Download as docx, pdf, or txt
You might also like
- NAPLEX Random Notes 68 PagesDocument57 pagesNAPLEX Random Notes 68 PagesThuan Tăng Nguyen100% (23)
- Biochemistry FinalDocument71 pagesBiochemistry FinalJanie-Vi Gorospe100% (2)
- Ganong Textbook of Medical PhysiologyDocument98 pagesGanong Textbook of Medical PhysiologyJanie-Vi Gorospe100% (1)
- Physio Pretest WordDocument143 pagesPhysio Pretest WordJanie-Vi Gorospe67% (3)
- Chemotherapy Question 1Document6 pagesChemotherapy Question 1Vaishali PrasharNo ratings yet
- Antibiotics: Microbial Control Antimicrobial AgentsDocument25 pagesAntibiotics: Microbial Control Antimicrobial AgentsMohammed Moutasim AyoubNo ratings yet
- Antibiotic Stewardship and Returning Travellers For 6 YearsDocument123 pagesAntibiotic Stewardship and Returning Travellers For 6 YearsPhaimNo ratings yet
- Antibiotic Resistance in Bacteria: Mbbs/Bds 1 Year 27.10.2010Document32 pagesAntibiotic Resistance in Bacteria: Mbbs/Bds 1 Year 27.10.2010احمد زيد سعيدNo ratings yet
- Quinolones Mechanisms of Action and Resistance - Course 94201 Sigal Ben-Yehuda - 10.1.2024Document59 pagesQuinolones Mechanisms of Action and Resistance - Course 94201 Sigal Ben-Yehuda - 10.1.2024yaellNo ratings yet
- Antibiotik Rasional - Dr. Truly SitorusDocument50 pagesAntibiotik Rasional - Dr. Truly Sitorusvina hidayatNo ratings yet
- Antibiotic 1Document13 pagesAntibiotic 1ريدان عياشNo ratings yet
- AB Lect2Document38 pagesAB Lect2Ivani Amelia CitraNo ratings yet
- Amr SeminarDocument48 pagesAmr SeminarSwijalNo ratings yet
- Antimicrobial Agents and ChemotherapyDocument139 pagesAntimicrobial Agents and ChemotherapyMonique BorresNo ratings yet
- Antimikroba-1Document21 pagesAntimikroba-1Richard MoralesNo ratings yet
- AntibioticsDocument5 pagesAntibioticsLaureece Salm ApduhanNo ratings yet
- All (Introduction To Anti-MicDocument3 pagesAll (Introduction To Anti-MicMiki AberaNo ratings yet
- Antibiotics in EndodonticsDocument74 pagesAntibiotics in EndodonticsdrishyaNo ratings yet
- Antiboitic - PHA-308Document14 pagesAntiboitic - PHA-308Nowfal Hasan SiamNo ratings yet
- Fomnya Et AlDocument13 pagesFomnya Et AlJesse IshayaNo ratings yet
- Antibiotics: General ConsiderationDocument50 pagesAntibiotics: General ConsiderationAyush ShrivastavaNo ratings yet
- Antibiotics, The Basics: Classification of Veterinary AntibioticsDocument2 pagesAntibiotics, The Basics: Classification of Veterinary Antibioticsgalihja100% (1)
- Antibiotik (Lengkap) - Dr. HamzahDocument117 pagesAntibiotik (Lengkap) - Dr. HamzahLusi MunawarohNo ratings yet
- ChemotherapyDocument66 pagesChemotherapyElias HaimanotNo ratings yet
- Antibacterial AgentsDocument44 pagesAntibacterial Agentsbelindasithole965No ratings yet
- Chemotherapy Lect 1Document26 pagesChemotherapy Lect 1kazelio2017No ratings yet
- Bacterial Resistance To Antibiotics: Reham Samir, PHD P18Document31 pagesBacterial Resistance To Antibiotics: Reham Samir, PHD P18Hadeer DaifAllahNo ratings yet
- 1a Antiinfective DrugsDocument4 pages1a Antiinfective DrugsMaria Donabella OngueNo ratings yet
- Antibiotics: Classification (Based On Mechanism of Action)Document35 pagesAntibiotics: Classification (Based On Mechanism of Action)Mohol DasNo ratings yet
- Antibiotic FinalDocument58 pagesAntibiotic Finalvandana kethavathNo ratings yet
- Bacteriostatic Agents: Drugs Which Bind To The 50s Ribosomal UnitDocument3 pagesBacteriostatic Agents: Drugs Which Bind To The 50s Ribosomal UnitJoshua Trinidad100% (1)
- Targeting Enzymes Involved in Chemotherapeutic AgentsDocument43 pagesTargeting Enzymes Involved in Chemotherapeutic AgentsAnuj DesaiNo ratings yet
- Pharmacology Solved Past PapersDocument10 pagesPharmacology Solved Past Papersfatima aghaNo ratings yet
- L P 6 Antibiotics - LAB - Fina - 2022Document33 pagesL P 6 Antibiotics - LAB - Fina - 2022Zakria Al-HadadNo ratings yet
- Antibiotic Classification and MechanismsDocument43 pagesAntibiotic Classification and Mechanismsyoza_kidNo ratings yet
- Pharma AntimicrobialsDocument19 pagesPharma AntimicrobialsYuku BabyNo ratings yet
- Reviewer PcolDocument3 pagesReviewer PcolMycaela Archivido De AlvaNo ratings yet
- Antimicrobial Drugs: Mechanism of Action & Resistance: R. Lia Iswara, DR, MS, SPMK Dept. of Microbiology FK UsuDocument16 pagesAntimicrobial Drugs: Mechanism of Action & Resistance: R. Lia Iswara, DR, MS, SPMK Dept. of Microbiology FK UsuDivika ShilvanaNo ratings yet
- New Drugs 2018: New Drug Mechanism of Action UseDocument7 pagesNew Drugs 2018: New Drug Mechanism of Action UsePremangshu GhoshalNo ratings yet
- MLS 044 Clinical Bacteriology Session 10Document5 pagesMLS 044 Clinical Bacteriology Session 10JJ AngNo ratings yet
- Abfghx Cfghheat Shfgheet Abx QNDocument6 pagesAbfghx Cfghheat Shfgheet Abx QNRăzvan RoșcaNo ratings yet
- Antibiotics in Periodontal DiseaseDocument57 pagesAntibiotics in Periodontal DiseaseReshmaaRajendranNo ratings yet
- Fuller AbxDocument78 pagesFuller AbxKe XuNo ratings yet
- Anti MicrobialDocument55 pagesAnti MicrobialNdayisaba CorneilleNo ratings yet
- New Drugs 2018 TableDocument5 pagesNew Drugs 2018 TableKirthikaRaghuramanNo ratings yet
- AntibacterialDocument18 pagesAntibacterialRafia Rayana btbcNo ratings yet
- Ch12 Part1Document15 pagesCh12 Part1lasanders601No ratings yet
- Resistance DevelopmentDocument44 pagesResistance Developmenttanvika katyayanNo ratings yet
- 2RS. 3 PneumoniaDocument33 pages2RS. 3 PneumoniaMuath AlqarniNo ratings yet
- Chemotherapy NotesDocument9 pagesChemotherapy Notesnileshkumarhjoshi942No ratings yet
- Chemotherapy ToxicityDocument37 pagesChemotherapy ToxicityCarlos Eduardo Cadu100% (1)
- 2 Antimicrobials and Mode of Action - 5 - 8 - 2014rshe - SuskaDocument14 pages2 Antimicrobials and Mode of Action - 5 - 8 - 2014rshe - SuskaIvan AguilarNo ratings yet
- Antibiotics & Antibiotic ResistanceDocument53 pagesAntibiotics & Antibiotic ResistanceLeenoos RayapanNo ratings yet
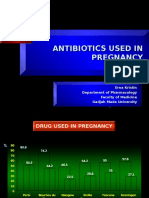
- Antibiotic Use in PregnancyDocument22 pagesAntibiotic Use in PregnancyRed DemonNo ratings yet
- AntimicrobialsDocument130 pagesAntimicrobialsPATRICK ROSHAN ANo ratings yet
- Mech. of Antibiotic ResistanceDocument20 pagesMech. of Antibiotic ResistanceDian NurmansyahNo ratings yet
- Mecanismo de Accao AntibioticoDocument1 pageMecanismo de Accao Antibioticocassimo2009No ratings yet
- New Drugs 2019: New Drug Mechanism of Action UseDocument6 pagesNew Drugs 2019: New Drug Mechanism of Action Userameez qureshiNo ratings yet
- 8.antimicrobial Control of MicrobesDocument69 pages8.antimicrobial Control of MicrobesSubhi MishraNo ratings yet
- Antibiotic Resistance, Part 2: Gram-Negative Pathogens: Catherine M. Oliphant, Pharmd, and Kathryn Eroschenko, PharmdDocument8 pagesAntibiotic Resistance, Part 2: Gram-Negative Pathogens: Catherine M. Oliphant, Pharmd, and Kathryn Eroschenko, PharmdSambit DashNo ratings yet
- Antibiotic ResistanceDocument32 pagesAntibiotic ResistanceEmine Alaaddinoglu100% (2)
- Antibiotics and FutureDocument16 pagesAntibiotics and FutureSachithNo ratings yet
- Katzung Pharmacology Semester 5 TablesDocument29 pagesKatzung Pharmacology Semester 5 TablesfatimaNo ratings yet
- Molecular and Cellular Biology of Pathogenic TrypanosomatidsFrom EverandMolecular and Cellular Biology of Pathogenic TrypanosomatidsNo ratings yet
- Final ICT OutputDocument5 pagesFinal ICT OutputJanie-Vi GorospeNo ratings yet
- Animal SloganDocument1 pageAnimal SloganJanie-Vi GorospeNo ratings yet
- Creative Output 1 - Bank Transaction SlipsDocument1 pageCreative Output 1 - Bank Transaction SlipsJanie-Vi GorospeNo ratings yet
- My How PosterDocument6 pagesMy How PosterJanie-Vi GorospeNo ratings yet
- Offline Task - Pronouns Crossword PuzzleDocument1 pageOffline Task - Pronouns Crossword PuzzleJanie-Vi GorospeNo ratings yet
- Go Grow GlowDocument10 pagesGo Grow GlowJanie-Vi GorospeNo ratings yet
- Grammar7 Sentence Fragments Exercise-210112-213611Document1 pageGrammar7 Sentence Fragments Exercise-210112-213611Janie-Vi GorospeNo ratings yet
- Grammar 7 Modifiers ExerciseDocument4 pagesGrammar 7 Modifiers ExerciseJanie-Vi GorospeNo ratings yet
- Orthodontics Transfer FormDocument1 pageOrthodontics Transfer FormJanie-Vi GorospeNo ratings yet
- Micro para - CompiledDocument94 pagesMicro para - CompiledJanie-Vi GorospeNo ratings yet
- RESP MEDICINE For PlabDocument73 pagesRESP MEDICINE For PlabJanie-Vi GorospeNo ratings yet
- Title: A Study of The Prevalence of Capilliariasis Philippinensis in Bagar and San Agustin, Candon, Ilocos SurDocument7 pagesTitle: A Study of The Prevalence of Capilliariasis Philippinensis in Bagar and San Agustin, Candon, Ilocos SurJanie-Vi GorospeNo ratings yet
- FAXCOM-Pharma March2019 (Repaired)Document15 pagesFAXCOM-Pharma March2019 (Repaired)Janie-Vi GorospeNo ratings yet
- April: Sunday Monday Tuesday Wednesday Thursday Friday SaturdayDocument1 pageApril: Sunday Monday Tuesday Wednesday Thursday Friday SaturdayJanie-Vi GorospeNo ratings yet
- Antibiotics ChartDocument10 pagesAntibiotics Chartadom09No ratings yet
- Usmle Pharm 3Document4 pagesUsmle Pharm 3sxymd321No ratings yet
- 11-Drugs Used in Meningitis Summary &questionsDocument6 pages11-Drugs Used in Meningitis Summary &questionsYousf SakrNo ratings yet
- AF SeedingDocument6 pagesAF SeedingdonkeyendutNo ratings yet
- XtendaDocument2 pagesXtendaAlexis CoronadoNo ratings yet
- Drug Study Ranitidine Citicoline Enalapril Aspilet Cefuroxime EtcDocument10 pagesDrug Study Ranitidine Citicoline Enalapril Aspilet Cefuroxime EtcmayeNo ratings yet
- Nelson's Pediatric Antimicrobial PDFDocument331 pagesNelson's Pediatric Antimicrobial PDFMADHANKUMAR MANICKAVELNo ratings yet
- Antibacterial and Anti Viral AgentsDocument51 pagesAntibacterial and Anti Viral AgentsabdeljelileNo ratings yet
- International Medical Guide For Ships (Quantification Addendum) Third EditionDocument58 pagesInternational Medical Guide For Ships (Quantification Addendum) Third EditionΔΗΜΗΤΡΗΣΧΑΛΑΤΣΗΣ100% (1)
- Guia IDSA-Practice Guidelines For The Management of Bacterial Meningitis-2004Document18 pagesGuia IDSA-Practice Guidelines For The Management of Bacterial Meningitis-2004Brenda Anali Pariona NapaNo ratings yet
- Lahiry 2021Document11 pagesLahiry 2021AsmaNo ratings yet
- Are Third Generation Cephalosporins Associated With A Bette - 2018 - Clinical MiDocument6 pagesAre Third Generation Cephalosporins Associated With A Bette - 2018 - Clinical MiRadia LachehebNo ratings yet
- Ceftriaxone-Induced Fatal Anaphylaxis Shock at An Emergency Department: A Case ReportDocument3 pagesCeftriaxone-Induced Fatal Anaphylaxis Shock at An Emergency Department: A Case ReportHeLena NukaNo ratings yet
- Blunt Abdominal Trauma MedicationDocument8 pagesBlunt Abdominal Trauma MedicationYudis Wira PratamaNo ratings yet
- Chapter 43 - Beta-LactamDocument7 pagesChapter 43 - Beta-LactamErika De JesusNo ratings yet
- Case Study 1 (Pneumonia)Document13 pagesCase Study 1 (Pneumonia)Kate EscotonNo ratings yet
- Differences Between Generations of CephalosporinsDocument3 pagesDifferences Between Generations of CephalosporinsAnkan PalNo ratings yet
- AntibioticsDocument7 pagesAntibioticsRahmania Eka SagitaNo ratings yet
- Farmakologi Jilid 2Document158 pagesFarmakologi Jilid 2TeguhsadjadNo ratings yet
- DRUG STUDY - Ceftriaxone (Forgram)Document2 pagesDRUG STUDY - Ceftriaxone (Forgram)julesubayubay5428100% (8)
- CURS ENGLEZA Boli InfectioaseDocument246 pagesCURS ENGLEZA Boli InfectioaseKiran LetrangeNo ratings yet
- Ceftriaxone + TazobactumDocument10 pagesCeftriaxone + Tazobactumnikoseamit7460100% (1)
- Drug Study For HPPDocument9 pagesDrug Study For HPPJennirose JingNo ratings yet
- DRUG STUDY For SrugeryDocument5 pagesDRUG STUDY For SrugeryZheyrille A. ArevaloNo ratings yet
- Lecture 10 Antibiotics & Antiinfectives-1Document39 pagesLecture 10 Antibiotics & Antiinfectives-1Dr Haris AwanNo ratings yet
- Mirah CMA Cost Minimization Analysis of Metformin and Acarbose in Treatment of Type 2 DiabetesDocument6 pagesMirah CMA Cost Minimization Analysis of Metformin and Acarbose in Treatment of Type 2 DiabetesRirin AptNo ratings yet
- CeftriaxoneDocument2 pagesCeftriaxoneunkown userNo ratings yet
- Antibiotics in Veterinary UseDocument83 pagesAntibiotics in Veterinary Usehansmeet100% (1)