Download as docx, pdf, or txt
You might also like
- 7E1 OperatingManualDocument2 pages7E1 OperatingManualSanjib Nath100% (1)
- Nurse Practitioner Board ReviewFrom EverandNurse Practitioner Board ReviewRating: 5 out of 5 stars5/5 (1)
- Annex 1a GlobalRoamer Locations and Mobile Network CoverageDocument34 pagesAnnex 1a GlobalRoamer Locations and Mobile Network CoverageHilmi FuadNo ratings yet
- Philadelphia Distilling Cocktail MenuDocument1 pagePhiladelphia Distilling Cocktail MenuEaterNo ratings yet
- Normal Newborn PP FinalDocument94 pagesNormal Newborn PP FinalTrisha Mae GalosNo ratings yet
- Neonatal Examination: by DR Ali Bel KheirDocument10 pagesNeonatal Examination: by DR Ali Bel KheirMohammed AlzergiNo ratings yet
- Normal Newborn PP Final-1Document97 pagesNormal Newborn PP Final-1ettevyviNo ratings yet
- 2pedia Newborn Disorder (Autosaved)Document64 pages2pedia Newborn Disorder (Autosaved)rajamjuhud1No ratings yet
- Assessment and Nursing Management Normal NewbornDocument17 pagesAssessment and Nursing Management Normal NewbornVinay Kp100% (1)
- 2 Newborn AssesmentDocument23 pages2 Newborn Assesment.No ratings yet
- SEMINAR ON Normal NewbornDocument133 pagesSEMINAR ON Normal Newborndipali dhayagudeNo ratings yet
- Examination of Newborn Physical Examination Include The FollowingDocument34 pagesExamination of Newborn Physical Examination Include The FollowingZimm Rrrr100% (2)
- The Newborn Infant RUBIADocument63 pagesThe Newborn Infant RUBIAmatucojulioNo ratings yet
- Newborn Assessment FinalDocument63 pagesNewborn Assessment FinalsanthiyasandyNo ratings yet
- Stage 1: During The First 30 Min. Through Which The Baby Is Characterized As PhysiologicallyDocument4 pagesStage 1: During The First 30 Min. Through Which The Baby Is Characterized As PhysiologicallyAmy LalringhluaniNo ratings yet
- 2 - Assessment of The NewbornDocument42 pages2 - Assessment of The NewbornDaenna Corrine JerezaNo ratings yet
- Immediate Newborn CareDocument9 pagesImmediate Newborn CareLj FerolinoNo ratings yet
- New Born, Infant and ToddlerDocument61 pagesNew Born, Infant and Toddlerمهند الرحيليNo ratings yet
- Newborn AssessmentDocument102 pagesNewborn Assessmentmolaf17696No ratings yet
- NewbornDocument193 pagesNewbornKenneth Myro Garcia100% (1)
- Newborns With Head Circumference of 37 or Less Than 33 Should Be Investigated For Neurologic InvolvementDocument3 pagesNewborns With Head Circumference of 37 or Less Than 33 Should Be Investigated For Neurologic InvolvementColleena CortesNo ratings yet
- Handouts Newborn AssessmentDocument21 pagesHandouts Newborn AssessmentjeromeNo ratings yet
- Content On New Born NNB&PNBDocument39 pagesContent On New Born NNB&PNBSabita JanaNo ratings yet
- Immediate Care of The Newborn and Newborn AssessmentDocument105 pagesImmediate Care of The Newborn and Newborn AssessmentAngela BautistaNo ratings yet
- Unit II The NewbornDocument47 pagesUnit II The NewbornmbolleaudreyNo ratings yet
- Nclex-Pn Chapter 21 BwfinalDocument12 pagesNclex-Pn Chapter 21 BwfinalatmojdNo ratings yet
- Neurologic Examination: Amanda Du, MD, Dpps Pediatrician-NeonatologistDocument91 pagesNeurologic Examination: Amanda Du, MD, Dpps Pediatrician-NeonatologistLyn LynNo ratings yet
- Elective - Neurologic Reporting 1Document23 pagesElective - Neurologic Reporting 1GenEsis CarandangNo ratings yet
- Apznzabuyifqyxfxvfewaduixp4nlcd7rqltsopbwaydxww5vzmvrn Fqdyjl 4ovwzyzezbcf82kwlrdq Zgkx1v2 Dofs Mmfmbce29ljhhe2kd6qz2x3zn Engb58mians8dtsvplx4izm4h Gwv2scw r0bmyktwv5zegdj4g9s Duxspj2oz1qjl4jsts23bumfy2p8gpwvzcjcxDocument186 pagesApznzabuyifqyxfxvfewaduixp4nlcd7rqltsopbwaydxww5vzmvrn Fqdyjl 4ovwzyzezbcf82kwlrdq Zgkx1v2 Dofs Mmfmbce29ljhhe2kd6qz2x3zn Engb58mians8dtsvplx4izm4h Gwv2scw r0bmyktwv5zegdj4g9s Duxspj2oz1qjl4jsts23bumfy2p8gpwvzcjcxRomm JacobNo ratings yet
- Maternal and ChildDocument33 pagesMaternal and Childjosephine100% (1)
- Physical Assessment of A Newborn BabyDocument17 pagesPhysical Assessment of A Newborn Babytibinj100% (1)
- Neural Tube Defect (Spina Bifida) : Guided by Presented byDocument41 pagesNeural Tube Defect (Spina Bifida) : Guided by Presented byShreyasi PatankarNo ratings yet
- Essential Newborns CareDocument18 pagesEssential Newborns CareJelly Yanquiling DumlaoNo ratings yet
- 11-Immediate Care of NewbornDocument112 pages11-Immediate Care of NewbornJiela CarbonillaNo ratings yet
- NCM 107 SL Finals EincDocument7 pagesNCM 107 SL Finals EincAngel DumlaoNo ratings yet
- Health Problems That Develop Among InfantsDocument86 pagesHealth Problems That Develop Among InfantsMaybelyn Dela CruzNo ratings yet
- Lesson 1. Pediatric WardDocument9 pagesLesson 1. Pediatric WardFlonamae AbiarNo ratings yet
- Care of New BornDocument25 pagesCare of New BornNirupama KsNo ratings yet
- Immediate Care of The NewbornDocument4 pagesImmediate Care of The Newbornmelinda100% (1)
- Systemic AssessmentDocument8 pagesSystemic AssessmentAmy LalringhluaniNo ratings yet
- Pediatric Nursing Common ProblemsDocument33 pagesPediatric Nursing Common ProblemsMaricel Agcaoili GallatoNo ratings yet
- Newborn Assessment by DR Dahir123Document84 pagesNewborn Assessment by DR Dahir123Najjuma BettyNo ratings yet
- NCM 209 PediaDocument76 pagesNCM 209 PediaJohn Cyprian AbeloNo ratings yet
- Newborn Assessment PDFDocument51 pagesNewborn Assessment PDFMilca DavidNo ratings yet
- Apgar Score May Be Influenced By: Preterm Birth Administration of Maternal Drugs Congenital AnomaliesDocument36 pagesApgar Score May Be Influenced By: Preterm Birth Administration of Maternal Drugs Congenital AnomaliesZimm RrrrNo ratings yet
- Hydrocephalus 170704144233Document56 pagesHydrocephalus 170704144233Pratyaksha TiwariNo ratings yet
- Characteristic of NewbornDocument9 pagesCharacteristic of Newbornbabyrainbow100% (15)
- Pedia-Reviewer CompleteDocument36 pagesPedia-Reviewer CompletePotato BroNo ratings yet
- Close During Embryonic Development Generally in The Lumbosacral RegionDocument24 pagesClose During Embryonic Development Generally in The Lumbosacral RegionPotato BroNo ratings yet
- Case 2 Hydrocephalus Group 4Document27 pagesCase 2 Hydrocephalus Group 4younggirldavidNo ratings yet
- Ob Peds Lecture Notes Nurse NursingDocument70 pagesOb Peds Lecture Notes Nurse Nursinglilchibaby3161100% (2)
- Danger Signs in NewbornDocument8 pagesDanger Signs in NewbornPrabhu MagudeeswaranNo ratings yet
- Care of The Normal Newborn: M. Rogers-Walker, MSN/Ed, RNDocument28 pagesCare of The Normal Newborn: M. Rogers-Walker, MSN/Ed, RNyanetp01No ratings yet
- Neonatology Lec1 2023Document17 pagesNeonatology Lec1 2023khaleelNo ratings yet
- Newborn Care 101 2nd SemDocument18 pagesNewborn Care 101 2nd SemFilamae Jayahr CadayNo ratings yet
- Pediatric Emergencies: DR Khalid RashedDocument32 pagesPediatric Emergencies: DR Khalid RashedMuhamad FaridNo ratings yet
- Pediatric Emergencies 1Document32 pagesPediatric Emergencies 1Muhamad FaridNo ratings yet
- Birthinjuries Dr.M.maniDocument65 pagesBirthinjuries Dr.M.manimaniNo ratings yet
- Newborn AssessmentDocument17 pagesNewborn Assessmentmarycris100% (3)
- Nursing Care of The New Born InfantDocument37 pagesNursing Care of The New Born Infantnila_sarichandraNo ratings yet
- The Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaFrom EverandThe Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaNo ratings yet
- Syringomyelia, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandSyringomyelia, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- Torque Values RTJ (B16.5)Document3 pagesTorque Values RTJ (B16.5)ariyamanjulaNo ratings yet
- Causes of MeanderingDocument1 pageCauses of MeanderingBalagopal V50% (2)
- Operator's Manual: Hydril K20-5000 Pulsation Dampener IAW PED 97/23/ECDocument16 pagesOperator's Manual: Hydril K20-5000 Pulsation Dampener IAW PED 97/23/ECAli Ali67% (3)
- Green PowerDocument20 pagesGreen PowerNishanth SubramaniNo ratings yet
- 68406-Ch 02Document28 pages68406-Ch 02Kirat Kamboz100% (1)
- IFAS System Troubleshooting Guide DraftDocument18 pagesIFAS System Troubleshooting Guide Draftsoumya pattanaikNo ratings yet
- SJNHC 212 431-434Document4 pagesSJNHC 212 431-434DAICY CULTURANo ratings yet
- Diseases of Lungs BLACKWOODDocument360 pagesDiseases of Lungs BLACKWOODG AnshuNo ratings yet
- EE311A 2021 AV Slides L23Document13 pagesEE311A 2021 AV Slides L23Ananya AgarwalNo ratings yet
- AFP Brochure08Document4 pagesAFP Brochure08YongoloooNo ratings yet
- Mining Iii To Viii PDFDocument77 pagesMining Iii To Viii PDFRaja Prabhu0% (1)
- Hypnisis in PsychosomaticsDocument3 pagesHypnisis in PsychosomaticsJoseph MeyersonNo ratings yet
- Erection and Painting of Steel StructureDocument7 pagesErection and Painting of Steel StructureTAHER AMMARNo ratings yet
- Why Integration Is The Key To Asia's Economic Progress? Explain Your AnswerDocument2 pagesWhy Integration Is The Key To Asia's Economic Progress? Explain Your AnswerQueeny JavierNo ratings yet
- Section 05505 METAL FABRICATIONS PDFDocument13 pagesSection 05505 METAL FABRICATIONS PDFIm ChinithNo ratings yet
- G4 Chem BoilingDocument5 pagesG4 Chem BoilingNashwaAlinsangaoNo ratings yet
- Reynolds, 2014Document8 pagesReynolds, 2014Joana ComiranNo ratings yet
- AventDocument9 pagesAventgushjonesNo ratings yet
- Family Law OutlineDocument44 pagesFamily Law OutlineBudleigh SaltertonNo ratings yet
- How To Make Lye For Natural Soap Making From Wood AshDocument7 pagesHow To Make Lye For Natural Soap Making From Wood AshMeim HakkasNo ratings yet
- Unmsm/Fqiq/Epiq/Daadp/Inglés TÉCNICO/EF5/2020-I: Section V: The Impact of Chemical Engineering Design On SocietyDocument3 pagesUnmsm/Fqiq/Epiq/Daadp/Inglés TÉCNICO/EF5/2020-I: Section V: The Impact of Chemical Engineering Design On SocietyJuanLopezTrujilloNo ratings yet
- Kiểm tra môn Học tốt Tiếng Anh 10 (Hệ 10 năm)Document4 pagesKiểm tra môn Học tốt Tiếng Anh 10 (Hệ 10 năm)Phương Ngọc LạiNo ratings yet
- Screening Test-EngDocument17 pagesScreening Test-EngJeffrey VallenteNo ratings yet
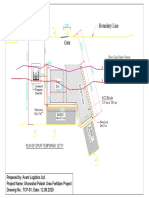
- Boundary Line: Plan of Gpuff Temporary JettyDocument1 pageBoundary Line: Plan of Gpuff Temporary Jettyshafiq_05No ratings yet
- Lab Manual Separation Tech Jan 2021Document43 pagesLab Manual Separation Tech Jan 2021Abdul QayyumNo ratings yet
- instaPDF - in Indian Grocery Items List 836Document16 pagesinstaPDF - in Indian Grocery Items List 836Namita BhattNo ratings yet
- Planning Considerations For Ice PlantsDocument5 pagesPlanning Considerations For Ice PlantsribozymesNo ratings yet