Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- NR 508 Test Bank PharmacologyDocument224 pagesNR 508 Test Bank PharmacologyChris100% (2)
- Greek and Roman Jewellery (Art History)Document168 pagesGreek and Roman Jewellery (Art History)MN D King Maker100% (4)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Power System Analysis II: Instructor: E-Mail: Office PhoneDocument66 pagesPower System Analysis II: Instructor: E-Mail: Office PhoneSelah TalepNo ratings yet
- ISKCON Desire Tree - Krishna Showing Universal FormDocument29 pagesISKCON Desire Tree - Krishna Showing Universal FormISKCON desire treeNo ratings yet
- Tube ClampDocument113 pagesTube ClampAmitava SilNo ratings yet
- Giesekus ModelDocument18 pagesGiesekus Modelvasopoli1No ratings yet
- SMOE Layout Man PDFDocument4 pagesSMOE Layout Man PDFCandrahasner SiregarNo ratings yet
- Determinação BcarotenoDocument2 pagesDeterminação BcarotenoAna Verônica Menezes de AguiarNo ratings yet
- Common Law Pleading Regarding Name ChangesDocument54 pagesCommon Law Pleading Regarding Name ChangesgmsapiensNo ratings yet
- Bio 1 SeriesDocument4 pagesBio 1 SerieskisesarevNo ratings yet
- Ca Q&aDocument129 pagesCa Q&aRavi TejaNo ratings yet
- Gradsaleh PDFDocument257 pagesGradsaleh PDFميرفت بكرى نمرNo ratings yet
- Xenon 2.2 4x2 148HP DC PDFDocument4 pagesXenon 2.2 4x2 148HP DC PDFshiksha torooNo ratings yet
- Java Programming LabDocument42 pagesJava Programming LabKeertiraj HajareNo ratings yet
- February 28 2014Document48 pagesFebruary 28 2014fijitimescanadaNo ratings yet
- KTM ContentsDocument4 pagesKTM Contentstahaqureshi123No ratings yet
- Teradata Interview QuestionsDocument11 pagesTeradata Interview QuestionsnarendrareddybanthiNo ratings yet
- PSY313-C Case SampleDocument16 pagesPSY313-C Case Samplefajrr loneNo ratings yet
- New DLL Physical ScienceDocument14 pagesNew DLL Physical ScienceFritzie MacalamNo ratings yet
- 1 Microbiology Course ContentDocument16 pages1 Microbiology Course ContentAziz AnisahNo ratings yet
- PandasDocument1,349 pagesPandasMichael GemminkNo ratings yet
- 7451 Planiseal288 GBDocument4 pages7451 Planiseal288 GBHendyKoNo ratings yet
- Jataka Tales 3 PDFDocument3 pagesJataka Tales 3 PDFGhosalNo ratings yet
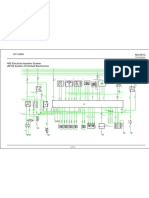
- Circuit Diagram: Ecu A/7Document1 pageCircuit Diagram: Ecu A/7RubénNo ratings yet
- Pedu 212 Physical Education Iii (Finals)Document7 pagesPedu 212 Physical Education Iii (Finals)Bea SaguinsinNo ratings yet
- Dynaco Mark VImanualDocument23 pagesDynaco Mark VImanualLeonardo MarraffiniNo ratings yet
- Challenges Q&AsDocument12 pagesChallenges Q&AsRaneesha MadurawalaNo ratings yet
- Selected Bibliography: Fundraising: Last Update: March 2009Document4 pagesSelected Bibliography: Fundraising: Last Update: March 2009Jorge Alberto Birrueta RubioNo ratings yet
- Mowbray SlidesCarnivalDocument30 pagesMowbray SlidesCarnivalschaNo ratings yet
- Eta Line 150-250Document32 pagesEta Line 150-250tafseerahmadNo ratings yet