Download as pdf or txt
You might also like
- CH250 Service Manual Version BDocument97 pagesCH250 Service Manual Version BSherin Rajan100% (12)
- Autism and AstrologyDocument9 pagesAutism and AstrologyJatinder Sandhu100% (1)
- DVP R Test PlanDocument2 pagesDVP R Test PlandavidNo ratings yet
- Dolby Technical Guidelines 1994Document0 pagesDolby Technical Guidelines 1994Shrwanda ShrwandaNo ratings yet
- Twilight Alice's POV Chapters 1-29Document102 pagesTwilight Alice's POV Chapters 1-29Sarah Yerkey100% (5)
- 4 Exposure Criteria, Occupational Exposure LevelsDocument24 pages4 Exposure Criteria, Occupational Exposure LevelsTunjungsNo ratings yet
- Ficha Tecnica CassiaDocument6 pagesFicha Tecnica CassiaLUISA MARCELA SANCHEZ AGUIRRENo ratings yet
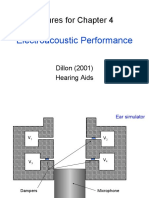
- Figures For Chapter 4: Electroacoustic PerformanceDocument23 pagesFigures For Chapter 4: Electroacoustic PerformanceTaegan YoungNo ratings yet
- Interpreting Spinorama Charts PDFDocument25 pagesInterpreting Spinorama Charts PDFjorge etayoNo ratings yet
- Esc201t l17 LCR FilterDocument36 pagesEsc201t l17 LCR FilterRachit MahajanNo ratings yet
- Materials 16 01879 v2Document23 pagesMaterials 16 01879 v2slavceNo ratings yet
- Audiometry Report Sibelmed W50: 125 250 500 1K 2K 4K 8K (HZ) 10 0 - 10 125 250 500 1K 2K 4K 8K (HZ) 10 0 - 10Document1 pageAudiometry Report Sibelmed W50: 125 250 500 1K 2K 4K 8K (HZ) 10 0 - 10 125 250 500 1K 2K 4K 8K (HZ) 10 0 - 10Boca PetualangNo ratings yet
- Iso 1999-Liedtke EJEMPLODocument4 pagesIso 1999-Liedtke EJEMPLOJM OccupationalNo ratings yet
- Zanden Model 1000 Stereo Equalizer AmplifierDocument2 pagesZanden Model 1000 Stereo Equalizer AmplifierEnrique PalacioNo ratings yet
- Formula Masking 1Document111 pagesFormula Masking 1Caroline RochaNo ratings yet
- Sound Control: Where Glass Becomes ArchitectureDocument6 pagesSound Control: Where Glass Becomes ArchitectureLeonel VelasquezNo ratings yet
- ASA 144 Cancun29NovliteDocument21 pagesASA 144 Cancun29NovliteVangelis ApostolouNo ratings yet
- Speech Signal Analysis and Coding: Dr. Arun KumarDocument52 pagesSpeech Signal Analysis and Coding: Dr. Arun KumarHoang Duong Quy RomNo ratings yet
- New Count The DotsDocument1 pageNew Count The Dotslin ee100% (1)
- Arif Wibowo-1Document1 pageArif Wibowo-1Boca PetualangNo ratings yet
- PrasutiyoDocument1 pagePrasutiyoBoca PetualangNo ratings yet
- Suhard IDocument1 pageSuhard IBoca PetualangNo ratings yet
- Ade IrawanDocument1 pageAde IrawanBoca PetualangNo ratings yet
- 1 - INIZIA 1 Product InformationDocument8 pages1 - INIZIA 1 Product InformationFerko YU7BXNo ratings yet
- Kuluk AsrialDocument1 pageKuluk AsrialBoca PetualangNo ratings yet
- AKG C422, C34, C33 Stereophonic Condenser MicrophonesDocument4 pagesAKG C422, C34, C33 Stereophonic Condenser MicrophonesMario CrispiNo ratings yet
- Reflex Horn Speakers: TC-630/TC-630M TC-615/TC-615MDocument4 pagesReflex Horn Speakers: TC-630/TC-630M TC-615/TC-615MEdison MendozaNo ratings yet
- Rangga Saputra-1Document1 pageRangga Saputra-1Boca PetualangNo ratings yet
- Sardi 1Document1 pageSardi 1Boca PetualangNo ratings yet
- Nadlif Muammar KH KhumainiDocument1 pageNadlif Muammar KH KhumainiBoca PetualangNo ratings yet
- Universal Twu1.5-Technical SheetDocument1 pageUniversal Twu1.5-Technical SheetCruz ArangoNo ratings yet
- HHHHDocument1 pageHHHHBoca PetualangNo ratings yet
- Acoustic Emission Health Monitoring of Steel BridgesDocument9 pagesAcoustic Emission Health Monitoring of Steel BridgesPrateek NegiNo ratings yet
- HidayatullahDocument1 pageHidayatullahBoca PetualangNo ratings yet
- Rully Mardianto-1Document1 pageRully Mardianto-1Boca PetualangNo ratings yet
- DarwotoDocument1 pageDarwotoBoca PetualangNo ratings yet
- Khoirul HidayatDocument1 pageKhoirul HidayatBoca PetualangNo ratings yet
- Rudyi Wahyu OrabowoDocument1 pageRudyi Wahyu OrabowoBoca PetualangNo ratings yet
- Iwan EndrasmoroDocument1 pageIwan EndrasmoroBoca PetualangNo ratings yet
- Andika Saputra-1Document1 pageAndika Saputra-1Boca PetualangNo ratings yet
- Eval Adf4118eb1Document6 pagesEval Adf4118eb1Everton Klinger Sousa SilvaNo ratings yet
- Eval Adf411xeb1Document6 pagesEval Adf411xeb1Everton Klinger Sousa SilvaNo ratings yet
- Gozali Purba KusumaDocument1 pageGozali Purba KusumaBoca PetualangNo ratings yet
- Vfo With SiDocument16 pagesVfo With SiToplician AdrianNo ratings yet
- Not All Dynamic Pressure Transducers Are Microphones!: Chad M Walber Ph.D. Research and DevelopmentDocument19 pagesNot All Dynamic Pressure Transducers Are Microphones!: Chad M Walber Ph.D. Research and DevelopmentGabriel Jérôme Vargas MoyaNo ratings yet
- Anil Kumar AudiometryDocument1 pageAnil Kumar AudiometryRavi Kiran NNo ratings yet
- Line 6 Guide To Mic Models: Electrophonic Limited Edition - Rev CDocument6 pagesLine 6 Guide To Mic Models: Electrophonic Limited Edition - Rev CDarko VrhovacNo ratings yet
- Et80, Et1010, Et1080Document4 pagesEt80, Et1010, Et1080KUNONo ratings yet
- M. Tamin-1Document1 pageM. Tamin-1Boca PetualangNo ratings yet
- Eca DesmawarniDocument1 pageEca DesmawarniBoca PetualangNo ratings yet
- Binson Echorec Schematic - EffectrodeDocument12 pagesBinson Echorec Schematic - EffectrodetrancegodzNo ratings yet
- 849 Guide en-USDocument12 pages849 Guide en-USMisu NguyenNo ratings yet
- KlsynmanDocument22 pagesKlsynmangargoylingNo ratings yet
- Eliya AriscaDocument1 pageEliya AriscaBoca PetualangNo ratings yet
- 2006 RAE4 X-Prep1Document11 pages2006 RAE4 X-Prep1AdrianNo ratings yet
- Diseño Interior - Junio 2017 PDFDocument147 pagesDiseño Interior - Junio 2017 PDFInter GomezNo ratings yet
- Scalacoustic FTDocument2 pagesScalacoustic FTCiro Nero MaguleNo ratings yet
- Part Ix: Reactive Silencers: Industrial Noise SeriesDocument8 pagesPart Ix: Reactive Silencers: Industrial Noise SeriesRaja Sekaran SajjaNo ratings yet
- Ceiling Speaker LC3 - Data - Sheet - enUS - 1920773259Document4 pagesCeiling Speaker LC3 - Data - Sheet - enUS - 1920773259Hernawan fAJARNo ratings yet
- Lo Verde Dong Comparingmethodsfordescribinglowfrequencyairborneisolationin ASTMand ISOstandardsDocument8 pagesLo Verde Dong Comparingmethodsfordescribinglowfrequencyairborneisolationin ASTMand ISOstandardsMaría Nahomy Castillo AbrilNo ratings yet
- Multi Band20Antenna20for20Different20Wireless20ApplicationsDocument5 pagesMulti Band20Antenna20for20Different20Wireless20ApplicationsDivamiNo ratings yet
- Tidu 016Document19 pagesTidu 016ZhitaiLiuNo ratings yet
- The Fourth Terminal: Benefits of Body-Biasing Techniques for FDSOI Circuits and SystemsFrom EverandThe Fourth Terminal: Benefits of Body-Biasing Techniques for FDSOI Circuits and SystemsSylvain ClercNo ratings yet
- Experiencia Clinica en El Manejo de Paralisis CordDocument9 pagesExperiencia Clinica en El Manejo de Paralisis CordvaleperoneNo ratings yet
- Goldsmith 2000Document24 pagesGoldsmith 2000valeperoneNo ratings yet
- Preview: Presbyphagia Markers in The Community-Dwelling Elderly PopulationDocument13 pagesPreview: Presbyphagia Markers in The Community-Dwelling Elderly PopulationvaleperoneNo ratings yet
- Swallowing Therapy For Dysphagia in Acute and Subacute StrokeDocument145 pagesSwallowing Therapy For Dysphagia in Acute and Subacute StrokevaleperoneNo ratings yet
- Aerosol Generating Procedures, Dysphagia Assessment and COVID 19 A Rapid ReviewDocument8 pagesAerosol Generating Procedures, Dysphagia Assessment and COVID 19 A Rapid ReviewvaleperoneNo ratings yet
- Presbyphagia Versus Dysphagia: Identifying Age-Related Changes in Swallow FunctionDocument7 pagesPresbyphagia Versus Dysphagia: Identifying Age-Related Changes in Swallow FunctionvaleperoneNo ratings yet
- Advances in Auditory Prostheses: ReviewDocument6 pagesAdvances in Auditory Prostheses: ReviewvaleperoneNo ratings yet
- Manual 1742Document37 pagesManual 1742valeperoneNo ratings yet
- Atheist TestDocument6 pagesAtheist TestDaveNo ratings yet
- Personality Iridology Manual With Cover qr3lzr 41 60Document20 pagesPersonality Iridology Manual With Cover qr3lzr 41 60Sergio GutierrezNo ratings yet
- Intelligence Testing Power PointDocument23 pagesIntelligence Testing Power PointLorri - Ann LamontNo ratings yet
- Progress Report: by Madam Sazuliana SanifDocument8 pagesProgress Report: by Madam Sazuliana Sanifhero100% (1)
- Evaluation Guidelines For Master Teacher Position: Requirements For Demonstration TeachingDocument3 pagesEvaluation Guidelines For Master Teacher Position: Requirements For Demonstration TeachingBraddock Mcgrath Dy100% (1)
- New DLP Math 2Document14 pagesNew DLP Math 2John Paul ArcoNo ratings yet
- Jona Gangan-GURO21 - Action-Plan-Template - VersionDocument2 pagesJona Gangan-GURO21 - Action-Plan-Template - VersionMaria Jonalyn GanganNo ratings yet
- Ventures Transitions Tests and Answer KeyDocument49 pagesVentures Transitions Tests and Answer Keydaniela sanclementeNo ratings yet
- Brain - Based LearningDocument3 pagesBrain - Based LearningRinna HareshNo ratings yet
- Final NCPDocument3 pagesFinal NCPtineeheartNo ratings yet
- Yoon Kim Resume 2018Document1 pageYoon Kim Resume 2018api-313216621No ratings yet
- Early Literacy EducationDocument144 pagesEarly Literacy EducationRené Ponce CarrilloNo ratings yet
- INGLÉS III - Unit 1 - Task 2 - Composition An Environmental FableDocument8 pagesINGLÉS III - Unit 1 - Task 2 - Composition An Environmental FableEstefania Mendoza TrujilloNo ratings yet
- Study Guide For Tanizaki Jun'ichirō "The Secret" (Himitsu, 1911, Tr. A. Chambers)Document3 pagesStudy Guide For Tanizaki Jun'ichirō "The Secret" (Himitsu, 1911, Tr. A. Chambers)BeholdmyswarthyfaceNo ratings yet
- Directory SubmisstionDocument4 pagesDirectory SubmisstionadmyainfotechNo ratings yet
- Waterfall ModelDocument6 pagesWaterfall ModelAswin MageshNo ratings yet
- 09 - Chapter 4 PDFDocument127 pages09 - Chapter 4 PDFApple JamNo ratings yet
- Shri Ram Piston ReportDocument452 pagesShri Ram Piston ReportGaurav PandeyNo ratings yet
- Parkour PDFDocument16 pagesParkour PDFbonengNo ratings yet
- GerundsDocument11 pagesGerundsNitiyanandanathan KamalanathanNo ratings yet
- Clarity+Journal+by+Michele+Lee +a++tDocument18 pagesClarity+Journal+by+Michele+Lee +a++tIrene MartínNo ratings yet
- Syllabus Ecn204 F12Document5 pagesSyllabus Ecn204 F12RobMagooNo ratings yet
- Lesson 2 Variables in ResearchDocument19 pagesLesson 2 Variables in ResearchJake ManzanoNo ratings yet
- Question Bank PSYC F.A Part I 1Document8 pagesQuestion Bank PSYC F.A Part I 1Linda SelvarajNo ratings yet
- End of Term LetterDocument1 pageEnd of Term LetterDiana OstrovanNo ratings yet
- An Analysis of The Influence of Public Relations Department Leadership Style On Public Relations Strategy Use and EffectivenessDocument25 pagesAn Analysis of The Influence of Public Relations Department Leadership Style On Public Relations Strategy Use and EffectivenessmadhurendrahraNo ratings yet
- Blank Mind SyndromeDocument4 pagesBlank Mind SyndromeAnushka JindalNo ratings yet