Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5824)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Leetcode Solutions in JavaDocument2 pagesLeetcode Solutions in JavaKunal KapoorNo ratings yet
- Membaca Ro PaulusDocument73 pagesMembaca Ro PaulusRhomadhoni Ika PutraNo ratings yet
- External Fixation and Temporary Stabilization of Femoral and Tibial Part 1Document8 pagesExternal Fixation and Temporary Stabilization of Femoral and Tibial Part 1Rhomadhoni Ika PutraNo ratings yet
- TombRaider LogDocument4 pagesTombRaider LogRhomadhoni Ika PutraNo ratings yet
- Osteogenisis Imperfecta: Christopher LimDocument34 pagesOsteogenisis Imperfecta: Christopher LimRhomadhoni Ika PutraNo ratings yet
- Elbow PainDocument9 pagesElbow PainRhomadhoni Ika PutraNo ratings yet
- Cervical PainDocument4 pagesCervical PainRhomadhoni Ika PutraNo ratings yet
- Peta Pasien Orthopaedi Senin 23 November 2015 Mia/Fat/Aai/Hdd/Cid/Dli/Dak/Mad/Asd/Git/Aip/Gas/Aan/Nrm/Anh/Scp/Fad/Epp/MpkDocument1 pagePeta Pasien Orthopaedi Senin 23 November 2015 Mia/Fat/Aai/Hdd/Cid/Dli/Dak/Mad/Asd/Git/Aip/Gas/Aan/Nrm/Anh/Scp/Fad/Epp/MpkRhomadhoni Ika PutraNo ratings yet
- Peta Pasien Orthopaedi Minggu 22 November 2015 Mia/Fat/Aai/Hdd/Cid/Dli/Dak/Mad/Asd/Git/Aip/Gas/Aan/Nrm/Anh/Scp/Fad/Epp/MpkDocument1 pagePeta Pasien Orthopaedi Minggu 22 November 2015 Mia/Fat/Aai/Hdd/Cid/Dli/Dak/Mad/Asd/Git/Aip/Gas/Aan/Nrm/Anh/Scp/Fad/Epp/MpkRhomadhoni Ika PutraNo ratings yet
- Peta Pasien Orthopaedi Sabtu, 21 November 2015 Mia/Fat/Aai/Hdd/Cid/Dli/Dak/Mad/Asd/Git/Aip/Gas/Aan/Nrm/Anh/Scp/Fad/Epp/MpkDocument1 pagePeta Pasien Orthopaedi Sabtu, 21 November 2015 Mia/Fat/Aai/Hdd/Cid/Dli/Dak/Mad/Asd/Git/Aip/Gas/Aan/Nrm/Anh/Scp/Fad/Epp/MpkRhomadhoni Ika PutraNo ratings yet
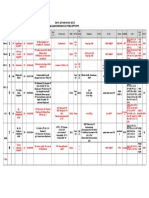
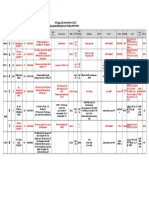
- Peta Pasien Orthopaedi Minggu, 2 AGUSTUS 2015 Soe/Fdl/Arv/Hdd/Cid/Dli/Dak/Mad/Asd/Git/Aip/Gas/Ady/Adh/Via/Ewi/Har/Dim/HboDocument2 pagesPeta Pasien Orthopaedi Minggu, 2 AGUSTUS 2015 Soe/Fdl/Arv/Hdd/Cid/Dli/Dak/Mad/Asd/Git/Aip/Gas/Ady/Adh/Via/Ewi/Har/Dim/HboRhomadhoni Ika PutraNo ratings yet
- Mapping 7 AGUSTUS 2015Document1 pageMapping 7 AGUSTUS 2015Rhomadhoni Ika PutraNo ratings yet
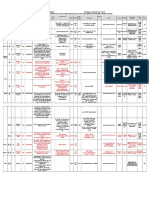
- Peta Pasien Orthopaedi Sabtu, 1 Agustus 2015 Soe/Fdl/Arv/Hdd/Cid/Dli/Dak/Mad/Asd/Git/Aip/Gas/Ady/Adh/Via/Ewi/Har/Dim/HboDocument2 pagesPeta Pasien Orthopaedi Sabtu, 1 Agustus 2015 Soe/Fdl/Arv/Hdd/Cid/Dli/Dak/Mad/Asd/Git/Aip/Gas/Ady/Adh/Via/Ewi/Har/Dim/HboRhomadhoni Ika PutraNo ratings yet
- Maping Bayangan 7 Maret 2016Document1 pageMaping Bayangan 7 Maret 2016Rhomadhoni Ika PutraNo ratings yet
- Basic Instruments For Screw Plate Fixation FinalDocument35 pagesBasic Instruments For Screw Plate Fixation FinalRhomadhoni Ika Putra100% (2)
- Other Suggested Resources: Cambridge IGCSE History (9-1) (0977)Document6 pagesOther Suggested Resources: Cambridge IGCSE History (9-1) (0977)Mc MurdoNo ratings yet
- Flat Earth Mythology and Fact (Biblical Astronomer, No. 94, 2000)Document8 pagesFlat Earth Mythology and Fact (Biblical Astronomer, No. 94, 2000)tjmigoto@hotmail.comNo ratings yet
- 2F MOLINA Physical AssessmentDocument12 pages2F MOLINA Physical AssessmentAngela Del CastilloNo ratings yet
- Tata Communications Transformation Services Limited Vs ACIT Bombay High CourtDocument3 pagesTata Communications Transformation Services Limited Vs ACIT Bombay High CourtRAMODSNo ratings yet
- Top 5 Customer ComplaintsDocument2 pagesTop 5 Customer ComplaintsNasir BukhariNo ratings yet
- Lecture No. 8 Systems Approach To ManagementDocument3 pagesLecture No. 8 Systems Approach To ManagementSehar IrfanNo ratings yet
- Child in Conflict With LawDocument3 pagesChild in Conflict With LawNamoAmitofou100% (2)
- UMT TriboLab Mechanical Tester and Tribometer-B1002 RevA2-Brochure PDFDocument8 pagesUMT TriboLab Mechanical Tester and Tribometer-B1002 RevA2-Brochure PDFcatalineuuNo ratings yet
- Lopez Vs Pan American World AirwaysDocument2 pagesLopez Vs Pan American World AirwaysMark Gabriel B. MarangaNo ratings yet
- The Ponchos CaseDocument4 pagesThe Ponchos CaseIsha AgrawalNo ratings yet
- CSULA Spring 2016 MGMT 308 SyllabusDocument5 pagesCSULA Spring 2016 MGMT 308 SyllabusAnonymous Wl8qW1No ratings yet
- Spiritual GiftDocument3 pagesSpiritual Giftharry misaoNo ratings yet
- Quality AssessmentDocument38 pagesQuality AssessmentIgnacioNo ratings yet
- Guide Investigator HandbookDocument45 pagesGuide Investigator HandbookCompaq Presario0% (1)
- Height Balanced Trees: Laboratory Module 4Document12 pagesHeight Balanced Trees: Laboratory Module 4ZafarIqbalNo ratings yet
- True Worship by W. WiersbeDocument4 pagesTrue Worship by W. WiersbeJack Nikholas100% (2)
- How To Make A Detailed OutlineDocument8 pagesHow To Make A Detailed OutlineIvan Clark PalabaoNo ratings yet
- Intro To Human Computer InteractionDocument53 pagesIntro To Human Computer InteractionKanit WongsuphasasawatNo ratings yet
- DruidDocument24 pagesDruidשובל לויNo ratings yet
- TEDx Speech Script - Hannah Pham - INSDocument4 pagesTEDx Speech Script - Hannah Pham - INSHan Thai Pham (Hannah)No ratings yet
- MBA Syllabus 2013Document60 pagesMBA Syllabus 2013carthik19No ratings yet
- Employee Commitment On Organizational Performance: K.Princy, E.RebekaDocument5 pagesEmployee Commitment On Organizational Performance: K.Princy, E.RebekaEBO The InspirationistNo ratings yet
- Verse (82:1) - Word by Word: Quranic Arabic CorpusDocument12 pagesVerse (82:1) - Word by Word: Quranic Arabic CorpusaminchatNo ratings yet
- (BATCH-2018-20) : Chetan Dattaji Gaikwad Institude of Management Studies, PuneDocument8 pages(BATCH-2018-20) : Chetan Dattaji Gaikwad Institude of Management Studies, PuneRubina MansooriNo ratings yet
- Basic Calculus - Q2 - Week 1 - 4Document65 pagesBasic Calculus - Q2 - Week 1 - 4Venice Gwyn ChavezNo ratings yet
- Mareting in Digital World PresentationDocument34 pagesMareting in Digital World PresentationFeroj AhmedNo ratings yet
- 7346326Document41 pages7346326syafik.uitmNo ratings yet
- EULAR Recommendations For The Role of The Nurse in Management of Chronic Inflammatory ArthritisDocument19 pagesEULAR Recommendations For The Role of The Nurse in Management of Chronic Inflammatory ArthritisRendra RafiNo ratings yet