Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fire Station Design GuideDocument6 pagesFire Station Design GuideAtmrezaNo ratings yet
- Impact of Covid19 On The Indian Stock MarketDocument6 pagesImpact of Covid19 On The Indian Stock MarketB31 Viraj PatilNo ratings yet
- ICO-Ophthalmology Surgical Competency Assessment Rubric-SICS (ICO-OSCAR: SICS)Document3 pagesICO-Ophthalmology Surgical Competency Assessment Rubric-SICS (ICO-OSCAR: SICS)Andi Akhmad FaisalNo ratings yet
- The Effects of Emotion On Short-Term Power Spectrum Analysis of Heart RateDocument5 pagesThe Effects of Emotion On Short-Term Power Spectrum Analysis of Heart RateManuel Guerrero GómezNo ratings yet
- NewDocument17 pagesNewMadhu BalaNo ratings yet
- Technical Datasheet DHFFMDocument2 pagesTechnical Datasheet DHFFMSamerNo ratings yet
- Optic AtrophyDocument34 pagesOptic AtrophySaif BokhariNo ratings yet
- Monitoring The Fermentation of GlucoseDocument4 pagesMonitoring The Fermentation of GlucoseSonia IsaacsNo ratings yet
- S M A R T: 201 A TEST #3 Define and Discuss The Purpose of Outcome IdentificationDocument6 pagesS M A R T: 201 A TEST #3 Define and Discuss The Purpose of Outcome IdentificationLindsay JonesNo ratings yet
- EthicsDocument10 pagesEthicsMadhubala JNo ratings yet
- Analisis Penerapan Metode Activity Based Costing (ABC) Dalam Menentukan Tarif Jasa Rawat Inap Di RSUD Kota PrabumulihDocument12 pagesAnalisis Penerapan Metode Activity Based Costing (ABC) Dalam Menentukan Tarif Jasa Rawat Inap Di RSUD Kota PrabumulihAffira AfriNo ratings yet
- 3.02 Medicina Clínica PDFDocument100 pages3.02 Medicina Clínica PDFCristina Maite Chacon AmayaNo ratings yet
- Life Calling Map Fillable FormDocument2 pagesLife Calling Map Fillable Formapi-300853489No ratings yet
- Kohler Students Scores Tops in The State Again For ACT ScoresDocument20 pagesKohler Students Scores Tops in The State Again For ACT ScoresThe Kohler VillagerNo ratings yet
- Future Biotechnology: The Eurobiotech JournalDocument4 pagesFuture Biotechnology: The Eurobiotech JournalsaraNo ratings yet
- Chris Hemsworth's God-Like Thor WorkoutDocument8 pagesChris Hemsworth's God-Like Thor WorkoutmarticarrerasNo ratings yet
- Vocabulary Set 28 - TAX ON FAST FOODDocument4 pagesVocabulary Set 28 - TAX ON FAST FOODchung hieuNo ratings yet
- Mentor NightDocument13 pagesMentor Nightapi-343161223No ratings yet
- 4.4.3.3 Data and Trend AnalysisDocument6 pages4.4.3.3 Data and Trend AnalysisIndermohan MehtaNo ratings yet
- Zoom For Healthcare: One Platform For Virtual Care & CommunicationDocument2 pagesZoom For Healthcare: One Platform For Virtual Care & CommunicationDespacho virtualNo ratings yet
- Henares Vs LTFRBDocument2 pagesHenares Vs LTFRBCarolina Lim GambanNo ratings yet
- Lec 1disorders of Vascular Flow and ShockDocument91 pagesLec 1disorders of Vascular Flow and ShockMohid AhmedNo ratings yet
- The Manual of Ethiopian Medical History - People To People PDFDocument60 pagesThe Manual of Ethiopian Medical History - People To People PDFShiferaw Biru100% (1)
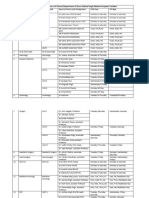
- OPD and OT Days of Doctors of Clinical Department of Guru Gobind Singh Medical HospitalDocument4 pagesOPD and OT Days of Doctors of Clinical Department of Guru Gobind Singh Medical HospitalBohar singh Brar BrarNo ratings yet
- Nestle Edition 10 FullDocument4 pagesNestle Edition 10 FullKaran RawatNo ratings yet
- Cheung2020 PDFDocument15 pagesCheung2020 PDFSandra Milena Cortes SotoNo ratings yet
- Lecture 2 Hope 1Document4 pagesLecture 2 Hope 1cally20smithNo ratings yet
- WEEK 2: 12A, 12B, 12G Ôn Tập Khảo Sát Pronunciation ClosestDocument6 pagesWEEK 2: 12A, 12B, 12G Ôn Tập Khảo Sát Pronunciation ClosestHàNhậtNguyễnNo ratings yet
- Mt. Olive - August 2012-FINALDocument52 pagesMt. Olive - August 2012-FINALjoe9783No ratings yet
- Trojan Battery Company Valve Regulated Lead Acid Battery Safety Data SheetDocument12 pagesTrojan Battery Company Valve Regulated Lead Acid Battery Safety Data SheetNels OdrajafNo ratings yet