Download as pdf or txt
You might also like
- Prioritize NCPDocument19 pagesPrioritize NCPzey young94% (34)
- 2 Series CPTDocument7 pages2 Series CPTRenuka bhaskarNo ratings yet
- Second TrimesterDocument11 pagesSecond Trimestermardsz100% (2)
- Chant A Chae NG 2011Document4 pagesChant A Chae NG 2011Eva YustianaNo ratings yet
- A Young Child With Recurrent Pneumonia and HemoptyDocument4 pagesA Young Child With Recurrent Pneumonia and Hemoptylincolnbasilio1No ratings yet
- Liam 1994Document1 pageLiam 1994eric.r.c1701No ratings yet
- Kurtz 2016Document5 pagesKurtz 2016Stevano PattiasinaNo ratings yet
- Ahmed 2021 Lung Us in PTBDocument5 pagesAhmed 2021 Lung Us in PTBmarvic gabitanNo ratings yet
- Journal ReadingDocument17 pagesJournal ReadingintanrhamaNo ratings yet
- Smolen Et Al 2018 Non Invasive Evaluation of A Liver Mass in A Patient Post SplenectomyDocument5 pagesSmolen Et Al 2018 Non Invasive Evaluation of A Liver Mass in A Patient Post SplenectomyPanagiotis SouldatosNo ratings yet
- Laparoscopic RepairDocument3 pagesLaparoscopic RepairDominique WilsonNo ratings yet
- Eyelid TattoingDocument15 pagesEyelid Tattoing小島隆司No ratings yet
- Congenital Bronchopulmonary Foregut Malformation: Systematic Review of The LiteratureDocument7 pagesCongenital Bronchopulmonary Foregut Malformation: Systematic Review of The LiteraturemikeNo ratings yet
- Kartagener Syndrome: A Not So Rare Phenomenon: Original ArticleDocument4 pagesKartagener Syndrome: A Not So Rare Phenomenon: Original ArticleAlfeus GradyNo ratings yet
- Surgical Case Report 2022 Mesoth PerithDocument3 pagesSurgical Case Report 2022 Mesoth PerithJeanne LahogueNo ratings yet
- 1752 1947 2 309 PDFDocument5 pages1752 1947 2 309 PDFHelen EngelinaNo ratings yet
- Symptomatic Lymphangioma of The Adrenal Gland: A Case ReportDocument3 pagesSymptomatic Lymphangioma of The Adrenal Gland: A Case Reportjulio perezNo ratings yet
- Transfusion Related Acute Lung Injury After Cesarean Section in A Patient With HELLP SyndromeDocument4 pagesTransfusion Related Acute Lung Injury After Cesarean Section in A Patient With HELLP SyndromeBayu Surya DanaNo ratings yet
- A 56 Year Old Woman With Multiple Pulmonary CystsDocument8 pagesA 56 Year Old Woman With Multiple Pulmonary CystsAchmad Dodi MeidiantoNo ratings yet
- Chilaiditi Syndrome - A Benign Air Under DiaphragmDocument1 pageChilaiditi Syndrome - A Benign Air Under DiaphragmBaran PalanimuthuNo ratings yet
- Non Small-Cell Lung Cancer in A 15-Year-Old NonsmokerDocument2 pagesNon Small-Cell Lung Cancer in A 15-Year-Old Nonsmokertonirian99No ratings yet
- Primary Carcinoma of Fallopian Tube: Case Series Case ReportDocument4 pagesPrimary Carcinoma of Fallopian Tube: Case Series Case ReportChi NgôNo ratings yet
- Pathology BDocument5 pagesPathology Bttdjhg2p6kNo ratings yet
- A Rare Case of Paediatric Lung Tumor: Pleuropulmonary Blastoma (Type-1 PPB)Document1 pageA Rare Case of Paediatric Lung Tumor: Pleuropulmonary Blastoma (Type-1 PPB)Javed AliNo ratings yet
- Pulmonary and Mediastinal Bronchogenic Cysts Clinicopathologic Study of 33 CaseDocument7 pagesPulmonary and Mediastinal Bronchogenic Cysts Clinicopathologic Study of 33 CaseDr AmalNo ratings yet
- Adult Intussusception - A Surgical Dilemma: J Ayub Med Coll Abbottabad 2006 18Document4 pagesAdult Intussusception - A Surgical Dilemma: J Ayub Med Coll Abbottabad 2006 18edi_wsNo ratings yet
- Case 1: Recurrent Pneumonia in A 15-Year-Old Girl: Article Figures & Data Info & Metrics CommentsDocument7 pagesCase 1: Recurrent Pneumonia in A 15-Year-Old Girl: Article Figures & Data Info & Metrics CommentsJoshua MendozaNo ratings yet
- s2044 Hemorrhoid or Cancer Anorectal Mucosal.2044Document1 pages2044 Hemorrhoid or Cancer Anorectal Mucosal.2044kiki tuanaya1No ratings yet
- Article Endobronchial TuberculosisDocument4 pagesArticle Endobronchial TuberculosisFaruqi clinic OfficialNo ratings yet
- Raut 2018Document4 pagesRaut 2018nesrine ninaNo ratings yet
- A 56 Year Old Man With Chronic Cough, HemoptysisDocument4 pagesA 56 Year Old Man With Chronic Cough, HemoptysisagamerocallejasNo ratings yet
- LungDocument5 pagesLungWafa MediNo ratings yet
- Dematos 1997Document6 pagesDematos 1997Ali AmokraneNo ratings yet
- Tuberculosis Masquerading As Recurrent Metastatic Carcinoma of The CervixDocument2 pagesTuberculosis Masquerading As Recurrent Metastatic Carcinoma of The Cervixpaijosuseno2242No ratings yet
- Clinical Case Reports - 2024 - Gyawali - Prune Belly Syndrome A Rare Case ReportDocument4 pagesClinical Case Reports - 2024 - Gyawali - Prune Belly Syndrome A Rare Case Reportoscarlicona25No ratings yet
- Late Presentation of Bochdalek Hernia: Clinical and Radiological AspectsDocument5 pagesLate Presentation of Bochdalek Hernia: Clinical and Radiological AspectsNelly NehNo ratings yet
- Aydin Et Al 2011 A Case of Uncontrolled AsthmaDocument5 pagesAydin Et Al 2011 A Case of Uncontrolled AsthmadvbhodhanaNo ratings yet
- Coexistence of Primary Thyroid Diffuse Large B Cell Lymphoma and Papillary Thyroid Carcinoma: A Case Report and Literature ReviewDocument5 pagesCoexistence of Primary Thyroid Diffuse Large B Cell Lymphoma and Papillary Thyroid Carcinoma: A Case Report and Literature ReviewFathkaHanifAbimanyuNo ratings yet
- Coexistence of Primary Thyroid Diffuse Large B Cell Lymphoma and Papillary Thyroid Carcinoma: A Case Report and Literature ReviewDocument5 pagesCoexistence of Primary Thyroid Diffuse Large B Cell Lymphoma and Papillary Thyroid Carcinoma: A Case Report and Literature ReviewFathkaHanifAbimanyuNo ratings yet
- A Case of Pulmonary Aspergilloma and ActinomycosisDocument4 pagesA Case of Pulmonary Aspergilloma and ActinomycosisNova PurbaNo ratings yet
- The Role of High-Resolution Chest CT in The Diagnosis of Neuroendocrine Cell Hyperplasia of Infancy - A Rare Form of Pediatric Interstitial Lung DiseaseDocument3 pagesThe Role of High-Resolution Chest CT in The Diagnosis of Neuroendocrine Cell Hyperplasia of Infancy - A Rare Form of Pediatric Interstitial Lung DiseaseWalid AissaNo ratings yet
- Seear 2017Document8 pagesSeear 2017Lucia NiculaeNo ratings yet
- Malignant Mesothelioma Presenting With Unexplained Recurrent Pleurisy EpisodesDocument4 pagesMalignant Mesothelioma Presenting With Unexplained Recurrent Pleurisy EpisodesNurul NingrumNo ratings yet
- Clearing The Air - A Conservative Option For Spontaneous PneumothoraxDocument2 pagesClearing The Air - A Conservative Option For Spontaneous PneumothoraxDivara SyautaNo ratings yet
- Ultrasonography: A Cost - Effective Modality For Diagnosis of Rib Tuberculosis - A Case ReportDocument3 pagesUltrasonography: A Cost - Effective Modality For Diagnosis of Rib Tuberculosis - A Case ReportAdvanced Research PublicationsNo ratings yet
- PIIS0012369215421269Document2 pagesPIIS0012369215421269chicyNo ratings yet
- Chylothorax-Literature Review and Two Rare CasesDocument5 pagesChylothorax-Literature Review and Two Rare CasesdrAlbertoVVNo ratings yet
- Case Report: Streptococcus AnginosusDocument4 pagesCase Report: Streptococcus AnginosusIesanu MaraNo ratings yet
- Radiographic Diagnosis of Hyaline Membrane Disease'Document5 pagesRadiographic Diagnosis of Hyaline Membrane Disease'Sekar MentariNo ratings yet
- A Case Report of Perforated Primary Follicular Lymphoma of The Jejunum Presenting As Aneurismal FormDocument3 pagesA Case Report of Perforated Primary Follicular Lymphoma of The Jejunum Presenting As Aneurismal FormPeertechz Publications Inc.No ratings yet
- Chilaiditi Syndrom in Child Diagnostic Trap (Case Report)Document6 pagesChilaiditi Syndrom in Child Diagnostic Trap (Case Report)IJAR JOURNALNo ratings yet
- 5 - Hung, 2004Document4 pages5 - Hung, 2004Henrique MachadoNo ratings yet
- Patient Record (Surgical Thyroid)Document2 pagesPatient Record (Surgical Thyroid)Crystine DavidsonNo ratings yet
- Clinical ParasitologyDocument17 pagesClinical ParasitologyMariann EstoqueNo ratings yet
- Case report-PALDocument5 pagesCase report-PALHeshan SiriwardenaNo ratings yet
- Stomach, Ened, Endino, Rib, Crushed, Hiatus, Life,: 5) - Symptoms Symptoms PermanentDocument4 pagesStomach, Ened, Endino, Rib, Crushed, Hiatus, Life,: 5) - Symptoms Symptoms PermanentayuNo ratings yet
- A Rare Case of Carcinoma of Unknown Primary in AnDocument2 pagesA Rare Case of Carcinoma of Unknown Primary in AnMax FaxNo ratings yet
- Nonresolving PF SarcoidosisDocument6 pagesNonresolving PF SarcoidosisJeansDaquinagNo ratings yet
- Ma1 Ignan Duodenocol Ic Fistulas: A Case Report and Review of The LiteratureDocument4 pagesMa1 Ignan Duodenocol Ic Fistulas: A Case Report and Review of The LiteratureJoy GhoseNo ratings yet
- E248048 FullDocument3 pagesE248048 FullsilviaNo ratings yet
- Jurnal BedahDocument3 pagesJurnal BedahAb Hakim MuslimNo ratings yet
- Pleuropulmonary BlastomaDocument8 pagesPleuropulmonary BlastomaAdriana RuizNo ratings yet
- Thoracic Endoscopy: Advances in Interventional PulmonologyFrom EverandThoracic Endoscopy: Advances in Interventional PulmonologyMichael J. SimoffNo ratings yet
- @anesthesia Books 2016 Oxford TextbookDocument1,016 pages@anesthesia Books 2016 Oxford TextbookAnny VelásquezNo ratings yet
- Modified by Garnavos Milch Vs Kocher Technique For Anterior Shoulder DislocationDocument9 pagesModified by Garnavos Milch Vs Kocher Technique For Anterior Shoulder DislocationNick LasanianosNo ratings yet
- Kenya ARV Guidelines 2022 - 230105 - 142032Document287 pagesKenya ARV Guidelines 2022 - 230105 - 142032islam media100% (1)
- Nejmra 2032506Document15 pagesNejmra 2032506subha95No ratings yet
- Spinal Cord Injury Without Radiological AbnormalitDocument3 pagesSpinal Cord Injury Without Radiological Abnormalitcollestein christdianNo ratings yet
- Andre Surgery Notes (Ed 3, 2013) W Washington+ChinYeeDocument155 pagesAndre Surgery Notes (Ed 3, 2013) W Washington+ChinYeeDaniel Lim100% (3)
- Dalman 222Document7 pagesDalman 222Cyril D. SuazoNo ratings yet
- Hyderabad: Cortico-Basal Implantology CourseDocument6 pagesHyderabad: Cortico-Basal Implantology CourseYousuf AdamNo ratings yet
- EAP FormDocument2 pagesEAP FormRebecca LuiNo ratings yet
- Syndarogya Proposal Form: Synbk Code Bic Code 9 2 1 0 0 0Document2 pagesSyndarogya Proposal Form: Synbk Code Bic Code 9 2 1 0 0 0Akhil ShastryNo ratings yet
- 10 Besar Penyakit November 2017Document53 pages10 Besar Penyakit November 2017dartosNo ratings yet
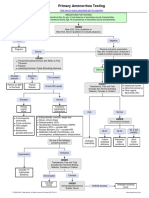
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- Z. J. Lipowski (Auth.), P. Pichot, P. Berner, R. Wolf, K. Thau (Eds.) - Biological Psychiatry, Higher Nervous Activity-Springer US (1985)Document928 pagesZ. J. Lipowski (Auth.), P. Pichot, P. Berner, R. Wolf, K. Thau (Eds.) - Biological Psychiatry, Higher Nervous Activity-Springer US (1985)cc vereNo ratings yet
- Cosmetic AcupunctureDocument3 pagesCosmetic Acupuncturejanachidambaram100% (1)
- Neumonía Adquirida en La Comunidad en Niños - Tratamiento Ambulatorio - UpToDateDocument32 pagesNeumonía Adquirida en La Comunidad en Niños - Tratamiento Ambulatorio - UpToDatepao.pearanda1998No ratings yet
- Dispelling The Malaria-Typhoid Co-Infection Myth in Nigeria. A Literature ReviewDocument8 pagesDispelling The Malaria-Typhoid Co-Infection Myth in Nigeria. A Literature Reviewwaleola25No ratings yet
- Links para Baixar Livros VeterináriosDocument14 pagesLinks para Baixar Livros VeterináriosBrunaFernandes33% (9)
- 2015 - Nursing Students' Experiences of and Satisfaction With The Clinical Learning EnvironmentDocument12 pages2015 - Nursing Students' Experiences of and Satisfaction With The Clinical Learning EnvironmentDaniel Andres Rincon AlvarezNo ratings yet
- MCQ 3rd LevelDocument19 pagesMCQ 3rd LevelislamNo ratings yet
- Health: Quarter 1 - Module 1Document11 pagesHealth: Quarter 1 - Module 1TIPAY, EMELIE L.No ratings yet
- SWOT AnalysisDocument48 pagesSWOT Analysisprasanna lamaNo ratings yet
- Three Treasures Correspondences BrochureDocument4 pagesThree Treasures Correspondences Brochure292293709No ratings yet
- Exoplan Supported Libraries @exocadDocument65 pagesExoplan Supported Libraries @exocadRaffa MarquesNo ratings yet
- Japan Medical Device Reimbursement PolicyDocument26 pagesJapan Medical Device Reimbursement Policyanimeshsarkar87No ratings yet
- What Living As A Resident Can Teach Long-Term Care Staff: The Power of Empathy To Transform Care (Excerpt)Document14 pagesWhat Living As A Resident Can Teach Long-Term Care Staff: The Power of Empathy To Transform Care (Excerpt)Health Professions Press, an imprint of Paul H. Brookes Publishing Co., Inc.No ratings yet
- NCM 112 TH (12F)Document24 pagesNCM 112 TH (12F)Justine April YbanezNo ratings yet
- Diagnostic Test For TBDocument78 pagesDiagnostic Test For TBSumesh ShresthaNo ratings yet