Download as docx, pdf, or txt
You might also like
- Bupa Insurance Letter For Couple PDFDocument1 pageBupa Insurance Letter For Couple PDFumerbutt100No ratings yet
- ACORD Reference ArchitectureDocument24 pagesACORD Reference ArchitectureMiguel Angel Calderon Narvaez100% (2)
- DocxDocument5 pagesDocxAsdfghjkl LkjhgfdsaNo ratings yet
- Claim Form Regency For Expats PDFDocument2 pagesClaim Form Regency For Expats PDFChris DarkNo ratings yet
- Reimbursement Check ListDocument1 pageReimbursement Check Listscada.wupptclNo ratings yet
- Group Medi Prime ClaimFormDocument6 pagesGroup Medi Prime ClaimFormPravin Balasaheb GunjalNo ratings yet
- Claim Form RGICLDocument2 pagesClaim Form RGICLneninthe420No ratings yet
- IRDA Claim Form A - N - BDocument6 pagesIRDA Claim Form A - N - Bisha mittalNo ratings yet
- Domiciliary Treatment - Claim Form - Borl: Details of Primary InsuredDocument1 pageDomiciliary Treatment - Claim Form - Borl: Details of Primary InsuredHimanshu Chouksey100% (1)
- NEW Domiciliary Claim Form PDFDocument1 pageNEW Domiciliary Claim Form PDFHimanshu ChoukseyNo ratings yet
- 2-GMC Claim Check - ListDocument2 pages2-GMC Claim Check - ListChayan HalderNo ratings yet
- Intellicare Reimbursement Form UPDATEDDocument2 pagesIntellicare Reimbursement Form UPDATEDPhilip Sardan100% (2)
- Health Claim Form: Part A (To Be Filled by Insured)Document3 pagesHealth Claim Form: Part A (To Be Filled by Insured)Harshad DhodiNo ratings yet
- Claimant's Statement Form For Individual ClaimsDocument4 pagesClaimant's Statement Form For Individual ClaimsAshok GNo ratings yet
- OPD Claim Form - IGI GeneralDocument1 pageOPD Claim Form - IGI GeneralAmeen Khan NiaziNo ratings yet
- OPD Claim Form & ChecklistDocument1 pageOPD Claim Form & ChecklistumannamNo ratings yet
- Claim Checklist For MD-IndiaDocument1 pageClaim Checklist For MD-Indiadipankar0majumder100% (1)
- ApolloMunich-Easy HealthDocument9 pagesApolloMunich-Easy HealthRS CharyNo ratings yet
- MedicalDocument5 pagesMedicalankur parekhNo ratings yet
- Documents Check ListDocument1 pageDocuments Check ListFaizan ShaikhNo ratings yet
- Medicash Claim FormDocument6 pagesMedicash Claim Formwaran RMNo ratings yet
- IRDAI Registration No. 103. Reliance General Insurance Company LimitedDocument2 pagesIRDAI Registration No. 103. Reliance General Insurance Company LimitedSumit BhallaNo ratings yet
- Health Claim Form Part-BDocument3 pagesHealth Claim Form Part-BAnkit KanojiaNo ratings yet
- Request For Cashless HospitalisationDocument3 pagesRequest For Cashless HospitalisationJegatheswaran MNo ratings yet
- In-Patient Claim Form: (To Be Filled by Claimant Employee)Document2 pagesIn-Patient Claim Form: (To Be Filled by Claimant Employee)Khan LalaNo ratings yet
- Claim Form - Part-B - HospitalDocument4 pagesClaim Form - Part-B - HospitalMadhavi BobadeNo ratings yet
- Medical Insurance Claim Form (Corporate)Document3 pagesMedical Insurance Claim Form (Corporate)hari198902234No ratings yet
- Please Update Mentioned Mobile Number As Primary Contact Details Against My Policy. I Also Hereby Confirm To Be Contacted On The Number Provided Below For Claim Status /policy RenewalDocument4 pagesPlease Update Mentioned Mobile Number As Primary Contact Details Against My Policy. I Also Hereby Confirm To Be Contacted On The Number Provided Below For Claim Status /policy RenewalSumit BhallaNo ratings yet
- Reimbursement Form: 1 Patient InformationDocument1 pageReimbursement Form: 1 Patient InformationMuhammad ZubairNo ratings yet
- Reimbursement Request Form PDFDocument2 pagesReimbursement Request Form PDFLarrae Lucila100% (1)
- Claim Form B For HospitalDocument5 pagesClaim Form B For Hospitalbala249818No ratings yet
- Reimbursement Claim FormDocument6 pagesReimbursement Claim FormUmesh KatigharNo ratings yet
- 1 Claim FormDocument36 pages1 Claim Formkarmayukh1No ratings yet
- Reimbursement Request Form With Patient Member Undertaking (1) (1) (2) (1) 2Document2 pagesReimbursement Request Form With Patient Member Undertaking (1) (1) (2) (1) 2Bryan Joshua PandaanNo ratings yet
- ITGI Health Claim FormDocument6 pagesITGI Health Claim FormWifi Internet Cafe & Multi ServicesNo ratings yet
- Claim FormDocument2 pagesClaim FormsrikanthNo ratings yet
- Claim Form For Group Personal Accident PoliciesDocument4 pagesClaim Form For Group Personal Accident PoliciesanujaNo ratings yet
- MSH Reimbursement - Form - Dubai NewDocument1 pageMSH Reimbursement - Form - Dubai NewTarak FakhfakhNo ratings yet
- CMRF ApplicationDocument2 pagesCMRF Applicationismart shankarNo ratings yet
- Aditya Birla - Claim - FormDocument9 pagesAditya Birla - Claim - FormSaransh KumarNo ratings yet
- Health Claim - Form-1Document5 pagesHealth Claim - Form-1Pinakin PatelNo ratings yet
- Check ListDocument2 pagesCheck Listtyagi.vishal8323No ratings yet
- Disability Claim Form v3Document7 pagesDisability Claim Form v3arekp28978No ratings yet
- OPD Claim Form PDFDocument1 pageOPD Claim Form PDFSankar SaripalliNo ratings yet
- Claim Intimation Form Insurance 0Document2 pagesClaim Intimation Form Insurance 0Vishal SankheNo ratings yet
- Other Documents List Required From HospitalDocument1 pageOther Documents List Required From HospitalsudeekshahospitalnalgondaNo ratings yet
- NFM Cis Form v.061421Document1 pageNFM Cis Form v.061421Abby FernandezNo ratings yet
- 01 Adamjee In-Patient Claim Form EnglishDocument2 pages01 Adamjee In-Patient Claim Form EnglishsabaNo ratings yet
- Revised - Med Assistance Form - With CNDocument3 pagesRevised - Med Assistance Form - With CNchristine vizcondeNo ratings yet
- Claim Check ListDocument5 pagesClaim Check ListMahesh ShindeNo ratings yet
- Health Claim Intimation FormDocument3 pagesHealth Claim Intimation FormKiranmayi UppalaNo ratings yet
- Ahmedabad Claim FormDocument5 pagesAhmedabad Claim FormFirdaus PanthakyNo ratings yet
- IRDAI Registration No. 103. Reliance General Insurance Company LimitedDocument4 pagesIRDAI Registration No. 103. Reliance General Insurance Company LimitedSumit BhallaNo ratings yet
- CMRF Application FormDocument5 pagesCMRF Application FormMohammed AliNo ratings yet
- AMHI-new Claim Form PDFDocument4 pagesAMHI-new Claim Form PDFQwerty TNo ratings yet
- Easy Health Insurance Claim Form PDFDocument4 pagesEasy Health Insurance Claim Form PDFAnkithNo ratings yet
- Reimbursement Form: Patient Information 1Document1 pageReimbursement Form: Patient Information 1EslNo ratings yet
- Simba Health Application Form APA4Document1 pageSimba Health Application Form APA4Julia MuthoniNo ratings yet
- 05 - Domiciliary Claim FormDocument2 pages05 - Domiciliary Claim FormSAI SRI VLOGSNo ratings yet
- Paramount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceDocument2 pagesParamount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceMohammad AyazNo ratings yet
- Credit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!From EverandCredit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!Rating: 1 out of 5 stars1/5 (2)
- UGC Extension of Schemes Up To 2023 of MarchDocument3 pagesUGC Extension of Schemes Up To 2023 of Marchshafignits_123No ratings yet
- WWW - Manaresults.co - In: III B. Tech I Semester Supplementary Examinations, Dec/Jan - 2022-23 Digital CommunicationsDocument1 pageWWW - Manaresults.co - In: III B. Tech I Semester Supplementary Examinations, Dec/Jan - 2022-23 Digital Communicationsshafignits_123No ratings yet
- Ninth Class Model Paper (Ap) : Summative Assessment - Ii (2022)Document6 pagesNinth Class Model Paper (Ap) : Summative Assessment - Ii (2022)shafignits_123No ratings yet
- WWW - Manaresults.co - In: Code No: R1631044Document2 pagesWWW - Manaresults.co - In: Code No: R1631044shafignits_123No ratings yet
- Question BankDocument3 pagesQuestion Bankshafignits_123No ratings yet
- Prof K V SubbarajuDocument26 pagesProf K V Subbarajushafignits_123No ratings yet
- Ninth Class Model Paper (Ap) : Summative Assessment - Ii (2022)Document5 pagesNinth Class Model Paper (Ap) : Summative Assessment - Ii (2022)shafignits_123No ratings yet
- Ninth Class Model Paper (Ap) : Summative Assessment - IiDocument4 pagesNinth Class Model Paper (Ap) : Summative Assessment - Iishafignits_123No ratings yet
- Ninth Class Model Paper (Ap) : Summative Assessment - Ii (2022)Document5 pagesNinth Class Model Paper (Ap) : Summative Assessment - Ii (2022)shafignits_123No ratings yet
- Yogi Vemana University:: KadapaDocument16 pagesYogi Vemana University:: Kadapashafignits_123No ratings yet
- Yogi Vemana University:: KadapaDocument16 pagesYogi Vemana University:: Kadapashafignits_123No ratings yet
- Yogi Vemana University, Kadapa-516005, A.P., India.: Appendix II-Table 2: Academic/Research ScoreDocument4 pagesYogi Vemana University, Kadapa-516005, A.P., India.: Appendix II-Table 2: Academic/Research Scoreshafignits_123No ratings yet
- Speech Enhancement Using An Adaptive Wiener Filtering Approach M. A. Abd El-Fattah, M. I. Dessouky, S. M. Diab and F. E. Abd El-SamieDocument18 pagesSpeech Enhancement Using An Adaptive Wiener Filtering Approach M. A. Abd El-Fattah, M. I. Dessouky, S. M. Diab and F. E. Abd El-Samieshafignits_123No ratings yet
- Gate Form 12Document2 pagesGate Form 12shafignits_123No ratings yet
- Bocwwb Batch 4 Nominal RollDocument12 pagesBocwwb Batch 4 Nominal Rollshafignits_123No ratings yet
- View AnswerDocument1 pageView Answershafignits_123No ratings yet
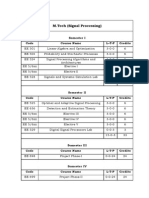
- M.Tech (Signal Processing) : Semester I Code Course Name L-T-P CreditsDocument1 pageM.Tech (Signal Processing) : Semester I Code Course Name L-T-P Creditsshafignits_123No ratings yet
- Daily Derivatives: ICICI Securities LTDDocument3 pagesDaily Derivatives: ICICI Securities LTDRohan KoliNo ratings yet
- Indian Fin-Tech Products Report 25042016 SecuredDocument51 pagesIndian Fin-Tech Products Report 25042016 Securedsumesh balakrishnanNo ratings yet
- E - MailDocument12 pagesE - Mailsullivan583No ratings yet
- DocumentDocument6 pagesDocumentBala RajuNo ratings yet
- E1 - FINACT1 - Proof of CashDocument1 pageE1 - FINACT1 - Proof of CashKevin James Sedurifa OledanNo ratings yet
- Statement 1664469716655Document22 pagesStatement 1664469716655salunkheclNo ratings yet
- Services Overview Guide NOKIADocument174 pagesServices Overview Guide NOKIACARLOS ONDARO MUÑOZNo ratings yet
- Role of RBI Under Banking Regulation Act, 1949Document11 pagesRole of RBI Under Banking Regulation Act, 1949Jay Ram100% (1)
- Time Division Multiple Access (Tdma)Document11 pagesTime Division Multiple Access (Tdma)LEEBAN MOSES MNo ratings yet
- Cisco 200-301 CCNA v2.4Document143 pagesCisco 200-301 CCNA v2.4Mohammad Arbi Al Ayubi100% (1)
- BS GroupingsDocument438 pagesBS GroupingsShivakumar RaoNo ratings yet
- Canadian Tire TPL CommentedDocument11 pagesCanadian Tire TPL CommentedDavid Tan100% (1)
- Pofrm 001Document3 pagesPofrm 001HR Executive TavoloNo ratings yet
- Liaison Officer Bookeeper Signature Over Printed Name/Date SignedDocument51 pagesLiaison Officer Bookeeper Signature Over Printed Name/Date SignedArmando LlidoNo ratings yet
- I ModeDocument7 pagesI Mode4.shilpiNo ratings yet
- BILLREPORTDocument3 pagesBILLREPORTjanakiramanmalligaNo ratings yet
- C3 - Problem 11 - Journalizing TransactionsDocument2 pagesC3 - Problem 11 - Journalizing TransactionsLorence John ImperialNo ratings yet
- Qa Si Ci WB PDFDocument11 pagesQa Si Ci WB PDFMeeNu KarthikNo ratings yet
- Local Literature and StudiesDocument4 pagesLocal Literature and StudiesRanniel Lazaro33% (3)
- Page 1 of 04: 030601525881??PUNA0101 842001Document5 pagesPage 1 of 04: 030601525881??PUNA0101 842001Rohit kumarNo ratings yet
- Struktur Organisasi (AR 2019)Document1 pageStruktur Organisasi (AR 2019)Annisa ZeinadinandaNo ratings yet
- Juhu To HotelDocument3 pagesJuhu To Hotelyesha60911No ratings yet
- Digital Marketing Class Notes Mid SemDocument62 pagesDigital Marketing Class Notes Mid SemJai KumarNo ratings yet
- UGRD-IT6201 Data Communications and Networking 1 QUIZ 1Document33 pagesUGRD-IT6201 Data Communications and Networking 1 QUIZ 1blandina o. mahayagNo ratings yet
- Quality of ServiceDocument370 pagesQuality of ServiceAvinashTripathiNo ratings yet
- 2021-08-02 Kristin - Invoice-Remote ControlDocument1 page2021-08-02 Kristin - Invoice-Remote ControlIvailo ZapryanovNo ratings yet