Download as pdf or txt
You might also like
- Green Wedge Urbanism History, Theory and Contemporary PracticeDocument302 pagesGreen Wedge Urbanism History, Theory and Contemporary PracticeTeodora FlrNo ratings yet
- Manual of Planktonic Foraminifera, Postuma 1971 (OCR)Document241 pagesManual of Planktonic Foraminifera, Postuma 1971 (OCR)Fauziah Parakkasi0% (1)
- KM Instructor Course Phase 1aDocument22 pagesKM Instructor Course Phase 1anozza_1No ratings yet
- 26 - LCCI L3 AC - Sep 2019 - ASE 20104 - MSDocument15 pages26 - LCCI L3 AC - Sep 2019 - ASE 20104 - MSKhin Zaw Htwe100% (6)
- Reliability and Validity of Measuring RespirationDocument5 pagesReliability and Validity of Measuring RespirationFlávio LuzNo ratings yet
- Breathing Exercises Influence On Breathing Patterns and HEALTH PEOPLEDocument9 pagesBreathing Exercises Influence On Breathing Patterns and HEALTH PEOPLEKang IljungNo ratings yet
- ViewDocument7 pagesViewAnandhu GNo ratings yet
- Breathing Movements of The Chest and Abdominal Wall in Healthy SubjectsDocument10 pagesBreathing Movements of The Chest and Abdominal Wall in Healthy SubjectsAnandhu GNo ratings yet
- Maintenance of Inspiratory Muscle Training in COPD Patients: One Year Follow-UpDocument5 pagesMaintenance of Inspiratory Muscle Training in COPD Patients: One Year Follow-UpGaoudam NatarajanNo ratings yet
- En V36n6a11 PDFDocument8 pagesEn V36n6a11 PDFJuly Andrea Cepeda MartínezNo ratings yet
- BwapDocument27 pagesBwapMagister KeperawatanNo ratings yet
- 10 3390@medicina57070702Document7 pages10 3390@medicina57070702Einar Cumplido MartínezNo ratings yet
- The Effects of Breath-Counting Meditation and Deep Breathing On Heart Rate VariabilityDocument9 pagesThe Effects of Breath-Counting Meditation and Deep Breathing On Heart Rate VariabilityMadame MoseilleNo ratings yet
- PNF 7 The Effect of Trunk Stability Excercise Using Stabilising ReservalDocument9 pagesPNF 7 The Effect of Trunk Stability Excercise Using Stabilising ReservalAnonymous j0xAgHs3No ratings yet
- Journal - Lung Function Changes in Young Obese Women - A Harbinger For Graver OutcomesDocument6 pagesJournal - Lung Function Changes in Young Obese Women - A Harbinger For Graver OutcomesSondang Farwaty SitanggangNo ratings yet
- Ejercicio DiafragmaticoDocument3 pagesEjercicio DiafragmaticoN onlyNo ratings yet
- 슈로스 (Schroth) 운동치료와 슬링운동치료가 척추측만증 환자의 유연성, 균형능력, 척추각 및 흉곽 확장에 미치는 효과 비교Document13 pages슈로스 (Schroth) 운동치료와 슬링운동치료가 척추측만증 환자의 유연성, 균형능력, 척추각 및 흉곽 확장에 미치는 효과 비교kang soon cheolNo ratings yet
- Optoelectronic PlethysmographyDocument15 pagesOptoelectronic PlethysmographygothicmetalspiritNo ratings yet
- Upper Thoracic Spine Mobilization and Mobility Exercise Versus Upper Cervical Spine Mobilization and Stabilization Exercise in Individuals With Forward Head Posture - A Randomized Clinical Trial - PMCDocument21 pagesUpper Thoracic Spine Mobilization and Mobility Exercise Versus Upper Cervical Spine Mobilization and Stabilization Exercise in Individuals With Forward Head Posture - A Randomized Clinical Trial - PMCEri KafexhiNo ratings yet
- 10a Artikel Measuring Chest ExpansionDocument5 pages10a Artikel Measuring Chest ExpansionSribharath SekarNo ratings yet
- Breathing Exercise of ScoliosisDocument3 pagesBreathing Exercise of Scoliosisrima rizky nourliaNo ratings yet
- MRI DiaphragmDocument13 pagesMRI Diaphragmhari vijayNo ratings yet
- Nutritional Methodology: Self-Reported and Technician-Measured Waist Circumferences Differ in Middle-Aged Men and WomenDocument8 pagesNutritional Methodology: Self-Reported and Technician-Measured Waist Circumferences Differ in Middle-Aged Men and Womenapi-19890414No ratings yet
- Body Position Influences The Maximum Inspiratory and Expiratory Mouth Pressures of Young Healthy SubjectsDocument3 pagesBody Position Influences The Maximum Inspiratory and Expiratory Mouth Pressures of Young Healthy SubjectsJoecoNo ratings yet
- International Journal of Pharma and Bio Sciences: Research Article Human PhysiologyDocument6 pagesInternational Journal of Pharma and Bio Sciences: Research Article Human PhysiologyajenggayatriNo ratings yet
- Stabil Function DiaphragmDocument21 pagesStabil Function DiaphragmMarcus LimaNo ratings yet
- JurnalDocument10 pagesJurnalAlifia RizqiNo ratings yet
- Respiratory Physiology & Neurobiology: Chest Wall Volumes During Inspiratory Loaded Breathing in Copd PatientsDocument6 pagesRespiratory Physiology & Neurobiology: Chest Wall Volumes During Inspiratory Loaded Breathing in Copd Patientsdaniel pasaribuNo ratings yet
- PDF 3Document9 pagesPDF 3Icha Chaphedech hildantraNo ratings yet
- Jurnal Rms 3Document9 pagesJurnal Rms 3zuhuda piliNo ratings yet
- Chest Expansion and Lung FunctionDocument8 pagesChest Expansion and Lung FunctionHammed BolajiNo ratings yet
- Cervical Traction For Neck Pain Patients A Clinical Prediction Rule 1266428336Document4 pagesCervical Traction For Neck Pain Patients A Clinical Prediction Rule 1266428336qwrertyuiopNo ratings yet
- Postural Awareness and Its Relation To Pain ValidaDocument11 pagesPostural Awareness and Its Relation To Pain ValidacderosasNo ratings yet
- Comparacion Articulos de Tres Ejercicios para Manguito Rotador en InglesDocument26 pagesComparacion Articulos de Tres Ejercicios para Manguito Rotador en IngleskarolndNo ratings yet
- IAP PaperDocument9 pagesIAP PaperGustavo Javier Caraballo PeñaNo ratings yet
- Qigong and Cop DDocument11 pagesQigong and Cop DRodrigo EzequielNo ratings yet
- 2018 Article 2031Document10 pages2018 Article 2031marcelonorisNo ratings yet
- 10 4328acam 6123Document4 pages10 4328acam 6123Muhammad AbdullahNo ratings yet
- Physiotherapy - 2015 - Pascoal - Abdominal Exercises Affect Inter-Rectus Distance in Postpartum Women - A Two-Dimensional Ultrasound StudyDocument7 pagesPhysiotherapy - 2015 - Pascoal - Abdominal Exercises Affect Inter-Rectus Distance in Postpartum Women - A Two-Dimensional Ultrasound StudyEwerton ElooyNo ratings yet
- Hamstring Length in Patellofemoral Pain Syndrome: Lisa C. White, Philippa Dolphin, John DixonDocument5 pagesHamstring Length in Patellofemoral Pain Syndrome: Lisa C. White, Philippa Dolphin, John DixonMamedNo ratings yet
- Comparison of Postural Sway Depending On Balance Pad TypeDocument6 pagesComparison of Postural Sway Depending On Balance Pad TypeElena MathewNo ratings yet
- Does The Addition of Manual Therapy Approach To A Cervical Exercise Program Improve Clinical Outcomes For Patients With Chronic Neck Pain in Short - and Mid-Term? A Randomized Controlled Trial - PMCDocument26 pagesDoes The Addition of Manual Therapy Approach To A Cervical Exercise Program Improve Clinical Outcomes For Patients With Chronic Neck Pain in Short - and Mid-Term? A Randomized Controlled Trial - PMCEri KafexhiNo ratings yet
- Ojsadmin, 279Document5 pagesOjsadmin, 279Muhammad FaizanNo ratings yet
- Crunch en Diastasis AbdominalDocument6 pagesCrunch en Diastasis AbdominalFlorencia Robuschi feestNo ratings yet
- PNF 22 The Effects of PNF and Trunk Stabilization Robot Training On Trunk Stability and Balance in Patients With Chronic StrokeDocument11 pagesPNF 22 The Effects of PNF and Trunk Stabilization Robot Training On Trunk Stability and Balance in Patients With Chronic StrokeAnonymous j0xAgHs3No ratings yet
- Tmpa535 TMPDocument6 pagesTmpa535 TMPFrontiersNo ratings yet
- Zarna Ethical NewDocument19 pagesZarna Ethical Newnandu_rajNo ratings yet
- Lung Function and Breathing Regulation Parameters During PregnancyDocument6 pagesLung Function and Breathing Regulation Parameters During PregnancyFaizah ShabrinaNo ratings yet
- Viegas Et Al. The Inter - and Intra-Rater Reliability of The Manual Diaphragm Assessment Scale in HealtDocument7 pagesViegas Et Al. The Inter - and Intra-Rater Reliability of The Manual Diaphragm Assessment Scale in HealtMilton Ricardo de Medeiros FernandesNo ratings yet
- Benefits of High-Intensity Exercise Training To Patients With Chronic Obstructive Pulmonary Disease: A Controlled StudyDocument10 pagesBenefits of High-Intensity Exercise Training To Patients With Chronic Obstructive Pulmonary Disease: A Controlled StudyCésarNo ratings yet
- MainDocument10 pagesMainMu RakimNo ratings yet
- Single Leg Stace ScopusDocument3 pagesSingle Leg Stace ScopusUmrohtul HabibahNo ratings yet
- Effects of Stabilization Exercise Using Flexi-Bar OnDocument5 pagesEffects of Stabilization Exercise Using Flexi-Bar OnYoh ChenNo ratings yet
- JKPT027 03 169Document5 pagesJKPT027 03 169Hendra Guntur BarunaNo ratings yet
- Study The Relation Between Body Mass Index, Waist Circumference and Spirometry in COPD PatientsDocument7 pagesStudy The Relation Between Body Mass Index, Waist Circumference and Spirometry in COPD PatientsFidyatul NazhiraNo ratings yet
- Herakova PDFDocument7 pagesHerakova PDFIwan SusantoNo ratings yet
- Aluko2013 2Document11 pagesAluko2013 2Dr Ahmed NabilNo ratings yet
- The effect of smartphone usage time on posture and respiratory functionDocument4 pagesThe effect of smartphone usage time on posture and respiratory functionl.cepeda01No ratings yet
- Comparison of Three Types of Exc in The Treatment of Rotator Cuff TendinopathyShoulder Impingement SyndromeDocument7 pagesComparison of Three Types of Exc in The Treatment of Rotator Cuff TendinopathyShoulder Impingement SyndromeKholis RedcrossNo ratings yet
- Biomechanical Classification Based On Lumnbo Pelvic RhythmDocument12 pagesBiomechanical Classification Based On Lumnbo Pelvic Rhythmhari vijayNo ratings yet
- Minimum Clinically Important Improvement For The Incremental Shuttle Walking TestDocument4 pagesMinimum Clinically Important Improvement For The Incremental Shuttle Walking TestmavhelllinaNo ratings yet
- Respiratory Physiology & NeurobiologyDocument5 pagesRespiratory Physiology & NeurobiologynimaaandmNo ratings yet
- A Century of Gibberellin ResearchDocument21 pagesA Century of Gibberellin ResearchMellya RizkiNo ratings yet
- Gibberellin Localization and Transport in Plants: ReviewDocument12 pagesGibberellin Localization and Transport in Plants: ReviewMellya RizkiNo ratings yet
- Male Black Widows Parasitize Mate-Searching Effort of Rivals To Find Females FasterDocument9 pagesMale Black Widows Parasitize Mate-Searching Effort of Rivals To Find Females FasterMellya RizkiNo ratings yet
- Ear Structures of The Naked Mole-Rat, (Rodentia: Bathyergidae)Document28 pagesEar Structures of The Naked Mole-Rat, (Rodentia: Bathyergidae)Mellya RizkiNo ratings yet
- Hypersensitivity To Drugs and Their Mechanisms: Name: Mellya Rizki Pitriani Student ID: B1B017031Document10 pagesHypersensitivity To Drugs and Their Mechanisms: Name: Mellya Rizki Pitriani Student ID: B1B017031Mellya RizkiNo ratings yet
- Somche2015 Paper1 PDFDocument16 pagesSomche2015 Paper1 PDFMellya RizkiNo ratings yet
- Mayakun 2019Document9 pagesMayakun 2019Mellya RizkiNo ratings yet
- Transcriptomic Changes Associated With Pregnancy in A Marsupial, The Gray Short-Tailed Opossum Monodelphis DomesticaDocument25 pagesTranscriptomic Changes Associated With Pregnancy in A Marsupial, The Gray Short-Tailed Opossum Monodelphis DomesticaMellya RizkiNo ratings yet
- Journal Pone 0221824Document69 pagesJournal Pone 0221824Mellya RizkiNo ratings yet
- The Rod Signaling Pathway in Marsupial RetinaeDocument19 pagesThe Rod Signaling Pathway in Marsupial RetinaeMellya RizkiNo ratings yet
- Christie 2015Document18 pagesChristie 2015Mellya RizkiNo ratings yet
- Mota 2016Document9 pagesMota 2016Mellya RizkiNo ratings yet
- Hori 2018Document5 pagesHori 2018Mellya RizkiNo ratings yet
- Acara 5 Kultur OrganDocument11 pagesAcara 5 Kultur OrganMellya RizkiNo ratings yet
- The Transcriptional Landscape of Streptococcus Architecture and Abundant Riboregulation Critical For Growth and VirulenceDocument25 pagesThe Transcriptional Landscape of Streptococcus Architecture and Abundant Riboregulation Critical For Growth and VirulenceMellya RizkiNo ratings yet
- Current Insights Into The Role of Rhizosphere Bacteria in Disease Suppressive SoilsDocument12 pagesCurrent Insights Into The Role of Rhizosphere Bacteria in Disease Suppressive SoilsMellya RizkiNo ratings yet
- 1 s2.0 S0300908418302955 MainDocument12 pages1 s2.0 S0300908418302955 MainMellya RizkiNo ratings yet
- Coral Lecture PDFDocument58 pagesCoral Lecture PDFMellya RizkiNo ratings yet
- Table 3.1. Result of Monolayer Cell Culture of Group II Observation Incubator Temperature Medium Color Cell Attachment Cell ConfluencyDocument3 pagesTable 3.1. Result of Monolayer Cell Culture of Group II Observation Incubator Temperature Medium Color Cell Attachment Cell ConfluencyMellya RizkiNo ratings yet
- Journal Pone 0206085Document14 pagesJournal Pone 0206085Mellya RizkiNo ratings yet
- Genetic Engineering Practical ReportDocument4 pagesGenetic Engineering Practical ReportMellya RizkiNo ratings yet
- Culturomics-Based Taxonomic Diversity of Bacterial Communities in The Hot Springs of Saudi ArabiaDocument11 pagesCulturomics-Based Taxonomic Diversity of Bacterial Communities in The Hot Springs of Saudi ArabiaMellya RizkiNo ratings yet
- Annelida and EchinodermataDocument8 pagesAnnelida and EchinodermataMellya RizkiNo ratings yet
- Bacterium From A Marine Oligotrophic Environment: Sphingomonas Alaskensis Sp. Nov., A DominantDocument8 pagesBacterium From A Marine Oligotrophic Environment: Sphingomonas Alaskensis Sp. Nov., A DominantMellya RizkiNo ratings yet
- Engineering Management 5 - ControllingDocument46 pagesEngineering Management 5 - ControllingCraig PeriNo ratings yet
- Thời gian làm bài 120 phút, không kể thời gian giao đềDocument9 pagesThời gian làm bài 120 phút, không kể thời gian giao đềĐỗ Hoàng DũngNo ratings yet
- SUBWAY EditedDocument13 pagesSUBWAY Editedsonaxiv697No ratings yet
- (Download PDF) Managerial Accounting An Introduction To Concepts Methods and Uses 11th Edition Maher Solutions Manual Full ChapterDocument40 pages(Download PDF) Managerial Accounting An Introduction To Concepts Methods and Uses 11th Edition Maher Solutions Manual Full Chapterallenabeshay52100% (9)
- RMA Planing Guide 200708 v1 1-1-36Document36 pagesRMA Planing Guide 200708 v1 1-1-36viswanath_manjulaNo ratings yet
- 15 3 16 - p.325 331 PDFDocument7 pages15 3 16 - p.325 331 PDFbeatcookNo ratings yet
- Fermi LevelDocument13 pagesFermi LevelArchit P. MeshramNo ratings yet
- Book Review of I Love You Since 1892Document2 pagesBook Review of I Love You Since 1892hannah100% (1)
- HUC Program Grading SchemeDocument1 pageHUC Program Grading SchemeThanis RaoNo ratings yet
- TR - Dressmaking NC IIDocument60 pagesTR - Dressmaking NC IIMR. CHRISTIAN DACORONNo ratings yet
- Ielts Reading Test 40Document8 pagesIelts Reading Test 40Samarth BajajNo ratings yet
- Insight in Inpatients With Psychotic Mania Demographic and Clinical FactorsDocument13 pagesInsight in Inpatients With Psychotic Mania Demographic and Clinical FactorsmusdalifahNo ratings yet
- Slides 4tl4Document312 pagesSlides 4tl4Isac AareiasNo ratings yet
- Avenida de Balide - Antigo Comarca Balide, Dili TLF.: (+670) 3310315 11111Document2 pagesAvenida de Balide - Antigo Comarca Balide, Dili TLF.: (+670) 3310315 11111iduyNo ratings yet
- The Digital Cast of Being Metaphysics Mathematics Cartesianism Cybernetics Capitalism CommunicationDocument215 pagesThe Digital Cast of Being Metaphysics Mathematics Cartesianism Cybernetics Capitalism CommunicationSilvia M. EsparzaOviedoNo ratings yet
- HP ZBOOK 17 QUICKSPECS c04111344Document45 pagesHP ZBOOK 17 QUICKSPECS c04111344hutz5000No ratings yet
- Yahoo Mail - PCN Number Request For - WV20UOYDocument2 pagesYahoo Mail - PCN Number Request For - WV20UOYVicky RathodNo ratings yet
- Thai RecipesDocument123 pagesThai Recipesmariana_luca_17100% (5)
- WH1602W Tmi JTDocument29 pagesWH1602W Tmi JTscribe72No ratings yet
- Self-Awareness To Being Watched and Socially-Desirable Behavior: A Field Experiment On The Effect of Body-Worn Cameras On Police Use-Of-ForceDocument14 pagesSelf-Awareness To Being Watched and Socially-Desirable Behavior: A Field Experiment On The Effect of Body-Worn Cameras On Police Use-Of-ForcePoliceFoundationNo ratings yet
- Lab 3 Cell Permeability 2013Document14 pagesLab 3 Cell Permeability 2013Andrew MartiniNo ratings yet
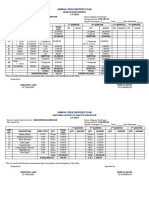
- Annual Procurement Plan-AppDocument6 pagesAnnual Procurement Plan-AppJonas MapacpacNo ratings yet
- Kelompok 2 - Ilmu Link. - Kelas E - Lecture 12Document11 pagesKelompok 2 - Ilmu Link. - Kelas E - Lecture 12SITI NUR AULIANo ratings yet
- ExamenesDocument4 pagesExamenesZareli Lazo AriasNo ratings yet
- A Recommender System Based On PersonalDocument15 pagesA Recommender System Based On Personalreiko-sanNo ratings yet
- Error Analysis in Physics PDFDocument2 pagesError Analysis in Physics PDFKrystal0% (1)