Download as doc or pdf
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Coaching The Tkatchev On Uneven BarsDocument5 pagesCoaching The Tkatchev On Uneven BarsValentin UzunovNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Kinematic Analysis of The Centre of Mass in The Back Handspring: A Case StudyDocument11 pagesKinematic Analysis of The Centre of Mass in The Back Handspring: A Case StudyValentin UzunovNo ratings yet
- Ssangyong Rodius ABSDocument9 pagesSsangyong Rodius ABSMTK2016No ratings yet
- Sandra Brown Ostateca Lui HawkDocument22 pagesSandra Brown Ostateca Lui HawkAdel ChaabaneNo ratings yet
- Patrick Meyer Reliability Understanding Statistics 2010Document160 pagesPatrick Meyer Reliability Understanding Statistics 2010jcgueinj100% (1)
- Developing The Straddle-Sit Press To HandstandDocument5 pagesDeveloping The Straddle-Sit Press To HandstandValentin Uzunov100% (2)
- Teaching Great Yurchenko Layout VaultsDocument10 pagesTeaching Great Yurchenko Layout VaultsValentin Uzunov100% (2)
- Does Kre-Alkalyn® Have Benefits in The Training of Gymnastics Strength Skills?Document7 pagesDoes Kre-Alkalyn® Have Benefits in The Training of Gymnastics Strength Skills?Valentin UzunovNo ratings yet
- Sprint Training For Vault - Off-Season Training Program For 7-12yr Old GymnastsDocument13 pagesSprint Training For Vault - Off-Season Training Program For 7-12yr Old GymnastsValentin UzunovNo ratings yet
- Qualitative Description of The Ideal Yurchenko Layout Vault TechniqueDocument6 pagesQualitative Description of The Ideal Yurchenko Layout Vault TechniqueValentin UzunovNo ratings yet
- Using The "Understand Teach" Model To Coach A Double Layout Dismount of The Asymmetrical BarsDocument5 pagesUsing The "Understand Teach" Model To Coach A Double Layout Dismount of The Asymmetrical BarsValentin UzunovNo ratings yet
- Understanding and Teaching Competitive Gymnastics Skill: The Understand - Teach ModelDocument4 pagesUnderstanding and Teaching Competitive Gymnastics Skill: The Understand - Teach ModelValentin UzunovNo ratings yet
- Stretching Scientifically Myths Facts The Science Part IDocument5 pagesStretching Scientifically Myths Facts The Science Part IValentin Uzunov100% (2)
- Ideological Approach To Coach The Handspring VaultDocument7 pagesIdeological Approach To Coach The Handspring VaultValentin Uzunov100% (1)
- Developing The Straight Body Cast To HandstandDocument6 pagesDeveloping The Straight Body Cast To HandstandValentin Uzunov100% (1)
- Coaching To The Learning StylesDocument5 pagesCoaching To The Learning StylesValentin Uzunov100% (1)
- Coaching and The Ringelmann EffectDocument4 pagesCoaching and The Ringelmann EffectValentin Uzunov100% (4)
- How To Teach A Freehip Circle To HandstandDocument3 pagesHow To Teach A Freehip Circle To HandstandValentin UzunovNo ratings yet
- Ecclesiastes 7.1-14 QuestionsDocument2 pagesEcclesiastes 7.1-14 QuestionsSamuel XiaoNo ratings yet
- A Complete Guide For Physics: Gscience Classes Practice SetDocument2 pagesA Complete Guide For Physics: Gscience Classes Practice SetWillis ChekovNo ratings yet
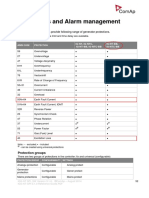
- Pages From IGS-NT-SPI-3.1.0 Reference Guide2Document1 pagePages From IGS-NT-SPI-3.1.0 Reference Guide2Mohamed MossadNo ratings yet
- Review Film-WPS OfficeDocument2 pagesReview Film-WPS OfficeSemprul BotNo ratings yet
- DNS Log Message Reference PDFDocument123 pagesDNS Log Message Reference PDFRam KumarNo ratings yet
- Installation and User's Guide: IBM Tivoli Storage Manager For Windows Backup-Archive ClientsDocument800 pagesInstallation and User's Guide: IBM Tivoli Storage Manager For Windows Backup-Archive ClientsJavier GonzalezNo ratings yet
- Sexual Vs Asexual Reproduction Worksheet-1Document3 pagesSexual Vs Asexual Reproduction Worksheet-1Deandre YoungNo ratings yet
- Series 800M4QT Specification SheetDocument4 pagesSeries 800M4QT Specification SheetWattsNo ratings yet
- Serveraid M5014/M5015 Sas/Sata Controllers: User'S GuideDocument92 pagesServeraid M5014/M5015 Sas/Sata Controllers: User'S GuideAntonNo ratings yet
- Jesusyouth Jesusyouth: Built On The RockDocument16 pagesJesusyouth Jesusyouth: Built On The Rockjyjc_adm100% (1)
- How To Produce Your Book With Scribus.: Make The Front MatterDocument3 pagesHow To Produce Your Book With Scribus.: Make The Front MattersudyNo ratings yet
- Law of Motion Final PDFDocument32 pagesLaw of Motion Final PDFMark RosalesNo ratings yet
- Crop Improvement of WheatDocument24 pagesCrop Improvement of WheatRabeesh VermaNo ratings yet
- Astm F2882F2882M-17Document7 pagesAstm F2882F2882M-17Gabriel Perez CruzNo ratings yet
- Sim 600Document1 pageSim 600Lupu ValentinNo ratings yet
- BNS - Module 2 - JamerDocument6 pagesBNS - Module 2 - JamerRenzo JamerNo ratings yet
- Problem StatementDocument23 pagesProblem Statementpandem soniyaNo ratings yet
- CH 35Document73 pagesCH 35api-234521500100% (1)
- Edu 105 H3Document3 pagesEdu 105 H3Michaella DometitaNo ratings yet
- Ila ResumeDocument2 pagesIla ResumeAravind SampathNo ratings yet
- Business Guide 2020Document68 pagesBusiness Guide 2020Elenca KyweNo ratings yet
- Project Report On DYEING OF FabricsDocument2 pagesProject Report On DYEING OF FabricsChasity ColeNo ratings yet
- 4l60e Manual Shift ConversionDocument10 pages4l60e Manual Shift ConversionSalvador PinedaNo ratings yet
- FRENCH JSS2 Second Term ExamDocument5 pagesFRENCH JSS2 Second Term ExamchrizyboyziNo ratings yet
- AHT Scan PodDocument6 pagesAHT Scan PodRyanRRNo ratings yet
- AssertivenessDocument97 pagesAssertivenessHemantNo ratings yet
- Human CommunicationDocument13 pagesHuman Communicationbeyouty suitsNo ratings yet