Download as pdf or txt
You might also like
- Guide To Hazardous Paint Management - ASNZS 4361.2.2017 - Part 2 - Lead Paint in Residential, Public and Commercial BuildingsDocument10 pagesGuide To Hazardous Paint Management - ASNZS 4361.2.2017 - Part 2 - Lead Paint in Residential, Public and Commercial Buildingshitman13630% (1)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (3)
- Practical Insulin: A Handbook for Prescribing ProvidersFrom EverandPractical Insulin: A Handbook for Prescribing ProvidersRating: 5 out of 5 stars5/5 (2)
- Nursing Care PlanDocument3 pagesNursing Care Planjovanney100% (10)
- Alex Sander Case StudyDocument12 pagesAlex Sander Case StudyAditya Beri100% (1)
- Thera L15 PracticalDocument21 pagesThera L15 PracticalFatmaNo ratings yet
- Penggunaan Insulin Pada Diabetes Tipe 2Document47 pagesPenggunaan Insulin Pada Diabetes Tipe 2pebbyfebrianNo ratings yet
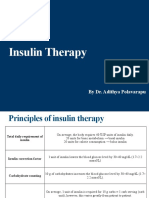
- Insulin Therapy: by Dr. Adithya PolavarapuDocument18 pagesInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNo ratings yet
- Insulin Treatment in DiabetesDocument86 pagesInsulin Treatment in DiabetesAhsan Rauf100% (1)
- 02 Tatalaksana Terapi Insulin - Prof Tri Murti AndayaniDocument39 pages02 Tatalaksana Terapi Insulin - Prof Tri Murti AndayaniEndang Wulan SariNo ratings yet
- Endocrine SystemDocument21 pagesEndocrine SystemMona MahfouzNo ratings yet
- Oral RevalidaDocument39 pagesOral Revalidajunathancortez123No ratings yet
- Insulin Initiation PPT - PPTX 2Document53 pagesInsulin Initiation PPT - PPTX 2Meno Ali100% (1)
- Lesson 15: Drugs For Diabetes: Introduction (ILO-1 - 2)Document38 pagesLesson 15: Drugs For Diabetes: Introduction (ILO-1 - 2)Ralp ManglicmotNo ratings yet
- Pharmacology Reading Materials On DMDocument19 pagesPharmacology Reading Materials On DMJames SoeNo ratings yet
- Management of Type 2 Diabetes:: DR - Bratasena.Mkedpd - SPPDDocument51 pagesManagement of Type 2 Diabetes:: DR - Bratasena.Mkedpd - SPPDAnnisa SyafeiNo ratings yet
- Childhood Diabetes 2016Document64 pagesChildhood Diabetes 2016Awatef AbushhiwaNo ratings yet
- Insulin Therapy in Type 1 DiabetesDocument11 pagesInsulin Therapy in Type 1 DiabetesrendraNo ratings yet
- Insulin GNTDocument41 pagesInsulin GNTV Narayan Rao TummalaNo ratings yet
- DM Presentation NewDocument44 pagesDM Presentation NewKipz JonsNo ratings yet
- Presented by DR Ashish Sharma Guided by DR Meena PatelDocument74 pagesPresented by DR Ashish Sharma Guided by DR Meena PatelAndrew Surya Putra SccNo ratings yet
- Diabetes in PregnancyDocument38 pagesDiabetes in Pregnancybdzq3i12No ratings yet
- Endocrinology ReviewDocument8 pagesEndocrinology ReviewAmna KhanNo ratings yet
- Diabetes Melitus Dan KomplikasinyaDocument60 pagesDiabetes Melitus Dan Komplikasinyahandiwijaya_85No ratings yet
- Antidiabetic Agents: Diabetes MellitusDocument7 pagesAntidiabetic Agents: Diabetes MellitusRatika SariNo ratings yet
- 60-2005 - Pregestational Diabetes MellitusDocument11 pages60-2005 - Pregestational Diabetes MellitusGrupo Atlas100% (1)
- Managing Diabetes - RaflaDocument38 pagesManaging Diabetes - Raflamsala76No ratings yet
- Diabetes Mellitus: Dr. Stanley Binagi Mmed Internal MedicineDocument60 pagesDiabetes Mellitus: Dr. Stanley Binagi Mmed Internal MedicineTeddy MauriceNo ratings yet
- DR - Rihab Pediatrics 02.pediatric DM Part TwoDocument7 pagesDR - Rihab Pediatrics 02.pediatric DM Part TwoMujtaba JawadNo ratings yet
- Dr. Dr. I Wayan Bikin Suryawan SpA (K) - Type II DM Whats New On ManagementDocument34 pagesDr. Dr. I Wayan Bikin Suryawan SpA (K) - Type II DM Whats New On ManagementajescoolNo ratings yet
- Meglitinide Works by Stimulating The Release of Insulin in The Presence of GlucoseDocument53 pagesMeglitinide Works by Stimulating The Release of Insulin in The Presence of GlucoseWil LesterNo ratings yet
- 5th WS-DM 02Document38 pages5th WS-DM 02Andy F MonroeNo ratings yet
- Diabetes MellitusDocument93 pagesDiabetes MellitusAllen Reyes SantosNo ratings yet
- Insulin Case Studies AACE 5-20-05Document56 pagesInsulin Case Studies AACE 5-20-05Leanne Shepherd100% (2)
- FO-Antidiabetic-27042020-Blok 7Document64 pagesFO-Antidiabetic-27042020-Blok 7Indah NurhalizaNo ratings yet
- Glycemic ManagementDocument39 pagesGlycemic ManagementZayar HmunNo ratings yet
- Endocrinology - Review NotesDocument9 pagesEndocrinology - Review NotesRoa Al-SajjanNo ratings yet
- LEC#37 Anti Diabetic Drugs (Insulin)Document20 pagesLEC#37 Anti Diabetic Drugs (Insulin)alihyderabro166No ratings yet
- DM Lab 2 - FinalDocument33 pagesDM Lab 2 - FinalMahamed Wefkey OmranNo ratings yet
- Insulin TherapyDocument10 pagesInsulin Therapymandloianand51No ratings yet
- Insulin and Antidiabetic Drugs: Prof - DR Asya RehmanDocument23 pagesInsulin and Antidiabetic Drugs: Prof - DR Asya RehmanGareth BaleNo ratings yet
- CASE Study Insulin InitiationDocument54 pagesCASE Study Insulin InitiationAshraf Shaaban MahfouzNo ratings yet
- Manejo de La DMGDocument5 pagesManejo de La DMGsandymejiaNo ratings yet
- Diabetes Mellitus: DR - Sumaia Z.H.Abuelbasher Mbbs.U N.Unversity - Mrcp. Uk Msc.C.Pharm - UmstDocument35 pagesDiabetes Mellitus: DR - Sumaia Z.H.Abuelbasher Mbbs.U N.Unversity - Mrcp. Uk Msc.C.Pharm - Umstsamar yousif mohamedNo ratings yet
- Antidiabetic Drugs. 12 May Modified 2016 of 2015 - 2017 11 17 MayDocument54 pagesAntidiabetic Drugs. 12 May Modified 2016 of 2015 - 2017 11 17 Mayblue sapphireNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Diabetes Mellitus Key PointsDocument6 pagesLewis: Medical-Surgical Nursing, 10 Edition: Diabetes Mellitus Key PointsDeo FactuarNo ratings yet
- EndokrinoDocument78 pagesEndokrinoJulian TaneNo ratings yet
- Jurnal DMDocument5 pagesJurnal DMratihparmadiniNo ratings yet
- Fit-Diploma 3-2-2024Document57 pagesFit-Diploma 3-2-2024light tweenNo ratings yet
- All Types of InsulinDocument18 pagesAll Types of Insulinali mohammedNo ratings yet
- Insulin Initiation and MonitoringDocument35 pagesInsulin Initiation and Monitoringeka prasepti darusmanNo ratings yet
- A Practical Guide To Insulin TherapyDocument42 pagesA Practical Guide To Insulin Therapyseun williams100% (2)
- T31 - Types of Diabetes and Diagnosis - PTPDocument6 pagesT31 - Types of Diabetes and Diagnosis - PTPangela adelantarNo ratings yet
- Diabetes Mellitus in Paediatric Age: Topics CoveredDocument13 pagesDiabetes Mellitus in Paediatric Age: Topics Coveredlotp12No ratings yet
- Diabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMDocument20 pagesDiabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMPriyanka Karnik100% (1)
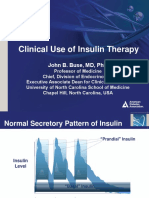
- Slide Clinical Use of Insulin Therapy (ADA)Document36 pagesSlide Clinical Use of Insulin Therapy (ADA)Dian SobaNo ratings yet
- Pharmacology Chapter 38Document7 pagesPharmacology Chapter 38languha NgatiNo ratings yet
- Lecture 2 Anti-Diabetic Therapy. DR HESHAM-1Document90 pagesLecture 2 Anti-Diabetic Therapy. DR HESHAM-1La romeNo ratings yet
- Antenatal Managemennt by DSKDocument14 pagesAntenatal Managemennt by DSKSanthosh Kumar DskNo ratings yet
- Pharmacology ResearchDocument20 pagesPharmacology ResearchaagalhazmiNo ratings yet
- Diabetes Mellitus: Dr. Beny Ghufron, SP - PD. SMF Penyakit Dalam Rsud DR Haryoto LumajangDocument70 pagesDiabetes Mellitus: Dr. Beny Ghufron, SP - PD. SMF Penyakit Dalam Rsud DR Haryoto LumajangDendian Berlia JelitaNo ratings yet
- EInsulin RegiemDocument18 pagesEInsulin RegiemzahrabokerNo ratings yet
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- SAB CHCAGE005 Provide Support To People Living With DementiaDocument114 pagesSAB CHCAGE005 Provide Support To People Living With DementiaAnonymous wWCGc6fzUX100% (3)
- Rift Valley Water Supply and Sanitation ProjectDocument59 pagesRift Valley Water Supply and Sanitation ProjectcherogonyaNo ratings yet
- CPE 103 ScriptDocument4 pagesCPE 103 ScriptExchan ヅNo ratings yet
- Artikel 3Document23 pagesArtikel 3Hadian UwuoNo ratings yet
- PrintDocument2 pagesPrintDeepak MoreNo ratings yet
- Phases of The Nursing Research Process: Module DescriptionDocument15 pagesPhases of The Nursing Research Process: Module DescriptionSamantha Janelah PagayNo ratings yet
- ReportViewer 1Document4 pagesReportViewer 1Shehriyar KhanNo ratings yet
- Literature Review PyramidDocument6 pagesLiterature Review Pyramidaflshvifm100% (1)
- Procedure Line Release After MaintenanceDocument2 pagesProcedure Line Release After MaintenanceWilson Atehortua100% (1)
- Communication Skills For Children With Severe Learning DifficultiesDocument10 pagesCommunication Skills For Children With Severe Learning DifficultiesMay Grace E. BalbinNo ratings yet
- Football Fanaticism: An Integrated Physiology Case Study: PreludeDocument2 pagesFootball Fanaticism: An Integrated Physiology Case Study: PreludeAbbNo ratings yet
- Dental Surgeon ResumeDocument4 pagesDental Surgeon Resumeafmsheushbqoac100% (1)
- Conservative Technique For Restoration of Anterior Teeth: Clinical Case ReportDocument6 pagesConservative Technique For Restoration of Anterior Teeth: Clinical Case ReportNonoNo ratings yet
- Medical Laboratory Technicians PDFDocument179 pagesMedical Laboratory Technicians PDFMicky Rod RazafNo ratings yet
- Emotional Intelligence What Is Emotional Intelligence ?Document7 pagesEmotional Intelligence What Is Emotional Intelligence ?shanNo ratings yet
- Meditative StateDocument227 pagesMeditative StateJeyashankar Ramakrishnan100% (1)
- Zyzz BibleDocument66 pagesZyzz BibleJean Santos0% (1)
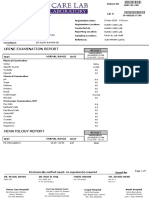
- Urine Examination Report: Test Normal Range UnitDocument1 pageUrine Examination Report: Test Normal Range Unitمرتجز حیدرNo ratings yet
- Cassell v. Snyders (N.D. Ill. 2020)Document18 pagesCassell v. Snyders (N.D. Ill. 2020)Scott Ronald Medgar EalyNo ratings yet
- Vig Soft 1Document10 pagesVig Soft 120L237PRAJIT ECEBNo ratings yet
- Jurnal KBDocument7 pagesJurnal KBAnahNo ratings yet
- Medical Surgical Nursing Nclex Questions Onco1Document12 pagesMedical Surgical Nursing Nclex Questions Onco1dee_day_8100% (2)
- RP 6 Month Hypertrophy App-Fat LossDocument10 pagesRP 6 Month Hypertrophy App-Fat LossjonasNo ratings yet
- Airway DevicesDocument58 pagesAirway DevicesArmaanjeet SinghNo ratings yet
- Nordlund-DAmato2018 ReferenceWorkEntry NeuroleadershipDocument4 pagesNordlund-DAmato2018 ReferenceWorkEntry NeuroleadershipLidya GergessNo ratings yet
- Is Mesh Always Necessary in Every Small UmbilicalDocument8 pagesIs Mesh Always Necessary in Every Small UmbilicalLeonardo RibeiroNo ratings yet
- B 22392798Document110 pagesB 22392798mapitit507No ratings yet