
Haemoglobin D Distribution in Ulcers For Assessment Healing
Haemoglobin D Distribution in Ulcers For Assessment Healing
You might also like
- ETE 424 Lab02 HandoffDocument4 pagesETE 424 Lab02 HandoffIfthakharul Alam ShuvoNo ratings yet
- Non-Invasive Diagnostic Techniques in DermatologyDocument3 pagesNon-Invasive Diagnostic Techniques in DermatologyVinh ThếNo ratings yet
- 2009 CutaneousScarringAClinicalReview PDFDocument7 pages2009 CutaneousScarringAClinicalReview PDFJ Roberto Meza OntiverosNo ratings yet
- Fine-Grained Diabetic Wound Depth and Granulation Tissue Amount Assessment Using Bilinear Convolutional Neural NetworkDocument12 pagesFine-Grained Diabetic Wound Depth and Granulation Tissue Amount Assessment Using Bilinear Convolutional Neural NetworkKaLebNo ratings yet
- Skin Lesion Classification of Dermoscopic Images Using Machine Learning and Convolutional Neural NetworkDocument11 pagesSkin Lesion Classification of Dermoscopic Images Using Machine Learning and Convolutional Neural NetworkAnish kumar DasNo ratings yet
- Paper No 7Document4 pagesPaper No 7sahil jadhavNo ratings yet
- Boundary Tracing Algorithm For Automatic Skin Lesion Detection in Macroscopic ImagesDocument9 pagesBoundary Tracing Algorithm For Automatic Skin Lesion Detection in Macroscopic ImagesKranthirekha ChennaboinaNo ratings yet
- Skin Lesion Using Support Vector Machine-MainDocument6 pagesSkin Lesion Using Support Vector Machine-MainBT20CS023 [Nishu]No ratings yet
- DeepSkin A Deep Learning Approach For Skin Cancer ClassificationDocument10 pagesDeepSkin A Deep Learning Approach For Skin Cancer ClassificationShivam MaheshNo ratings yet
- Karim 2020Document15 pagesKarim 2020Astri SuyataNo ratings yet
- Disease Detection From An Image of Skin LesionA Survey ReportDocument3 pagesDisease Detection From An Image of Skin LesionA Survey ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Superficial, Partial, and Full Thickness, Can Also Be Used To Describe Depth inDocument3 pagesSuperficial, Partial, and Full Thickness, Can Also Be Used To Describe Depth inMerly Ann MaltoNo ratings yet
- Collagen Regeneration Template in The Management of Full-Thickness Wounds - A Prospective Multicentre Study. Alet2019Document8 pagesCollagen Regeneration Template in The Management of Full-Thickness Wounds - A Prospective Multicentre Study. Alet2019Li A VélezNo ratings yet
- Research Article: Skin Disease Recognition Method Based On Image Color and Texture FeaturesDocument11 pagesResearch Article: Skin Disease Recognition Method Based On Image Color and Texture FeaturesAYUSH KUMARNo ratings yet
- Skin Disease Recognition Using Texture AnalysisDocument5 pagesSkin Disease Recognition Using Texture Analysissahil jadhavNo ratings yet
- Dermal SubstitutesDocument9 pagesDermal SubstitutesEsq. Nelson OduorNo ratings yet
- Identification & Enhancement of Different Skin Lesion Images by Segmentation TechniquesDocument6 pagesIdentification & Enhancement of Different Skin Lesion Images by Segmentation TechniquesECS TechnologyNo ratings yet
- Skin Lesion Detection Using CNNDocument7 pagesSkin Lesion Detection Using CNNInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Detection of Abnormal Tissue Growth in MR Imaging Using Biogeography Based OptimizationDocument7 pagesDetection of Abnormal Tissue Growth in MR Imaging Using Biogeography Based OptimizationInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Successful Treatment of Facial Atrophic Acne Scars by Fractional Radiofrequency Microneedle in Vietnamese PatientsDocument3 pagesSuccessful Treatment of Facial Atrophic Acne Scars by Fractional Radiofrequency Microneedle in Vietnamese PatientsArturo OteroNo ratings yet
- 2012 JBO v18 n6 p061213 LiewDocument10 pages2012 JBO v18 n6 p061213 LiewYih Miin LiewNo ratings yet
- An Efficient Gray-Level Co-Occurrence Matrix (GLCM) BasedDocument4 pagesAn Efficient Gray-Level Co-Occurrence Matrix (GLCM) BasedS M RizviNo ratings yet
- Identification and Classification of Skin Cancer Using A GUI and A Deep Neural NetworkDocument14 pagesIdentification and Classification of Skin Cancer Using A GUI and A Deep Neural NetworkIJRASETPublicationsNo ratings yet
- (IJETA-V5I2P5) :mr. Pratik Badhe, Mr. Pravin Pawar, Prof. Bahubali Shiragapur, Prof Nishikant SurwadeDocument4 pages(IJETA-V5I2P5) :mr. Pratik Badhe, Mr. Pravin Pawar, Prof. Bahubali Shiragapur, Prof Nishikant SurwadeIJETA - EighthSenseGroupNo ratings yet
- UntitledDocument29 pagesUntitledITB433 Priti RathodNo ratings yet
- An Hybrid Approach For Identification of Breast Cancer Using Mammogram ImagesDocument4 pagesAn Hybrid Approach For Identification of Breast Cancer Using Mammogram ImagesEditor IJRITCCNo ratings yet
- A Segmentation Process To Isolate Various Cytological Components From Follicular Histology Based On Texture HeterogeneityDocument9 pagesA Segmentation Process To Isolate Various Cytological Components From Follicular Histology Based On Texture HeterogeneityIJRASETPublicationsNo ratings yet
- SRT 29 E13272Document12 pagesSRT 29 E13272Tânia QueirósNo ratings yet
- Revolutionizing Skin Cancer Detection: A Comprehensive Review of Deep Learning MethodsDocument6 pagesRevolutionizing Skin Cancer Detection: A Comprehensive Review of Deep Learning MethodsH.M. RaiNo ratings yet
- 551Document7 pages551dilkulNo ratings yet
- SosotherDocument8 pagesSosotherMarsella SetiawanNo ratings yet
- Paper 06Document13 pagesPaper 06nayera279No ratings yet
- Deep Ensemble Learning For Skin Lesions Classification With Convolutional Neural NetworkDocument8 pagesDeep Ensemble Learning For Skin Lesions Classification With Convolutional Neural NetworkIAES IJAINo ratings yet
- Literature Survey On Skin Lesion ClassificationDocument7 pagesLiterature Survey On Skin Lesion ClassificationIJRASETPublicationsNo ratings yet
- 5 A Machine Learning Approach For Skin Disease Detection and 2022 HealthcareDocument15 pages5 A Machine Learning Approach For Skin Disease Detection and 2022 HealthcarePaul Awinpang GodswayNo ratings yet
- C3 Skin Lesion Based Melanoma Disease Detection Approach For Efficient Classification of Medical ImagesDocument16 pagesC3 Skin Lesion Based Melanoma Disease Detection Approach For Efficient Classification of Medical ImagesMuthu KNo ratings yet
- Skin Lesion Classification Based On ConvolutionalDocument6 pagesSkin Lesion Classification Based On ConvolutionalAnchal SharmaNo ratings yet
- Identification of Skin Disease Using Machine LearningDocument15 pagesIdentification of Skin Disease Using Machine LearningSURYA PRAKASH K ITNo ratings yet
- Twa Made EasyDocument6 pagesTwa Made EasyDottor LphoneNo ratings yet
- Ijigsp V7 N6 6 PDFDocument7 pagesIjigsp V7 N6 6 PDFShantala GiraddiNo ratings yet
- A Survey of Feature Extraction in Dermoscopy Image Analysis of Skin CancerDocument14 pagesA Survey of Feature Extraction in Dermoscopy Image Analysis of Skin CancerSUMIT GANGWARNo ratings yet
- Deep Learning Based Skin Cancer Classifier Using MobileNetDocument7 pagesDeep Learning Based Skin Cancer Classifier Using MobileNetIJRASETPublicationsNo ratings yet
- Ajd 12390Document5 pagesAjd 12390Ratih Anindita Rahajeng RipyonoNo ratings yet
- Efficacy of Mesotherapy in Facial Rejuvenation A Histological and Immunohistochemical Evaluation - El-Domyati, 2012Document12 pagesEfficacy of Mesotherapy in Facial Rejuvenation A Histological and Immunohistochemical Evaluation - El-Domyati, 2012Rafael Autran Cavalcante AraújoNo ratings yet
- Fixation of Split Skin Graft Using Cyanoacrylate Tissue Adhesive Versus Skin Stapling: A Comparative StudyDocument4 pagesFixation of Split Skin Graft Using Cyanoacrylate Tissue Adhesive Versus Skin Stapling: A Comparative StudysindujasaravananNo ratings yet
- 2014 JBO v19 n2 p021111 GongDocument11 pages2014 JBO v19 n2 p021111 GongYih Miin LiewNo ratings yet
- Role of Proliferative Markers in Breast LesionsDocument6 pagesRole of Proliferative Markers in Breast LesionsAchyut KanungoNo ratings yet
- Diagnostics 13 03147 v2Document40 pagesDiagnostics 13 03147 v2SURYA PRAKASH K ITNo ratings yet
- AnnMaxillofacSurg62204-7504388 020504Document6 pagesAnnMaxillofacSurg62204-7504388 020504mascoNo ratings yet
- A Glioma Segmentation Method Using Cotraining and Superpixel-Based Spatial and Clinical ConstraintsDocument11 pagesA Glioma Segmentation Method Using Cotraining and Superpixel-Based Spatial and Clinical ConstraintsjaspayoNo ratings yet
- HealthCom2010 v5Document6 pagesHealthCom2010 v5davorNo ratings yet
- Jurnal Mengenai Pewarnaan KolagenDocument6 pagesJurnal Mengenai Pewarnaan KolagenrahmaaaaaNo ratings yet
- Implementation of Digital Signal ProcessingDocument3 pagesImplementation of Digital Signal Processingडाँ सूर्यदेव चौधरीNo ratings yet
- Detection and Classification of Acne Lesions in Acne Patients: A Mobile ApplicationDocument6 pagesDetection and Classification of Acne Lesions in Acne Patients: A Mobile ApplicationEdward RenzoNo ratings yet
- EIT2016 AcneDetectionandClassification PDFDocument6 pagesEIT2016 AcneDetectionandClassification PDFEdward RenzoNo ratings yet
- Classification of The Clinical Images ForDocument10 pagesClassification of The Clinical Images ForHaleema ahsanNo ratings yet
- Radiomics in Gliomas: Clinical Implications of Computational Modeling and Fractal-Based AnalysisDocument20 pagesRadiomics in Gliomas: Clinical Implications of Computational Modeling and Fractal-Based AnalysisAkansha SinghNo ratings yet
- Novel Methods To Detect Melanoma by Dermoscopy Images: August 2021Document12 pagesNovel Methods To Detect Melanoma by Dermoscopy Images: August 2021Md. Sazzad Mia 191-15-2503No ratings yet
- Melanoma Disease Detection and Classification Using Deep LearningDocument11 pagesMelanoma Disease Detection and Classification Using Deep LearningIJRASETPublicationsNo ratings yet
- A Comparative Study of Collagen Granule Dressing Versus Conventional Dressing in Deep WoundsDocument6 pagesA Comparative Study of Collagen Granule Dressing Versus Conventional Dressing in Deep WoundsInternational Organization of Scientific Research (IOSR)No ratings yet
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- The Difference of Stem Cell ProductDocument12 pagesThe Difference of Stem Cell ProductIsmail Tidak Ada KepanjanganNo ratings yet
- Dok Baru 2020-02-22 07.09.19Document11 pagesDok Baru 2020-02-22 07.09.19Ismail Tidak Ada KepanjanganNo ratings yet
- Dok Baru 2020-02-22 07.48.28Document3 pagesDok Baru 2020-02-22 07.48.28Ismail Tidak Ada KepanjanganNo ratings yet
- Dok Baru 2020-02-22 07.52.37Document11 pagesDok Baru 2020-02-22 07.52.37Ismail Tidak Ada KepanjanganNo ratings yet
- Dok Baru 2020-02-22 07.52.16Document11 pagesDok Baru 2020-02-22 07.52.16Ismail Tidak Ada KepanjanganNo ratings yet
- Dok Baru 2020-02-22 07.51.50Document11 pagesDok Baru 2020-02-22 07.51.50Ismail Tidak Ada KepanjanganNo ratings yet
- Imaging The Patient With Sacroiliac PainDocument11 pagesImaging The Patient With Sacroiliac PainIsmail Tidak Ada KepanjanganNo ratings yet
- Daftar Pustaka 15 - 161Document1 pageDaftar Pustaka 15 - 161Ismail Tidak Ada KepanjanganNo ratings yet
- Outcomes After Arthroscopic Bankart Repair in Adolescent Athletes Participating in Collision and Contact SportsDocument8 pagesOutcomes After Arthroscopic Bankart Repair in Adolescent Athletes Participating in Collision and Contact SportsIsmail Tidak Ada KepanjanganNo ratings yet
- Arthroscopic Bankart Repair For The Management of Anterior Shoulder Instability Indications and OutcomesDocument10 pagesArthroscopic Bankart Repair For The Management of Anterior Shoulder Instability Indications and OutcomesIsmail Tidak Ada KepanjanganNo ratings yet
- Research Process - StepsDocument29 pagesResearch Process - StepsShaanu SaxenaNo ratings yet
- Isomeros Del FenalenoDocument5 pagesIsomeros Del Fenalenocharalito123No ratings yet
- Linear Algebra Done WrongDocument231 pagesLinear Algebra Done WrongS NandaNo ratings yet
- Statistics - Chap1 & 2 - Inroduction Assignment 28 AprilDocument2 pagesStatistics - Chap1 & 2 - Inroduction Assignment 28 AprilnathanNo ratings yet
- Arduino Tutorial OV7670 Camera ModuleDocument18 pagesArduino Tutorial OV7670 Camera ModuleKabilesh CmNo ratings yet
- SAP HANA Developer Guide For SAP HANA Studio enDocument892 pagesSAP HANA Developer Guide For SAP HANA Studio enWagBezerraNo ratings yet
- 2G Drive TestDocument73 pages2G Drive TestAhmad Ramadan0% (1)
- Mil DTL 7601Document12 pagesMil DTL 7601Michaël REYNAULTNo ratings yet
- HHDocument48 pagesHHbipin012No ratings yet
- Updated NewDocument73 pagesUpdated NewAbhishek GaurNo ratings yet
- Sanyo ICs STKs PDFDocument117 pagesSanyo ICs STKs PDFFreddy Monge BarbaranNo ratings yet
- Technical Information Data Communication With Victron Energy Products - ENDocument13 pagesTechnical Information Data Communication With Victron Energy Products - ENMonitoreo PetasolareNo ratings yet
- CapmDocument51 pagesCapmlathachilNo ratings yet
- British Standard: A Single Copy of This British Standard Is Licensed ToDocument30 pagesBritish Standard: A Single Copy of This British Standard Is Licensed Todasdasdsad432No ratings yet
- Msunit 2 GraspsDocument6 pagesMsunit 2 Graspsapi-338845804No ratings yet
- Chapter 2 AisDocument27 pagesChapter 2 AisPhrexilyn PajarilloNo ratings yet
- Ecommender Ystem: Resented By: Nisrine HIHOUD Yassin AKHROUF Chaymae BOUJIM Mohamed Amine EL ALAOUIDocument20 pagesEcommender Ystem: Resented By: Nisrine HIHOUD Yassin AKHROUF Chaymae BOUJIM Mohamed Amine EL ALAOUIAmine El AlaouiNo ratings yet
- K30a Datasheet PDFDocument1 pageK30a Datasheet PDFIvan CVNo ratings yet
- 26G Radar Level MeterDocument14 pages26G Radar Level Meterilopera1971No ratings yet
- 2023 TJPhO v1Document11 pages2023 TJPhO v1Phúc NguyễnNo ratings yet
- Analog Devices - MT-016Document6 pagesAnalog Devices - MT-016ModyKing99No ratings yet
- Ir2112 (S) & (PBF) : High and Low Side DriverDocument17 pagesIr2112 (S) & (PBF) : High and Low Side DriverMugahed DammagNo ratings yet
- Pipe Bend RadiusDocument8 pagesPipe Bend RadiusAdagharaNo ratings yet
- BOQ - 400/220/33kV GIS Substation For Panchshil Data Center at Airoli, Navi MumbaiDocument13 pagesBOQ - 400/220/33kV GIS Substation For Panchshil Data Center at Airoli, Navi MumbaiPrasad Pawar - ERO Power100% (1)
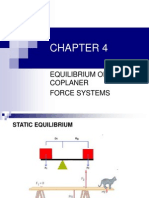
- CHAPTER 4 Equilibrium of Coplanar Force SystemsDocument50 pagesCHAPTER 4 Equilibrium of Coplanar Force SystemsDavid Murphy80% (10)
- Tutorial Fpga Spartan-3eDocument53 pagesTutorial Fpga Spartan-3eCarlos Muñoz BacaNo ratings yet
- Soild VoidDocument5 pagesSoild VoidTanushree SalujaNo ratings yet
- P281 (En) SYS600 94 Operation 14042015Document191 pagesP281 (En) SYS600 94 Operation 14042015Victor SalazarNo ratings yet
- VHF Uhf Duoband Ant eDocument2 pagesVHF Uhf Duoband Ant eNol SatuNo ratings yet

































































































Download as pdf or txt
You might also like
- ETE 424 Lab02 HandoffDocument4 pagesETE 424 Lab02 HandoffIfthakharul Alam ShuvoNo ratings yet
- Non-Invasive Diagnostic Techniques in DermatologyDocument3 pagesNon-Invasive Diagnostic Techniques in DermatologyVinh ThếNo ratings yet
- 2009 CutaneousScarringAClinicalReview PDFDocument7 pages2009 CutaneousScarringAClinicalReview PDFJ Roberto Meza OntiverosNo ratings yet
- Fine-Grained Diabetic Wound Depth and Granulation Tissue Amount Assessment Using Bilinear Convolutional Neural NetworkDocument12 pagesFine-Grained Diabetic Wound Depth and Granulation Tissue Amount Assessment Using Bilinear Convolutional Neural NetworkKaLebNo ratings yet
- Skin Lesion Classification of Dermoscopic Images Using Machine Learning and Convolutional Neural NetworkDocument11 pagesSkin Lesion Classification of Dermoscopic Images Using Machine Learning and Convolutional Neural NetworkAnish kumar DasNo ratings yet
- Paper No 7Document4 pagesPaper No 7sahil jadhavNo ratings yet
- Boundary Tracing Algorithm For Automatic Skin Lesion Detection in Macroscopic ImagesDocument9 pagesBoundary Tracing Algorithm For Automatic Skin Lesion Detection in Macroscopic ImagesKranthirekha ChennaboinaNo ratings yet
- Skin Lesion Using Support Vector Machine-MainDocument6 pagesSkin Lesion Using Support Vector Machine-MainBT20CS023 [Nishu]No ratings yet
- DeepSkin A Deep Learning Approach For Skin Cancer ClassificationDocument10 pagesDeepSkin A Deep Learning Approach For Skin Cancer ClassificationShivam MaheshNo ratings yet
- Karim 2020Document15 pagesKarim 2020Astri SuyataNo ratings yet
- Disease Detection From An Image of Skin LesionA Survey ReportDocument3 pagesDisease Detection From An Image of Skin LesionA Survey ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Superficial, Partial, and Full Thickness, Can Also Be Used To Describe Depth inDocument3 pagesSuperficial, Partial, and Full Thickness, Can Also Be Used To Describe Depth inMerly Ann MaltoNo ratings yet
- Collagen Regeneration Template in The Management of Full-Thickness Wounds - A Prospective Multicentre Study. Alet2019Document8 pagesCollagen Regeneration Template in The Management of Full-Thickness Wounds - A Prospective Multicentre Study. Alet2019Li A VélezNo ratings yet
- Research Article: Skin Disease Recognition Method Based On Image Color and Texture FeaturesDocument11 pagesResearch Article: Skin Disease Recognition Method Based On Image Color and Texture FeaturesAYUSH KUMARNo ratings yet
- Skin Disease Recognition Using Texture AnalysisDocument5 pagesSkin Disease Recognition Using Texture Analysissahil jadhavNo ratings yet
- Dermal SubstitutesDocument9 pagesDermal SubstitutesEsq. Nelson OduorNo ratings yet
- Identification & Enhancement of Different Skin Lesion Images by Segmentation TechniquesDocument6 pagesIdentification & Enhancement of Different Skin Lesion Images by Segmentation TechniquesECS TechnologyNo ratings yet
- Skin Lesion Detection Using CNNDocument7 pagesSkin Lesion Detection Using CNNInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Detection of Abnormal Tissue Growth in MR Imaging Using Biogeography Based OptimizationDocument7 pagesDetection of Abnormal Tissue Growth in MR Imaging Using Biogeography Based OptimizationInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Successful Treatment of Facial Atrophic Acne Scars by Fractional Radiofrequency Microneedle in Vietnamese PatientsDocument3 pagesSuccessful Treatment of Facial Atrophic Acne Scars by Fractional Radiofrequency Microneedle in Vietnamese PatientsArturo OteroNo ratings yet
- 2012 JBO v18 n6 p061213 LiewDocument10 pages2012 JBO v18 n6 p061213 LiewYih Miin LiewNo ratings yet
- An Efficient Gray-Level Co-Occurrence Matrix (GLCM) BasedDocument4 pagesAn Efficient Gray-Level Co-Occurrence Matrix (GLCM) BasedS M RizviNo ratings yet
- Identification and Classification of Skin Cancer Using A GUI and A Deep Neural NetworkDocument14 pagesIdentification and Classification of Skin Cancer Using A GUI and A Deep Neural NetworkIJRASETPublicationsNo ratings yet
- (IJETA-V5I2P5) :mr. Pratik Badhe, Mr. Pravin Pawar, Prof. Bahubali Shiragapur, Prof Nishikant SurwadeDocument4 pages(IJETA-V5I2P5) :mr. Pratik Badhe, Mr. Pravin Pawar, Prof. Bahubali Shiragapur, Prof Nishikant SurwadeIJETA - EighthSenseGroupNo ratings yet
- UntitledDocument29 pagesUntitledITB433 Priti RathodNo ratings yet
- An Hybrid Approach For Identification of Breast Cancer Using Mammogram ImagesDocument4 pagesAn Hybrid Approach For Identification of Breast Cancer Using Mammogram ImagesEditor IJRITCCNo ratings yet
- A Segmentation Process To Isolate Various Cytological Components From Follicular Histology Based On Texture HeterogeneityDocument9 pagesA Segmentation Process To Isolate Various Cytological Components From Follicular Histology Based On Texture HeterogeneityIJRASETPublicationsNo ratings yet
- SRT 29 E13272Document12 pagesSRT 29 E13272Tânia QueirósNo ratings yet
- Revolutionizing Skin Cancer Detection: A Comprehensive Review of Deep Learning MethodsDocument6 pagesRevolutionizing Skin Cancer Detection: A Comprehensive Review of Deep Learning MethodsH.M. RaiNo ratings yet
- 551Document7 pages551dilkulNo ratings yet
- SosotherDocument8 pagesSosotherMarsella SetiawanNo ratings yet
- Paper 06Document13 pagesPaper 06nayera279No ratings yet
- Deep Ensemble Learning For Skin Lesions Classification With Convolutional Neural NetworkDocument8 pagesDeep Ensemble Learning For Skin Lesions Classification With Convolutional Neural NetworkIAES IJAINo ratings yet
- Literature Survey On Skin Lesion ClassificationDocument7 pagesLiterature Survey On Skin Lesion ClassificationIJRASETPublicationsNo ratings yet
- 5 A Machine Learning Approach For Skin Disease Detection and 2022 HealthcareDocument15 pages5 A Machine Learning Approach For Skin Disease Detection and 2022 HealthcarePaul Awinpang GodswayNo ratings yet
- C3 Skin Lesion Based Melanoma Disease Detection Approach For Efficient Classification of Medical ImagesDocument16 pagesC3 Skin Lesion Based Melanoma Disease Detection Approach For Efficient Classification of Medical ImagesMuthu KNo ratings yet
- Skin Lesion Classification Based On ConvolutionalDocument6 pagesSkin Lesion Classification Based On ConvolutionalAnchal SharmaNo ratings yet
- Identification of Skin Disease Using Machine LearningDocument15 pagesIdentification of Skin Disease Using Machine LearningSURYA PRAKASH K ITNo ratings yet
- Twa Made EasyDocument6 pagesTwa Made EasyDottor LphoneNo ratings yet
- Ijigsp V7 N6 6 PDFDocument7 pagesIjigsp V7 N6 6 PDFShantala GiraddiNo ratings yet
- A Survey of Feature Extraction in Dermoscopy Image Analysis of Skin CancerDocument14 pagesA Survey of Feature Extraction in Dermoscopy Image Analysis of Skin CancerSUMIT GANGWARNo ratings yet
- Deep Learning Based Skin Cancer Classifier Using MobileNetDocument7 pagesDeep Learning Based Skin Cancer Classifier Using MobileNetIJRASETPublicationsNo ratings yet
- Ajd 12390Document5 pagesAjd 12390Ratih Anindita Rahajeng RipyonoNo ratings yet
- Efficacy of Mesotherapy in Facial Rejuvenation A Histological and Immunohistochemical Evaluation - El-Domyati, 2012Document12 pagesEfficacy of Mesotherapy in Facial Rejuvenation A Histological and Immunohistochemical Evaluation - El-Domyati, 2012Rafael Autran Cavalcante AraújoNo ratings yet
- Fixation of Split Skin Graft Using Cyanoacrylate Tissue Adhesive Versus Skin Stapling: A Comparative StudyDocument4 pagesFixation of Split Skin Graft Using Cyanoacrylate Tissue Adhesive Versus Skin Stapling: A Comparative StudysindujasaravananNo ratings yet
- 2014 JBO v19 n2 p021111 GongDocument11 pages2014 JBO v19 n2 p021111 GongYih Miin LiewNo ratings yet
- Role of Proliferative Markers in Breast LesionsDocument6 pagesRole of Proliferative Markers in Breast LesionsAchyut KanungoNo ratings yet
- Diagnostics 13 03147 v2Document40 pagesDiagnostics 13 03147 v2SURYA PRAKASH K ITNo ratings yet
- AnnMaxillofacSurg62204-7504388 020504Document6 pagesAnnMaxillofacSurg62204-7504388 020504mascoNo ratings yet
- A Glioma Segmentation Method Using Cotraining and Superpixel-Based Spatial and Clinical ConstraintsDocument11 pagesA Glioma Segmentation Method Using Cotraining and Superpixel-Based Spatial and Clinical ConstraintsjaspayoNo ratings yet
- HealthCom2010 v5Document6 pagesHealthCom2010 v5davorNo ratings yet
- Jurnal Mengenai Pewarnaan KolagenDocument6 pagesJurnal Mengenai Pewarnaan KolagenrahmaaaaaNo ratings yet
- Implementation of Digital Signal ProcessingDocument3 pagesImplementation of Digital Signal Processingडाँ सूर्यदेव चौधरीNo ratings yet
- Detection and Classification of Acne Lesions in Acne Patients: A Mobile ApplicationDocument6 pagesDetection and Classification of Acne Lesions in Acne Patients: A Mobile ApplicationEdward RenzoNo ratings yet
- EIT2016 AcneDetectionandClassification PDFDocument6 pagesEIT2016 AcneDetectionandClassification PDFEdward RenzoNo ratings yet
- Classification of The Clinical Images ForDocument10 pagesClassification of The Clinical Images ForHaleema ahsanNo ratings yet
- Radiomics in Gliomas: Clinical Implications of Computational Modeling and Fractal-Based AnalysisDocument20 pagesRadiomics in Gliomas: Clinical Implications of Computational Modeling and Fractal-Based AnalysisAkansha SinghNo ratings yet
- Novel Methods To Detect Melanoma by Dermoscopy Images: August 2021Document12 pagesNovel Methods To Detect Melanoma by Dermoscopy Images: August 2021Md. Sazzad Mia 191-15-2503No ratings yet
- Melanoma Disease Detection and Classification Using Deep LearningDocument11 pagesMelanoma Disease Detection and Classification Using Deep LearningIJRASETPublicationsNo ratings yet
- A Comparative Study of Collagen Granule Dressing Versus Conventional Dressing in Deep WoundsDocument6 pagesA Comparative Study of Collagen Granule Dressing Versus Conventional Dressing in Deep WoundsInternational Organization of Scientific Research (IOSR)No ratings yet
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- The Difference of Stem Cell ProductDocument12 pagesThe Difference of Stem Cell ProductIsmail Tidak Ada KepanjanganNo ratings yet
- Dok Baru 2020-02-22 07.09.19Document11 pagesDok Baru 2020-02-22 07.09.19Ismail Tidak Ada KepanjanganNo ratings yet
- Dok Baru 2020-02-22 07.48.28Document3 pagesDok Baru 2020-02-22 07.48.28Ismail Tidak Ada KepanjanganNo ratings yet
- Dok Baru 2020-02-22 07.52.37Document11 pagesDok Baru 2020-02-22 07.52.37Ismail Tidak Ada KepanjanganNo ratings yet
- Dok Baru 2020-02-22 07.52.16Document11 pagesDok Baru 2020-02-22 07.52.16Ismail Tidak Ada KepanjanganNo ratings yet
- Dok Baru 2020-02-22 07.51.50Document11 pagesDok Baru 2020-02-22 07.51.50Ismail Tidak Ada KepanjanganNo ratings yet
- Imaging The Patient With Sacroiliac PainDocument11 pagesImaging The Patient With Sacroiliac PainIsmail Tidak Ada KepanjanganNo ratings yet
- Daftar Pustaka 15 - 161Document1 pageDaftar Pustaka 15 - 161Ismail Tidak Ada KepanjanganNo ratings yet
- Outcomes After Arthroscopic Bankart Repair in Adolescent Athletes Participating in Collision and Contact SportsDocument8 pagesOutcomes After Arthroscopic Bankart Repair in Adolescent Athletes Participating in Collision and Contact SportsIsmail Tidak Ada KepanjanganNo ratings yet
- Arthroscopic Bankart Repair For The Management of Anterior Shoulder Instability Indications and OutcomesDocument10 pagesArthroscopic Bankart Repair For The Management of Anterior Shoulder Instability Indications and OutcomesIsmail Tidak Ada KepanjanganNo ratings yet
- Research Process - StepsDocument29 pagesResearch Process - StepsShaanu SaxenaNo ratings yet
- Isomeros Del FenalenoDocument5 pagesIsomeros Del Fenalenocharalito123No ratings yet
- Linear Algebra Done WrongDocument231 pagesLinear Algebra Done WrongS NandaNo ratings yet
- Statistics - Chap1 & 2 - Inroduction Assignment 28 AprilDocument2 pagesStatistics - Chap1 & 2 - Inroduction Assignment 28 AprilnathanNo ratings yet
- Arduino Tutorial OV7670 Camera ModuleDocument18 pagesArduino Tutorial OV7670 Camera ModuleKabilesh CmNo ratings yet
- SAP HANA Developer Guide For SAP HANA Studio enDocument892 pagesSAP HANA Developer Guide For SAP HANA Studio enWagBezerraNo ratings yet
- 2G Drive TestDocument73 pages2G Drive TestAhmad Ramadan0% (1)
- Mil DTL 7601Document12 pagesMil DTL 7601Michaël REYNAULTNo ratings yet
- HHDocument48 pagesHHbipin012No ratings yet
- Updated NewDocument73 pagesUpdated NewAbhishek GaurNo ratings yet
- Sanyo ICs STKs PDFDocument117 pagesSanyo ICs STKs PDFFreddy Monge BarbaranNo ratings yet
- Technical Information Data Communication With Victron Energy Products - ENDocument13 pagesTechnical Information Data Communication With Victron Energy Products - ENMonitoreo PetasolareNo ratings yet
- CapmDocument51 pagesCapmlathachilNo ratings yet
- British Standard: A Single Copy of This British Standard Is Licensed ToDocument30 pagesBritish Standard: A Single Copy of This British Standard Is Licensed Todasdasdsad432No ratings yet
- Msunit 2 GraspsDocument6 pagesMsunit 2 Graspsapi-338845804No ratings yet
- Chapter 2 AisDocument27 pagesChapter 2 AisPhrexilyn PajarilloNo ratings yet
- Ecommender Ystem: Resented By: Nisrine HIHOUD Yassin AKHROUF Chaymae BOUJIM Mohamed Amine EL ALAOUIDocument20 pagesEcommender Ystem: Resented By: Nisrine HIHOUD Yassin AKHROUF Chaymae BOUJIM Mohamed Amine EL ALAOUIAmine El AlaouiNo ratings yet
- K30a Datasheet PDFDocument1 pageK30a Datasheet PDFIvan CVNo ratings yet
- 26G Radar Level MeterDocument14 pages26G Radar Level Meterilopera1971No ratings yet
- 2023 TJPhO v1Document11 pages2023 TJPhO v1Phúc NguyễnNo ratings yet
- Analog Devices - MT-016Document6 pagesAnalog Devices - MT-016ModyKing99No ratings yet
- Ir2112 (S) & (PBF) : High and Low Side DriverDocument17 pagesIr2112 (S) & (PBF) : High and Low Side DriverMugahed DammagNo ratings yet
- Pipe Bend RadiusDocument8 pagesPipe Bend RadiusAdagharaNo ratings yet
- BOQ - 400/220/33kV GIS Substation For Panchshil Data Center at Airoli, Navi MumbaiDocument13 pagesBOQ - 400/220/33kV GIS Substation For Panchshil Data Center at Airoli, Navi MumbaiPrasad Pawar - ERO Power100% (1)
- CHAPTER 4 Equilibrium of Coplanar Force SystemsDocument50 pagesCHAPTER 4 Equilibrium of Coplanar Force SystemsDavid Murphy80% (10)
- Tutorial Fpga Spartan-3eDocument53 pagesTutorial Fpga Spartan-3eCarlos Muñoz BacaNo ratings yet
- Soild VoidDocument5 pagesSoild VoidTanushree SalujaNo ratings yet
- P281 (En) SYS600 94 Operation 14042015Document191 pagesP281 (En) SYS600 94 Operation 14042015Victor SalazarNo ratings yet
- VHF Uhf Duoband Ant eDocument2 pagesVHF Uhf Duoband Ant eNol SatuNo ratings yet