Download as docx, pdf, or txt
You might also like
- Sample Asset Handover FormDocument1 pageSample Asset Handover FormApartmenti Tanzania100% (2)
- Luovutuskirja Ajoneuvon Vesikulkuneuvon Omistusoikeuden Siirrosta B124eDocument2 pagesLuovutuskirja Ajoneuvon Vesikulkuneuvon Omistusoikeuden Siirrosta B124eAirsoftNo ratings yet
- Reimbursement Claim FormDocument2 pagesReimbursement Claim FormG. Prabha karanNo ratings yet
- Reimbursement FormDocument2 pagesReimbursement FormVaibhavNo ratings yet
- DAGS Travel Order September 2023-Pick-Up I-BEAMSDocument8 pagesDAGS Travel Order September 2023-Pick-Up I-BEAMSFrancis Danver EmerzNo ratings yet
- Conveyance Claim Form Conveyance Claim FormDocument1 pageConveyance Claim Form Conveyance Claim FormmeghadurganNo ratings yet
- DAGS Travel Order For October 2022Document2 pagesDAGS Travel Order For October 2022Francis Danver EmerzNo ratings yet
- Expenses Voucher BillsDocument1 pageExpenses Voucher Billsguptaprabha951No ratings yet
- Payment Application Form: No Fill In Name Dpt/项目PgmDocument5 pagesPayment Application Form: No Fill In Name Dpt/项目PgmGomathyselviNo ratings yet
- Expenses Voucher BillsDocument1 pageExpenses Voucher Billsguptaprabha951No ratings yet
- DAGS TRAVEL ORDER For OCTOBER 2023 - Attend Bidding in DA Regional OfficeDocument2 pagesDAGS TRAVEL ORDER For OCTOBER 2023 - Attend Bidding in DA Regional OfficeFrancis Danver EmerzNo ratings yet
- Monthly Vehicle Use RPT - Fuel Card Trans LogDocument4 pagesMonthly Vehicle Use RPT - Fuel Card Trans LogAhmed SayedNo ratings yet
- Letter Credit Application Form ModelDocument4 pagesLetter Credit Application Form ModelMelissa ReNo ratings yet
- United India Motor Commercial Proposal From PDFDocument2 pagesUnited India Motor Commercial Proposal From PDFRajeev SinghNo ratings yet
- Employee Gate Pass Form - ABC - OBDocument1 pageEmployee Gate Pass Form - ABC - OBFOODMNL Accounting100% (1)
- KrisFlyer Miles FormDocument2 pagesKrisFlyer Miles FormCatur AnugerahNo ratings yet
- SSD - New Travel AuthorisationDocument1 pageSSD - New Travel AuthorisationDengAwutNo ratings yet
- Expenses Claim For Outstation TripDocument2 pagesExpenses Claim For Outstation TripChandru ChristurajNo ratings yet
- TM06-GAS-021-001 - Company - Transport - Information - Arrangement (1) - Rev 04 - 23.7.2019Document1 pageTM06-GAS-021-001 - Company - Transport - Information - Arrangement (1) - Rev 04 - 23.7.2019zenel nadyaNo ratings yet
- Department of State Growth: Application For RegistrationDocument1 pageDepartment of State Growth: Application For Registrationdibesh dhakalNo ratings yet
- MRO Accreditation MC186 - For PostingDocument5 pagesMRO Accreditation MC186 - For PostingNairdna P Led OirasorNo ratings yet
- Monthly Vehicle Use RPT - Fuel Card Trans LogDocument8 pagesMonthly Vehicle Use RPT - Fuel Card Trans LogPakistan Tourism OfficialNo ratings yet
- Annexure IV - Travel Expense Claim FormDocument3 pagesAnnexure IV - Travel Expense Claim FormKeshav ShankarNo ratings yet
- Cargo Booking Vendor FormDocument3 pagesCargo Booking Vendor FormjeklinNo ratings yet
- Consignment Form: Office Use (Firefly Express Tracking Number)Document4 pagesConsignment Form: Office Use (Firefly Express Tracking Number)PROSURVEY STUDIONo ratings yet
- Windscreen Claim FormDocument1 pageWindscreen Claim FormHihiNo ratings yet
- Welcome To AutoCheck - Full ReportDocument3 pagesWelcome To AutoCheck - Full ReportOnur BayramovNo ratings yet
- F3529 CFDDocument1 pageF3529 CFDjmvuletichNo ratings yet
- Application Design: Amit Dalal Gulu Gulu Tour and Travels Pvt. Ltd. 1/1/2020Document7 pagesApplication Design: Amit Dalal Gulu Gulu Tour and Travels Pvt. Ltd. 1/1/2020AMITNo ratings yet
- BER-TRF-21-025 - KZ SignedDocument2 pagesBER-TRF-21-025 - KZ SignedMohd NasrullahNo ratings yet
- 8588 (1) - MergedDocument11 pages8588 (1) - MergedAli AlahmaNo ratings yet
- AppyDocument2 pagesAppyAngus 鄧雋杰 TangNo ratings yet
- Ta FormDocument1 pageTa FormShiva ThakurNo ratings yet
- Toledo City ApplicationDocument1 pageToledo City Applicationsass23No ratings yet
- Ventas FlujogrammaDocument1 pageVentas FlujogrammaHenry CarrilloNo ratings yet
- QR TEN 10000 01-00-27 Complaint Request FormDocument2 pagesQR TEN 10000 01-00-27 Complaint Request Formasiaperdana.umumNo ratings yet
- Vehicle Service / Repair Requisition Form: Normal / Routine Service Major (Estimated Above RM3,000.00)Document1 pageVehicle Service / Repair Requisition Form: Normal / Routine Service Major (Estimated Above RM3,000.00)Wang Khong HweeNo ratings yet
- De-4-Drydock Defect FormDocument3 pagesDe-4-Drydock Defect Formmaxuya2001No ratings yet
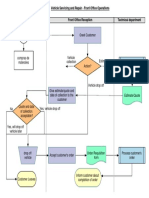
- Vehicle Servicing and Repair - Front Office OperationsDocument1 pageVehicle Servicing and Repair - Front Office OperationsHenry CarrilloNo ratings yet
- LBU F VL MR9 VehicleTransfer PDFDocument4 pagesLBU F VL MR9 VehicleTransfer PDFRama Moorthy JeelagaNo ratings yet
- Taxi Auto ReceiptDocument1 pageTaxi Auto ReceiptShrikant MehtaNo ratings yet
- Final Job Card CGCDocument2 pagesFinal Job Card CGCAnwar HariryNo ratings yet
- Application For Airside Vehicle Operators PermitDocument2 pagesApplication For Airside Vehicle Operators Permitt59t2c9qf5No ratings yet
- Expenses FormatDocument1 pageExpenses Formatamit pokharelNo ratings yet
- Premium Freight Monitoirng RecordDocument1 pagePremium Freight Monitoirng RecordRamNo ratings yet
- Premium Freight Monitoirng RecordDocument1 pagePremium Freight Monitoirng RecordRamNo ratings yet
- Dispute / Adjustment Notification / Authorization Form: Manila International Airport AuthorityDocument1 pageDispute / Adjustment Notification / Authorization Form: Manila International Airport AuthorityJoanna Marie CastilloNo ratings yet
- Travel Expenses and Allowance Claim Form PDFDocument2 pagesTravel Expenses and Allowance Claim Form PDFibrahim holidaysNo ratings yet
- Travel Expenses and Allowance Claim FormDocument2 pagesTravel Expenses and Allowance Claim Formibrahim holidaysNo ratings yet
- F3529 CFDDocument2 pagesF3529 CFDinfo.brisbanea1trailersNo ratings yet
- Certificate of Assessed ProjectsDocument1 pageCertificate of Assessed ProjectsLouie MacniNo ratings yet
- Calculation Sheet For TADA AdvanceDocument1 pageCalculation Sheet For TADA AdvanceWaseem khan kakarNo ratings yet
- Bid Taxi 0 Ahbo@bis - Gov.inDocument13 pagesBid Taxi 0 Ahbo@bis - Gov.inChehar EnterprisesNo ratings yet
- ExxonMobil Reimbursement FormDocument2 pagesExxonMobil Reimbursement FormPrem BindNo ratings yet
- FORM-24 Detail Article RtoDocument3 pagesFORM-24 Detail Article RtoSUNNY MANOJ RAJPUTNo ratings yet
- My Docs Shipping InstructionDocument1 pageMy Docs Shipping InstructionGokulganth ThirumalNo ratings yet
- Asean Trade in Goods Agreement Asean Industrial Cooperation Scheme Certificate of Origin (Combined Declaration and Certificate) Form DDocument1 pageAsean Trade in Goods Agreement Asean Industrial Cooperation Scheme Certificate of Origin (Combined Declaration and Certificate) Form DAndrew NatanaelNo ratings yet