Iso-EngDocument2 pagesPa66-G30 Ahbk003 Tds-Iso-EngVinoth SekarNo ratings yet
- Standard Safety Measures: DefinitionsDocument26 pagesStandard Safety Measures: DefinitionsAnilkumar JaraliNo ratings yet
- TM 9-2350-247-20-1 PDFDocument871 pagesTM 9-2350-247-20-1 PDFsergey62No ratings yet
- Chemical Security Printing IndustryDocument58 pagesChemical Security Printing IndustryaodiseoccNo ratings yet
- Msds - Limpia Contacto 3m 16-101Document8 pagesMsds - Limpia Contacto 3m 16-101Ruth E. Pisco VillavicencioNo ratings yet
- MSDS MaxiguardDocument13 pagesMSDS MaxiguardImran HaqNo ratings yet
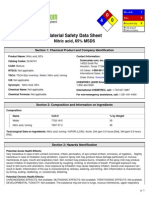
- Nitric Acid, 65% MSDS: Section 1: Chemical Product and Company IdentificationDocument6 pagesNitric Acid, 65% MSDS: Section 1: Chemical Product and Company IdentificationBharat J ShettyNo ratings yet
- Delo 1000 Marine MSDSDocument6 pagesDelo 1000 Marine MSDSPCRNo ratings yet









































































































Download as docx, pdf, or txt
You might also like
- Height Pass and Vertigo Test Report FormatDocument2 pagesHeight Pass and Vertigo Test Report Formatsyed khaja misbhuddin75% (4)
- Bultonoon PatDocument1 pageBultonoon PatErrol Llanes100% (1)
- Osha Appendix CDocument7 pagesOsha Appendix CGermán Cárdenas AlvarezNo ratings yet
- Respirator Medical Evaluation Questionnaire: To Be Filled Out by The EmployeeDocument5 pagesRespirator Medical Evaluation Questionnaire: To Be Filled Out by The Employeerustynail35209No ratings yet
- Pre-Employment OSHA Questionnaire 06.23.2022 PACE. WINDA 4Document2 pagesPre-Employment OSHA Questionnaire 06.23.2022 PACE. WINDA 4Joseph ThomasNo ratings yet
- Northwell Direct - Respirator Medical Evaluation QuestionnaireDocument5 pagesNorthwell Direct - Respirator Medical Evaluation QuestionnaireFaithNo ratings yet
- Attachment A - OSHA Questionnaire 29 CFR 1910.134, Appendix CDocument10 pagesAttachment A - OSHA Questionnaire 29 CFR 1910.134, Appendix CDarryl BrittNo ratings yet
- OSHA's Respirator Medical QuestionnaireDocument7 pagesOSHA's Respirator Medical QuestionnaireJeffNo ratings yet
- Annexure 1Document2 pagesAnnexure 1math anuNo ratings yet
- Revised-PhilPEN-12 28 18Document1 pageRevised-PhilPEN-12 28 18Kristine TanNo ratings yet
- CVD NCD Risk Assessment FormDocument2 pagesCVD NCD Risk Assessment Formsmoothp3akNo ratings yet
- Respiratory Assessment Form: Miner IdentificationDocument2 pagesRespiratory Assessment Form: Miner IdentificationMikaela Eris CortelloNo ratings yet
- Adakah Anda Mengalami Gejala-Gejala Respiratori Berikut?Document3 pagesAdakah Anda Mengalami Gejala-Gejala Respiratori Berikut?Eu JinnNo ratings yet
- Facility Risk Assessment Form v.2Document1 pageFacility Risk Assessment Form v.2Errol Llanes100% (1)
- ProposaForm Questionniare Linked CHRDocument1 pageProposaForm Questionniare Linked CHRPrachi DubeyNo ratings yet
- Facility Risk Assessement Form 2016Document1 pageFacility Risk Assessement Form 2016kojiki67% (3)
- 5.intertanko Health DeclarationDocument1 page5.intertanko Health DeclarationJohanna Catalan CantonesNo ratings yet
- Respiratory QuestionnaireDocument14 pagesRespiratory QuestionnaireFirsty Demy ChristantiNo ratings yet
- Screening Tool ColourDocument1 pageScreening Tool ColourMuhammad RamlanNo ratings yet
- Pre-Op Health History Questionnaire (Interactive PDFDocument6 pagesPre-Op Health History Questionnaire (Interactive PDFBrenda RaymondNo ratings yet
- FormatDocument3 pagesFormatchiragNo ratings yet
- Medical HistoryDocument3 pagesMedical HistorydjoiajgNo ratings yet
- Global COVID-19 Clinical PlatformDocument8 pagesGlobal COVID-19 Clinical PlatformMaria Do SocorroNo ratings yet
- Declaration - Return To Work Form (Covid 19) : EmployeeDocument2 pagesDeclaration - Return To Work Form (Covid 19) : EmployeeFahad Khalid100% (1)
- Interstitial Diffuse Lung Disease Patient QuestionnaireDocument4 pagesInterstitial Diffuse Lung Disease Patient QuestionnaireJamban08No ratings yet
- Case Study Comprehensive Geriatric AssessmentDocument15 pagesCase Study Comprehensive Geriatric Assessmentinfinite maskedNo ratings yet
- I. Confidential Medical Report Ii. Laboratory Report Iii. X-Ray FormDocument9 pagesI. Confidential Medical Report Ii. Laboratory Report Iii. X-Ray FormAlex BensonNo ratings yet
- Questions: Assessment of The Thorax and Lungs, Heart and Central Vessels, Peripheral Vascular System, Breast and AxillaeDocument1 pageQuestions: Assessment of The Thorax and Lungs, Heart and Central Vessels, Peripheral Vascular System, Breast and AxillaeHylerr PanggalatomNo ratings yet
- Anglo - Eastern Fleet Personnel Division Health Declaration FormDocument1 pageAnglo - Eastern Fleet Personnel Division Health Declaration Formamit kumarNo ratings yet
- Radio Medical RecordDocument6 pagesRadio Medical Recordanshul_sharma_5No ratings yet
- Medif Information Sheet For Passengers Requiring Medical Clearence - Part 1-2 - Tarom From 4122 - 2Document2 pagesMedif Information Sheet For Passengers Requiring Medical Clearence - Part 1-2 - Tarom From 4122 - 2ViolleteMorenaNo ratings yet
- BHHP 7-9 PDFDocument1 pageBHHP 7-9 PDFSiti MasturaNo ratings yet
- Health Declaration Form: Borang Pengisytiharan KesihatanDocument1 pageHealth Declaration Form: Borang Pengisytiharan Kesihatanhasan mamatNo ratings yet
- Screening FormDocument2 pagesScreening FormMarie I. RosalesNo ratings yet
- Declaration Initial IllnessDocument1 pageDeclaration Initial IllnessFahad KhalidNo ratings yet
- Medical History Questionnaire 01Document5 pagesMedical History Questionnaire 01Cleidy Claudio BanegasNo ratings yet
- MIT Medical Department Pediatrics History Form: AppointmentDocument5 pagesMIT Medical Department Pediatrics History Form: AppointmentGee Angela ZozobradoNo ratings yet
- Booty Fitness Par-Q & Liability Waiver: MEDICAL HISTORY (Please Circle Your Answers)Document1 pageBooty Fitness Par-Q & Liability Waiver: MEDICAL HISTORY (Please Circle Your Answers)api-192899910No ratings yet
- 25 3 2013 05 01 Pathare 200536 sdc1Document3 pages25 3 2013 05 01 Pathare 200536 sdc1Jenny Lyne LisayenNo ratings yet
- NCD Risk Assessment FormDocument1 pageNCD Risk Assessment Formruiza corcino100% (4)
- Au Pair Medical Record Verification FormDocument2 pagesAu Pair Medical Record Verification FormSamir Antonio Garcia BarrancoNo ratings yet
- HDF For MDC Projects Version 06052020Document1 pageHDF For MDC Projects Version 06052020Jude Bon Albao0% (1)
- Health CheckDocument9 pagesHealth Checkamoon08.arNo ratings yet
- Respiratory Distress Case ScenarioDocument23 pagesRespiratory Distress Case ScenarioRakeesh VeeraNo ratings yet
- OBGDocument112 pagesOBGNurlaily Sofia NazleeNo ratings yet
- Mimay MimaropaDocument1 pageMimay MimaropaErrol LlanesNo ratings yet
- Caregiving ExamDocument7 pagesCaregiving ExamMaiko TyNo ratings yet
- Borang Isytihar Kesihatan Fasa 3Document1 pageBorang Isytihar Kesihatan Fasa 3faris zainuddinNo ratings yet
- Kuesioner MenstruasiDocument7 pagesKuesioner MenstruasirerenNo ratings yet
- DiabetesDocument2 pagesDiabetessudhanshugst123No ratings yet
- NSG 120 Patient Care Plan ProjectDocument25 pagesNSG 120 Patient Care Plan Projectgodfreykaruku21No ratings yet
- Islamia College, Peshawar (Icp) Department of Zoology Thyroid Gland Health Assessement QuestionareDocument2 pagesIslamia College, Peshawar (Icp) Department of Zoology Thyroid Gland Health Assessement QuestionareJalil Hijazi AjsNo ratings yet
- Practical Exam Video Submission Instruction Guide Update-2Document10 pagesPractical Exam Video Submission Instruction Guide Update-2Personal TrainerNo ratings yet
- Dizziness Questionnaire: Name - DateDocument2 pagesDizziness Questionnaire: Name - DateRavi VarakalaNo ratings yet
- Chaitanya Godavari Grameena Bank:: Head Office:: Guntur Medical Examination ReportDocument2 pagesChaitanya Godavari Grameena Bank:: Head Office:: Guntur Medical Examination ReportbajibabuNo ratings yet
- COVID-19 Screening Form ... : Patient's Name: Date: DateDocument2 pagesCOVID-19 Screening Form ... : Patient's Name: Date: DateMichaelaKatrinaTrinidadNo ratings yet
- Wa0009.Document1 pageWa0009.enterluqNo ratings yet
- Dental and Medical History FormDocument1 pageDental and Medical History FormBon QuiapoNo ratings yet
- Compre 2018 Ipd 111-150Document9 pagesCompre 2018 Ipd 111-150Lemuel ValerioNo ratings yet
- Diaphragm Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiaphragm Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Ijlssr 1164 10 2015 PDFDocument4 pagesIjlssr 1164 10 2015 PDFmeiutaNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Gangguan Fungsi Paru Pada Pekerja Pembuat Kasur (Studi Kasus Di Desa Banjarkerta Karanganyar Purbalingga)Document5 pagesFaktor-Faktor Yang Berhubungan Dengan Gangguan Fungsi Paru Pada Pekerja Pembuat Kasur (Studi Kasus Di Desa Banjarkerta Karanganyar Purbalingga)meiutaNo ratings yet
- The Peak Ow Meter and Its Use in Clinical Practice: January 2011Document5 pagesThe Peak Ow Meter and Its Use in Clinical Practice: January 2011meiutaNo ratings yet
- Evaluating Individual and Program Outcomes: Clinical PearlsDocument1 pageEvaluating Individual and Program Outcomes: Clinical PearlsmeiutaNo ratings yet
- Primary Spontaneous Pneumothorax: Why All The Confusion Over First-Line Treatment?Document4 pagesPrimary Spontaneous Pneumothorax: Why All The Confusion Over First-Line Treatment?meiutaNo ratings yet
- Benzene Exposure Among Auto-Repair Workers From Workplace Ambience: A Pioneer Study From PakistanDocument10 pagesBenzene Exposure Among Auto-Repair Workers From Workplace Ambience: A Pioneer Study From PakistanmeiutaNo ratings yet
- Update On The Diagnosis and Treatment of Tracheal and Bronchial InjuryDocument7 pagesUpdate On The Diagnosis and Treatment of Tracheal and Bronchial InjurymeiutaNo ratings yet
- Bianda Axanditya 22010110130181 Bab2ktiDocument10 pagesBianda Axanditya 22010110130181 Bab2ktimeiutaNo ratings yet
- Dok Baru 2019-06-15 16.02.17 PDFDocument4 pagesDok Baru 2019-06-15 16.02.17 PDFmeiutaNo ratings yet
- Scanned With CamscannerDocument6 pagesScanned With CamscannermeiutaNo ratings yet
- The Regulation of Sleep and Wakefulness by The Hypothalamic Neuropeptide Orexin/HypocretinDocument8 pagesThe Regulation of Sleep and Wakefulness by The Hypothalamic Neuropeptide Orexin/HypocretinmeiutaNo ratings yet
- MedEdicus Insomnia CME and Test Questions PDFDocument20 pagesMedEdicus Insomnia CME and Test Questions PDFmeiutaNo ratings yet
- Sleep and Sleep Disorders: Velayudhan Mohan KumarDocument8 pagesSleep and Sleep Disorders: Velayudhan Mohan KumarmeiutaNo ratings yet
- 7217 Nihms690005Document17 pages7217 Nihms690005meiutaNo ratings yet
- Parasomnias: Wisconsin Medical JournalDocument5 pagesParasomnias: Wisconsin Medical JournalmeiutaNo ratings yet
- Roth2007 PDFDocument9 pagesRoth2007 PDFmeiutaNo ratings yet
- Riginal Rticle: J. O. Adeniran, J. O. Taiwo, L. O. Abdur-RahmanDocument4 pagesRiginal Rticle: J. O. Adeniran, J. O. Taiwo, L. O. Abdur-RahmanmeiutaNo ratings yet
- 02 - SegurançaDocument91 pages02 - SegurançaBelmiro BernardoNo ratings yet
- Sebu8224-08-00-3500c Omm-2014 PDFDocument160 pagesSebu8224-08-00-3500c Omm-2014 PDFMartin Franco100% (2)
- Safety Mobil Dte 24Document9 pagesSafety Mobil Dte 24Emrah BinayNo ratings yet
- Red Dye SDSDocument20 pagesRed Dye SDSalphadingNo ratings yet
- Kwik Grip Spray Adhesive: Material Safety Data SheetDocument8 pagesKwik Grip Spray Adhesive: Material Safety Data Sheetemre sönmezNo ratings yet
- Hempadur Mastic 45889: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingDocument9 pagesHempadur Mastic 45889: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingEmre ÖzbilgiNo ratings yet
- Cloralex Max MsdsDocument6 pagesCloralex Max MsdsnaranjerosNo ratings yet
- DPI PPE For Schools COVID VersionDocument43 pagesDPI PPE For Schools COVID VersionJitesh ThakurNo ratings yet
- SDS - HHI Pyrolysis Oil - Flash Point 10CDocument11 pagesSDS - HHI Pyrolysis Oil - Flash Point 10CKelly LimNo ratings yet
- Material Safety Data Sheet Oct Page 1 of XDocument5 pagesMaterial Safety Data Sheet Oct Page 1 of XMarcus BessinNo ratings yet
- GMP WHO For Hormone Product PDFDocument17 pagesGMP WHO For Hormone Product PDFphamuyenthuNo ratings yet
- Caustic Soda Liquid 48-50%Document12 pagesCaustic Soda Liquid 48-50%wongpengchiong7205No ratings yet
- SC 255435Document12 pagesSC 255435Nguyễn Sỹ Thế AnhNo ratings yet
- 3M 6059 ABEK1 Filter-Data SheetDocument1 page3M 6059 ABEK1 Filter-Data SheetMichael TadrosNo ratings yet
- Molykote G - Rapid PlusDocument9 pagesMolykote G - Rapid PlusNICKYNo ratings yet
- Safety Catalog 2015 Arrange - WurthDocument52 pagesSafety Catalog 2015 Arrange - WurthNithin Basheer50% (2)
- MSDS For PaintDocument10 pagesMSDS For Paintcem jakartaNo ratings yet
- Hempel's Curing Agent 9705000000 En-UsDocument10 pagesHempel's Curing Agent 9705000000 En-UsAnonymous HPlNDhM6ejNo ratings yet
- CGA Air Grade SpecificationsDocument4 pagesCGA Air Grade Specificationsal bauerNo ratings yet
- MSDS Multipox MX-94 Traffic YellowDocument4 pagesMSDS Multipox MX-94 Traffic Yelloweva andriana putriNo ratings yet
- Material Safety Data Sheet: Veolia Water Systems (Gulf) FZCDocument2 pagesMaterial Safety Data Sheet: Veolia Water Systems (Gulf) FZCJHUPEL ABARIAL100% (1)
- MM - 4a.pdf BREAK SYSTEME AXEL TECH PDFDocument16 pagesMM - 4a.pdf BREAK SYSTEME AXEL TECH PDFRachid SmailiNo ratings yet
- Pa66-G30 Ahbk003 Tds-Iso-EngDocument2 pagesPa66-G30 Ahbk003 Tds-Iso-EngVinoth SekarNo ratings yet
- Standard Safety Measures: DefinitionsDocument26 pagesStandard Safety Measures: DefinitionsAnilkumar JaraliNo ratings yet
- TM 9-2350-247-20-1 PDFDocument871 pagesTM 9-2350-247-20-1 PDFsergey62No ratings yet
- Chemical Security Printing IndustryDocument58 pagesChemical Security Printing IndustryaodiseoccNo ratings yet
- Msds - Limpia Contacto 3m 16-101Document8 pagesMsds - Limpia Contacto 3m 16-101Ruth E. Pisco VillavicencioNo ratings yet
- MSDS MaxiguardDocument13 pagesMSDS MaxiguardImran HaqNo ratings yet
- Nitric Acid, 65% MSDS: Section 1: Chemical Product and Company IdentificationDocument6 pagesNitric Acid, 65% MSDS: Section 1: Chemical Product and Company IdentificationBharat J ShettyNo ratings yet
- Delo 1000 Marine MSDSDocument6 pagesDelo 1000 Marine MSDSPCRNo ratings yet