
Yang 2018
Yang 2018
You might also like
- 1.pharmacy Technician Study GuideDocument31 pages1.pharmacy Technician Study GuideAlan Hao93% (14)
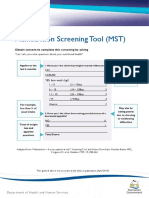
- Malnutrition Screening Tool (MST) : Obtain Consent To Complete This Screening by AskingDocument2 pagesMalnutrition Screening Tool (MST) : Obtain Consent To Complete This Screening by AskingAku dienaNo ratings yet
- Paul E. Steiner - Okinawa and Its People (I)Document10 pagesPaul E. Steiner - Okinawa and Its People (I)José Luis IgueNo ratings yet
- Evaluation of A New Model of Hind Limb Ischemia in Rabbit: and Paris, FranceDocument9 pagesEvaluation of A New Model of Hind Limb Ischemia in Rabbit: and Paris, FranceKharina AreeistyNo ratings yet
- Angiosome-Targeted Infrapopliteal EndovascularDocument9 pagesAngiosome-Targeted Infrapopliteal EndovascularPablo BoadaNo ratings yet
- Two-Stage Bone Lengthening With Reuse of A Single Intramedullary Telescopic Nail in Patients With AchondroplasiaDocument7 pagesTwo-Stage Bone Lengthening With Reuse of A Single Intramedullary Telescopic Nail in Patients With AchondroplasiaLizza Mora RNo ratings yet
- Total Calcanectomy For The Treatment of Calcaneal OsteomyelitisDocument4 pagesTotal Calcanectomy For The Treatment of Calcaneal OsteomyelitisCleff FlowersNo ratings yet
- Accepted Manuscript: Seminars in Vascular SurgeryDocument33 pagesAccepted Manuscript: Seminars in Vascular SurgeryAnis BergerNo ratings yet
- PRGF in Chronic Ulcers - Diabetic Foot UlcersDocument5 pagesPRGF in Chronic Ulcers - Diabetic Foot UlcersVikram ReddyNo ratings yet
- Surgical Treatment of Plantar First Metatarsal UlcerationsDocument8 pagesSurgical Treatment of Plantar First Metatarsal UlcerationsDalid Raul Nieto ZepedaNo ratings yet
- Calcanectomy For OsteomyelitisDocument7 pagesCalcanectomy For OsteomyelitisCleff FlowersNo ratings yet
- Is It Safe To Extract The Reverse Sural Artery Flap From The Proximal Third of The Leg?Document7 pagesIs It Safe To Extract The Reverse Sural Artery Flap From The Proximal Third of The Leg?yennysabriniNo ratings yet
- Elif KI (2021) - Tibiotalocalcaneal Intramedullary Nailing For Unstable Geriatric Ankle FracturesDocument7 pagesElif KI (2021) - Tibiotalocalcaneal Intramedullary Nailing For Unstable Geriatric Ankle FracturesHariom ShuklaNo ratings yet
- Duplex Guided Balloon Angioplasty and Subintimal DDocument8 pagesDuplex Guided Balloon Angioplasty and Subintimal DJose PiulatsNo ratings yet
- SN02Document11 pagesSN02Enrique San NorbertoNo ratings yet
- Advanced Limb Salvage - Pedal Artery InterventionsDocument10 pagesAdvanced Limb Salvage - Pedal Artery Interventionsafso afsoNo ratings yet
- Diabetic Limb Salvage Procedure With Bone Allograft and Free Flap Transfer: A Case ReportDocument9 pagesDiabetic Limb Salvage Procedure With Bone Allograft and Free Flap Transfer: A Case ReportJacob DoughertyNo ratings yet
- 1 s2.0 S0011853211000346 Main PDFDocument6 pages1 s2.0 S0011853211000346 Main PDFMichael XuNo ratings yet
- Complications and Morbidity Associated With Loop Ileostomies in Patients With Ulcerative ColitisDocument5 pagesComplications and Morbidity Associated With Loop Ileostomies in Patients With Ulcerative ColitisNathalia GonzalezNo ratings yet
- Et0420 MedAffairs MouawadDocument5 pagesEt0420 MedAffairs MouawadAna Silvia LebrOnNo ratings yet
- 10 5114@pdia 2016 62415Document6 pages10 5114@pdia 2016 62415senkonenNo ratings yet
- Specific Aspects of Percutaneous Closure of Patent Ductus Arteriosus in Adult PatientsDocument6 pagesSpecific Aspects of Percutaneous Closure of Patent Ductus Arteriosus in Adult PatientsTri RachmadijantoNo ratings yet
- 31MDI RET '17 JacksonDocument6 pages31MDI RET '17 Jacksoncd.brendasotofloresNo ratings yet
- 10 36516-Jocass 1276127-3055931Document5 pages10 36516-Jocass 1276127-3055931yyyyx842No ratings yet
- Modified Extrapleural Ligation of Patent Ductus Arteriosus: A Convenient Surgical Approach in A Developing CountryDocument4 pagesModified Extrapleural Ligation of Patent Ductus Arteriosus: A Convenient Surgical Approach in A Developing CountryHandyka Vb GNo ratings yet
- Reconstruction of Mandible by Free Fibular Flap: Original ArticleDocument5 pagesReconstruction of Mandible by Free Fibular Flap: Original ArticleSani Solihatul FitriNo ratings yet
- The Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionDocument10 pagesThe Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionRobert ChristevenNo ratings yet
- Bovine Digit Surgical TechniqueDocument16 pagesBovine Digit Surgical TechniqueWendyNo ratings yet
- TurkeyGMJ 62 200 enDocument6 pagesTurkeyGMJ 62 200 enCocoNo ratings yet
- Lymphedema Rates in Pedicled ALTP For Coverage in Irradiated Groin Defects 2019Document4 pagesLymphedema Rates in Pedicled ALTP For Coverage in Irradiated Groin Defects 2019yeapdshengNo ratings yet
- Varicose Veins: A Clinical Study: Original Research ArticleDocument5 pagesVaricose Veins: A Clinical Study: Original Research ArticleAndhika DNo ratings yet
- Treatment of Vascular Malformations of The Mandible: A Description of 12 CasesDocument5 pagesTreatment of Vascular Malformations of The Mandible: A Description of 12 CasesneyhaaNo ratings yet
- 1 s2.0 S2214031X20300693 MainDocument6 pages1 s2.0 S2214031X20300693 MainCristhian Jover CastroNo ratings yet
- NAIS Initial PaperDocument10 pagesNAIS Initial Paperjesus Porras ColonNo ratings yet
- Long-Term Outcome After Thrombolysis For Acute Lower Limb IschaemiaDocument9 pagesLong-Term Outcome After Thrombolysis For Acute Lower Limb IschaemiaIdham Adyasa Manggala PutraNo ratings yet
- Sural Island Flap - A Good Option For Coverage of The Exposed Heel (Tendo-Achillis)Document6 pagesSural Island Flap - A Good Option For Coverage of The Exposed Heel (Tendo-Achillis)yennysabriniNo ratings yet
- Monux 2020Document7 pagesMonux 2020dev darma karinggaNo ratings yet
- A Prospective Observational Study On Scola For Ventral Hernia With Diastasis Recti - Our Experience at A Tertiary Care HospitalDocument4 pagesA Prospective Observational Study On Scola For Ventral Hernia With Diastasis Recti - Our Experience at A Tertiary Care HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Use of External Fixation in The Reconstruction of The Charcot Foot and AnkleDocument21 pagesUse of External Fixation in The Reconstruction of The Charcot Foot and AnkleAnonymous kdBDppigENo ratings yet
- 20SPIGCDocument3 pages20SPIGCscribullNo ratings yet
- TRIGONOMETRIADocument7 pagesTRIGONOMETRIACatalina RodríguezNo ratings yet
- The Association Between Skin Blood Flow and Edema On Epidermal Thickness in The Diabetic FootDocument8 pagesThe Association Between Skin Blood Flow and Edema On Epidermal Thickness in The Diabetic FootdeborapkphnNo ratings yet
- Khan 2018Document5 pagesKhan 2018Ivor Wiguna Hartanto WilopoNo ratings yet
- LskjjdshiubifsDocument8 pagesLskjjdshiubifsAchmad Luthfi TiflaniNo ratings yet
- Evolving Approaches To The Iliacs, Femorals, Popliteals, and RenalsDocument12 pagesEvolving Approaches To The Iliacs, Femorals, Popliteals, and RenalsSohil ElfarNo ratings yet
- Efficacyof Vacuum Assisted Closure VACTherapyin Healingof Diabetic Foot Ulcerandafter Diabetic Foot AmputationDocument11 pagesEfficacyof Vacuum Assisted Closure VACTherapyin Healingof Diabetic Foot Ulcerandafter Diabetic Foot AmputationZven BlackNo ratings yet
- Ismaeil 2018Document15 pagesIsmaeil 2018Javier ZaquinaulaNo ratings yet
- Tom Skin-Sparing Approach To Treatemen of NSTI 2016Document14 pagesTom Skin-Sparing Approach To Treatemen of NSTI 2016Sadaf Raisa KhanNo ratings yet
- Bridging Plate Osteosynthesis of Humeral Shaft Fractures: Bruno Livani, William Dias BelangeroDocument9 pagesBridging Plate Osteosynthesis of Humeral Shaft Fractures: Bruno Livani, William Dias BelangeroMiguel Angel Lamas RamirezNo ratings yet
- Elective Frozen Elephant Trunk Procedure Using The E-Vita Open Plus Prosthesis in 94 Patients: A Multicentre French RegistryDocument7 pagesElective Frozen Elephant Trunk Procedure Using The E-Vita Open Plus Prosthesis in 94 Patients: A Multicentre French RegistryrédaNo ratings yet
- Lobular Capillary Hemangioma An Extremely Rare Entity in The Retromolar Region Case ReportDocument5 pagesLobular Capillary Hemangioma An Extremely Rare Entity in The Retromolar Region Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Alogénico Vs AutoóogoDocument4 pagesAlogénico Vs AutoóogoMaximiliano Jara ContrerasNo ratings yet
- Lemus Rangel 2010Document2 pagesLemus Rangel 2010audiNo ratings yet
- FIRST2020Document10 pagesFIRST2020Jeisson Daniel Barrera AlvarezNo ratings yet
- Is Mesh Always Necessary in Every Small UmbilicalDocument8 pagesIs Mesh Always Necessary in Every Small UmbilicalLeonardo RibeiroNo ratings yet
- Management of Anastomotic Leaks After Esophagectomy and Gastric Pull-UpDocument9 pagesManagement of Anastomotic Leaks After Esophagectomy and Gastric Pull-UpSergio Sitta TarquiniNo ratings yet
- The Journal of Foot & Ankle Surgery: Christopher Bibbo, DO, DPM, FACFASDocument5 pagesThe Journal of Foot & Ankle Surgery: Christopher Bibbo, DO, DPM, FACFASdamonenNo ratings yet
- Lee 2015Document7 pagesLee 2015AncaVerdesNo ratings yet
- Ma 2021Document6 pagesMa 2021bigben9262No ratings yet
- Pe Rich On DR It Is of The Auricle and Its ManagementDocument6 pagesPe Rich On DR It Is of The Auricle and Its ManagementmitaNo ratings yet
- Endoscopic Treatment of Choanal Atresia and Use of Balloon Dilation: Our ExperienceDocument6 pagesEndoscopic Treatment of Choanal Atresia and Use of Balloon Dilation: Our Experiencefarah maulida martaNo ratings yet
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementFrom EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementNo ratings yet
- Designing A Breast Abscess Pathway: A Guide For General SurgeonsDocument5 pagesDesigning A Breast Abscess Pathway: A Guide For General SurgeonsRobert ChristevenNo ratings yet
- MC Participant 0Document220 pagesMC Participant 0Robert ChristevenNo ratings yet
- Summary Diagnostic Guidelines PAD CLI Diabetic Foot PerimedDocument38 pagesSummary Diagnostic Guidelines PAD CLI Diabetic Foot PerimedRobert ChristevenNo ratings yet
- Technique: Median Sternotomy - Gold Standard Incision For Cardiac SurgeonsDocument8 pagesTechnique: Median Sternotomy - Gold Standard Incision For Cardiac SurgeonsRobert ChristevenNo ratings yet
- Raza 2017Document7 pagesRaza 2017Robert ChristevenNo ratings yet
- Systems Biology of Gastric Cancer: Perspectives On The Omics-Based Diagnosis and TreatmentDocument8 pagesSystems Biology of Gastric Cancer: Perspectives On The Omics-Based Diagnosis and TreatmentRobert ChristevenNo ratings yet
- The Principles of The Surgical Management of Gastric CancerDocument5 pagesThe Principles of The Surgical Management of Gastric CancerRobert ChristevenNo ratings yet
- Neonatal Intestinal Obstruction EPSGHAN PDFDocument77 pagesNeonatal Intestinal Obstruction EPSGHAN PDFRobert ChristevenNo ratings yet
- Print PDFDocument16 pagesPrint PDFRobert ChristevenNo ratings yet
- Cancers: Gastric Cancer in History: A Perspective Interdisciplinary StudyDocument15 pagesCancers: Gastric Cancer in History: A Perspective Interdisciplinary StudyRobert ChristevenNo ratings yet
- Fukuoka, AJCS PDFDocument12 pagesFukuoka, AJCS PDFRobert ChristevenNo ratings yet
- Print PDFDocument16 pagesPrint PDFRobert ChristevenNo ratings yet
- The Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionDocument10 pagesThe Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionRobert ChristevenNo ratings yet
- 405 699 1 PBDocument6 pages405 699 1 PBRobert ChristevenNo ratings yet
- WHO Ultrasound Manual Vol2 PDFDocument529 pagesWHO Ultrasound Manual Vol2 PDFRobert ChristevenNo ratings yet
- Navsaria2016 Article PenetratingTraumaToTheMediastiDocument10 pagesNavsaria2016 Article PenetratingTraumaToTheMediastiRobert ChristevenNo ratings yet
- Referat TBDocument16 pagesReferat TBRobert ChristevenNo ratings yet
- Intestinal Obstruction E.C Atresia IleumDocument12 pagesIntestinal Obstruction E.C Atresia IleumRobert ChristevenNo ratings yet
- Escala SocratesDocument3 pagesEscala SocratesarNo ratings yet
- Removing The Guesswork From Potency SelectionDocument11 pagesRemoving The Guesswork From Potency SelectionRehan AnisNo ratings yet
- Nasopharyngeal Carcinoma in Children and AdolescentsDocument5 pagesNasopharyngeal Carcinoma in Children and AdolescentsSyifa MunawarahNo ratings yet
- Closed Fracture of Middle ClaviculaDocument12 pagesClosed Fracture of Middle ClaviculachiciNo ratings yet
- Model AnalysisDocument7 pagesModel Analysissrishti jainNo ratings yet
- Home MedicineDocument29 pagesHome MedicineBasanthanesh BasanNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument16 pagesRajiv Gandhi University of Health Sciences Bangalore, KarnatakaYadnya SaputraNo ratings yet
- 1Document18 pages1Japheth GofredoNo ratings yet
- Ampalaya CandyDocument16 pagesAmpalaya Candycharlesjoshdaniel83% (6)
- Slender Quest DetailsDocument1 pageSlender Quest Detailsparents021No ratings yet
- Ust Anatomy Mock 2015-1 PDFDocument7 pagesUst Anatomy Mock 2015-1 PDFJanna Janoras ŰNo ratings yet
- Questions 2011 - License ExamDocument196 pagesQuestions 2011 - License ExamDr-mustafa NazarNo ratings yet
- Chemical Constituents From The Stems Of: Celastrus OrbiculatusDocument5 pagesChemical Constituents From The Stems Of: Celastrus OrbiculatusTuan PhamquocNo ratings yet
- Psych Unit I Part 1Document42 pagesPsych Unit I Part 1api-293070066No ratings yet
- CSS Osteoarthritis GenuDocument33 pagesCSS Osteoarthritis Genufatimah putriNo ratings yet
- Age Appropriate Dosage For ChildrenDocument22 pagesAge Appropriate Dosage For Childrenmukesh choudharyNo ratings yet
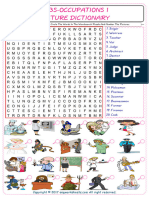
- Jobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Document2 pagesJobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Raquel NoeliaNo ratings yet
- General and Local AnesthesiaDocument1 pageGeneral and Local Anesthesiaahmedhelper300No ratings yet
- Daftar PustakaDocument2 pagesDaftar Pustakasantis_8No ratings yet
- CetakDocument140 pagesCetakFuzoh MfzNo ratings yet
- ObjectiveDocument2 pagesObjectiveMarvinNo ratings yet
- OSU Orthopaedics Accomplishments Report 2010Document32 pagesOSU Orthopaedics Accomplishments Report 2010osuorthopaedicsNo ratings yet
- რკინადეფიციტური ანემიაDocument25 pagesრკინადეფიციტური ანემიაoliko maglakvelidzeNo ratings yet
- 37.mon Tieng Anh - Chuyen Lam Son - Thanh Hoa - Lan 2 - (Hoctai - VN)Document20 pages37.mon Tieng Anh - Chuyen Lam Son - Thanh Hoa - Lan 2 - (Hoctai - VN)Thúy HiềnNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Professional Nursing Practice Key Points Professional Nursing PracticeDocument3 pagesLewis: Medical-Surgical Nursing, 10 Edition: Professional Nursing Practice Key Points Professional Nursing PracticePrincess AgarwalNo ratings yet
- Jurnal Terindeks ScopusDocument8 pagesJurnal Terindeks ScopusAyu Sisca PrastiwiNo ratings yet
- Leeds Studies in English: Magic and MedicineDocument32 pagesLeeds Studies in English: Magic and MedicineSimonida Mona VulićNo ratings yet








































































































Download as doc, pdf, or txt
You might also like
- 1.pharmacy Technician Study GuideDocument31 pages1.pharmacy Technician Study GuideAlan Hao93% (14)
- Malnutrition Screening Tool (MST) : Obtain Consent To Complete This Screening by AskingDocument2 pagesMalnutrition Screening Tool (MST) : Obtain Consent To Complete This Screening by AskingAku dienaNo ratings yet
- Paul E. Steiner - Okinawa and Its People (I)Document10 pagesPaul E. Steiner - Okinawa and Its People (I)José Luis IgueNo ratings yet
- Evaluation of A New Model of Hind Limb Ischemia in Rabbit: and Paris, FranceDocument9 pagesEvaluation of A New Model of Hind Limb Ischemia in Rabbit: and Paris, FranceKharina AreeistyNo ratings yet
- Angiosome-Targeted Infrapopliteal EndovascularDocument9 pagesAngiosome-Targeted Infrapopliteal EndovascularPablo BoadaNo ratings yet
- Two-Stage Bone Lengthening With Reuse of A Single Intramedullary Telescopic Nail in Patients With AchondroplasiaDocument7 pagesTwo-Stage Bone Lengthening With Reuse of A Single Intramedullary Telescopic Nail in Patients With AchondroplasiaLizza Mora RNo ratings yet
- Total Calcanectomy For The Treatment of Calcaneal OsteomyelitisDocument4 pagesTotal Calcanectomy For The Treatment of Calcaneal OsteomyelitisCleff FlowersNo ratings yet
- Accepted Manuscript: Seminars in Vascular SurgeryDocument33 pagesAccepted Manuscript: Seminars in Vascular SurgeryAnis BergerNo ratings yet
- PRGF in Chronic Ulcers - Diabetic Foot UlcersDocument5 pagesPRGF in Chronic Ulcers - Diabetic Foot UlcersVikram ReddyNo ratings yet
- Surgical Treatment of Plantar First Metatarsal UlcerationsDocument8 pagesSurgical Treatment of Plantar First Metatarsal UlcerationsDalid Raul Nieto ZepedaNo ratings yet
- Calcanectomy For OsteomyelitisDocument7 pagesCalcanectomy For OsteomyelitisCleff FlowersNo ratings yet
- Is It Safe To Extract The Reverse Sural Artery Flap From The Proximal Third of The Leg?Document7 pagesIs It Safe To Extract The Reverse Sural Artery Flap From The Proximal Third of The Leg?yennysabriniNo ratings yet
- Elif KI (2021) - Tibiotalocalcaneal Intramedullary Nailing For Unstable Geriatric Ankle FracturesDocument7 pagesElif KI (2021) - Tibiotalocalcaneal Intramedullary Nailing For Unstable Geriatric Ankle FracturesHariom ShuklaNo ratings yet
- Duplex Guided Balloon Angioplasty and Subintimal DDocument8 pagesDuplex Guided Balloon Angioplasty and Subintimal DJose PiulatsNo ratings yet
- SN02Document11 pagesSN02Enrique San NorbertoNo ratings yet
- Advanced Limb Salvage - Pedal Artery InterventionsDocument10 pagesAdvanced Limb Salvage - Pedal Artery Interventionsafso afsoNo ratings yet
- Diabetic Limb Salvage Procedure With Bone Allograft and Free Flap Transfer: A Case ReportDocument9 pagesDiabetic Limb Salvage Procedure With Bone Allograft and Free Flap Transfer: A Case ReportJacob DoughertyNo ratings yet
- 1 s2.0 S0011853211000346 Main PDFDocument6 pages1 s2.0 S0011853211000346 Main PDFMichael XuNo ratings yet
- Complications and Morbidity Associated With Loop Ileostomies in Patients With Ulcerative ColitisDocument5 pagesComplications and Morbidity Associated With Loop Ileostomies in Patients With Ulcerative ColitisNathalia GonzalezNo ratings yet
- Et0420 MedAffairs MouawadDocument5 pagesEt0420 MedAffairs MouawadAna Silvia LebrOnNo ratings yet
- 10 5114@pdia 2016 62415Document6 pages10 5114@pdia 2016 62415senkonenNo ratings yet
- Specific Aspects of Percutaneous Closure of Patent Ductus Arteriosus in Adult PatientsDocument6 pagesSpecific Aspects of Percutaneous Closure of Patent Ductus Arteriosus in Adult PatientsTri RachmadijantoNo ratings yet
- 31MDI RET '17 JacksonDocument6 pages31MDI RET '17 Jacksoncd.brendasotofloresNo ratings yet
- 10 36516-Jocass 1276127-3055931Document5 pages10 36516-Jocass 1276127-3055931yyyyx842No ratings yet
- Modified Extrapleural Ligation of Patent Ductus Arteriosus: A Convenient Surgical Approach in A Developing CountryDocument4 pagesModified Extrapleural Ligation of Patent Ductus Arteriosus: A Convenient Surgical Approach in A Developing CountryHandyka Vb GNo ratings yet
- Reconstruction of Mandible by Free Fibular Flap: Original ArticleDocument5 pagesReconstruction of Mandible by Free Fibular Flap: Original ArticleSani Solihatul FitriNo ratings yet
- The Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionDocument10 pagesThe Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionRobert ChristevenNo ratings yet
- Bovine Digit Surgical TechniqueDocument16 pagesBovine Digit Surgical TechniqueWendyNo ratings yet
- TurkeyGMJ 62 200 enDocument6 pagesTurkeyGMJ 62 200 enCocoNo ratings yet
- Lymphedema Rates in Pedicled ALTP For Coverage in Irradiated Groin Defects 2019Document4 pagesLymphedema Rates in Pedicled ALTP For Coverage in Irradiated Groin Defects 2019yeapdshengNo ratings yet
- Varicose Veins: A Clinical Study: Original Research ArticleDocument5 pagesVaricose Veins: A Clinical Study: Original Research ArticleAndhika DNo ratings yet
- Treatment of Vascular Malformations of The Mandible: A Description of 12 CasesDocument5 pagesTreatment of Vascular Malformations of The Mandible: A Description of 12 CasesneyhaaNo ratings yet
- 1 s2.0 S2214031X20300693 MainDocument6 pages1 s2.0 S2214031X20300693 MainCristhian Jover CastroNo ratings yet
- NAIS Initial PaperDocument10 pagesNAIS Initial Paperjesus Porras ColonNo ratings yet
- Long-Term Outcome After Thrombolysis For Acute Lower Limb IschaemiaDocument9 pagesLong-Term Outcome After Thrombolysis For Acute Lower Limb IschaemiaIdham Adyasa Manggala PutraNo ratings yet
- Sural Island Flap - A Good Option For Coverage of The Exposed Heel (Tendo-Achillis)Document6 pagesSural Island Flap - A Good Option For Coverage of The Exposed Heel (Tendo-Achillis)yennysabriniNo ratings yet
- Monux 2020Document7 pagesMonux 2020dev darma karinggaNo ratings yet
- A Prospective Observational Study On Scola For Ventral Hernia With Diastasis Recti - Our Experience at A Tertiary Care HospitalDocument4 pagesA Prospective Observational Study On Scola For Ventral Hernia With Diastasis Recti - Our Experience at A Tertiary Care HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Use of External Fixation in The Reconstruction of The Charcot Foot and AnkleDocument21 pagesUse of External Fixation in The Reconstruction of The Charcot Foot and AnkleAnonymous kdBDppigENo ratings yet
- 20SPIGCDocument3 pages20SPIGCscribullNo ratings yet
- TRIGONOMETRIADocument7 pagesTRIGONOMETRIACatalina RodríguezNo ratings yet
- The Association Between Skin Blood Flow and Edema On Epidermal Thickness in The Diabetic FootDocument8 pagesThe Association Between Skin Blood Flow and Edema On Epidermal Thickness in The Diabetic FootdeborapkphnNo ratings yet
- Khan 2018Document5 pagesKhan 2018Ivor Wiguna Hartanto WilopoNo ratings yet
- LskjjdshiubifsDocument8 pagesLskjjdshiubifsAchmad Luthfi TiflaniNo ratings yet
- Evolving Approaches To The Iliacs, Femorals, Popliteals, and RenalsDocument12 pagesEvolving Approaches To The Iliacs, Femorals, Popliteals, and RenalsSohil ElfarNo ratings yet
- Efficacyof Vacuum Assisted Closure VACTherapyin Healingof Diabetic Foot Ulcerandafter Diabetic Foot AmputationDocument11 pagesEfficacyof Vacuum Assisted Closure VACTherapyin Healingof Diabetic Foot Ulcerandafter Diabetic Foot AmputationZven BlackNo ratings yet
- Ismaeil 2018Document15 pagesIsmaeil 2018Javier ZaquinaulaNo ratings yet
- Tom Skin-Sparing Approach To Treatemen of NSTI 2016Document14 pagesTom Skin-Sparing Approach To Treatemen of NSTI 2016Sadaf Raisa KhanNo ratings yet
- Bridging Plate Osteosynthesis of Humeral Shaft Fractures: Bruno Livani, William Dias BelangeroDocument9 pagesBridging Plate Osteosynthesis of Humeral Shaft Fractures: Bruno Livani, William Dias BelangeroMiguel Angel Lamas RamirezNo ratings yet
- Elective Frozen Elephant Trunk Procedure Using The E-Vita Open Plus Prosthesis in 94 Patients: A Multicentre French RegistryDocument7 pagesElective Frozen Elephant Trunk Procedure Using The E-Vita Open Plus Prosthesis in 94 Patients: A Multicentre French RegistryrédaNo ratings yet
- Lobular Capillary Hemangioma An Extremely Rare Entity in The Retromolar Region Case ReportDocument5 pagesLobular Capillary Hemangioma An Extremely Rare Entity in The Retromolar Region Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Alogénico Vs AutoóogoDocument4 pagesAlogénico Vs AutoóogoMaximiliano Jara ContrerasNo ratings yet
- Lemus Rangel 2010Document2 pagesLemus Rangel 2010audiNo ratings yet
- FIRST2020Document10 pagesFIRST2020Jeisson Daniel Barrera AlvarezNo ratings yet
- Is Mesh Always Necessary in Every Small UmbilicalDocument8 pagesIs Mesh Always Necessary in Every Small UmbilicalLeonardo RibeiroNo ratings yet
- Management of Anastomotic Leaks After Esophagectomy and Gastric Pull-UpDocument9 pagesManagement of Anastomotic Leaks After Esophagectomy and Gastric Pull-UpSergio Sitta TarquiniNo ratings yet
- The Journal of Foot & Ankle Surgery: Christopher Bibbo, DO, DPM, FACFASDocument5 pagesThe Journal of Foot & Ankle Surgery: Christopher Bibbo, DO, DPM, FACFASdamonenNo ratings yet
- Lee 2015Document7 pagesLee 2015AncaVerdesNo ratings yet
- Ma 2021Document6 pagesMa 2021bigben9262No ratings yet
- Pe Rich On DR It Is of The Auricle and Its ManagementDocument6 pagesPe Rich On DR It Is of The Auricle and Its ManagementmitaNo ratings yet
- Endoscopic Treatment of Choanal Atresia and Use of Balloon Dilation: Our ExperienceDocument6 pagesEndoscopic Treatment of Choanal Atresia and Use of Balloon Dilation: Our Experiencefarah maulida martaNo ratings yet
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementFrom EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementNo ratings yet
- Designing A Breast Abscess Pathway: A Guide For General SurgeonsDocument5 pagesDesigning A Breast Abscess Pathway: A Guide For General SurgeonsRobert ChristevenNo ratings yet
- MC Participant 0Document220 pagesMC Participant 0Robert ChristevenNo ratings yet
- Summary Diagnostic Guidelines PAD CLI Diabetic Foot PerimedDocument38 pagesSummary Diagnostic Guidelines PAD CLI Diabetic Foot PerimedRobert ChristevenNo ratings yet
- Technique: Median Sternotomy - Gold Standard Incision For Cardiac SurgeonsDocument8 pagesTechnique: Median Sternotomy - Gold Standard Incision For Cardiac SurgeonsRobert ChristevenNo ratings yet
- Raza 2017Document7 pagesRaza 2017Robert ChristevenNo ratings yet
- Systems Biology of Gastric Cancer: Perspectives On The Omics-Based Diagnosis and TreatmentDocument8 pagesSystems Biology of Gastric Cancer: Perspectives On The Omics-Based Diagnosis and TreatmentRobert ChristevenNo ratings yet
- The Principles of The Surgical Management of Gastric CancerDocument5 pagesThe Principles of The Surgical Management of Gastric CancerRobert ChristevenNo ratings yet
- Neonatal Intestinal Obstruction EPSGHAN PDFDocument77 pagesNeonatal Intestinal Obstruction EPSGHAN PDFRobert ChristevenNo ratings yet
- Print PDFDocument16 pagesPrint PDFRobert ChristevenNo ratings yet
- Cancers: Gastric Cancer in History: A Perspective Interdisciplinary StudyDocument15 pagesCancers: Gastric Cancer in History: A Perspective Interdisciplinary StudyRobert ChristevenNo ratings yet
- Fukuoka, AJCS PDFDocument12 pagesFukuoka, AJCS PDFRobert ChristevenNo ratings yet
- Print PDFDocument16 pagesPrint PDFRobert ChristevenNo ratings yet
- The Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionDocument10 pagesThe Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionRobert ChristevenNo ratings yet
- 405 699 1 PBDocument6 pages405 699 1 PBRobert ChristevenNo ratings yet
- WHO Ultrasound Manual Vol2 PDFDocument529 pagesWHO Ultrasound Manual Vol2 PDFRobert ChristevenNo ratings yet
- Navsaria2016 Article PenetratingTraumaToTheMediastiDocument10 pagesNavsaria2016 Article PenetratingTraumaToTheMediastiRobert ChristevenNo ratings yet
- Referat TBDocument16 pagesReferat TBRobert ChristevenNo ratings yet
- Intestinal Obstruction E.C Atresia IleumDocument12 pagesIntestinal Obstruction E.C Atresia IleumRobert ChristevenNo ratings yet
- Escala SocratesDocument3 pagesEscala SocratesarNo ratings yet
- Removing The Guesswork From Potency SelectionDocument11 pagesRemoving The Guesswork From Potency SelectionRehan AnisNo ratings yet
- Nasopharyngeal Carcinoma in Children and AdolescentsDocument5 pagesNasopharyngeal Carcinoma in Children and AdolescentsSyifa MunawarahNo ratings yet
- Closed Fracture of Middle ClaviculaDocument12 pagesClosed Fracture of Middle ClaviculachiciNo ratings yet
- Model AnalysisDocument7 pagesModel Analysissrishti jainNo ratings yet
- Home MedicineDocument29 pagesHome MedicineBasanthanesh BasanNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument16 pagesRajiv Gandhi University of Health Sciences Bangalore, KarnatakaYadnya SaputraNo ratings yet
- 1Document18 pages1Japheth GofredoNo ratings yet
- Ampalaya CandyDocument16 pagesAmpalaya Candycharlesjoshdaniel83% (6)
- Slender Quest DetailsDocument1 pageSlender Quest Detailsparents021No ratings yet
- Ust Anatomy Mock 2015-1 PDFDocument7 pagesUst Anatomy Mock 2015-1 PDFJanna Janoras ŰNo ratings yet
- Questions 2011 - License ExamDocument196 pagesQuestions 2011 - License ExamDr-mustafa NazarNo ratings yet
- Chemical Constituents From The Stems Of: Celastrus OrbiculatusDocument5 pagesChemical Constituents From The Stems Of: Celastrus OrbiculatusTuan PhamquocNo ratings yet
- Psych Unit I Part 1Document42 pagesPsych Unit I Part 1api-293070066No ratings yet
- CSS Osteoarthritis GenuDocument33 pagesCSS Osteoarthritis Genufatimah putriNo ratings yet
- Age Appropriate Dosage For ChildrenDocument22 pagesAge Appropriate Dosage For Childrenmukesh choudharyNo ratings yet
- Jobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Document2 pagesJobs-Occupations Find and Circle The Words in The Wordsearch Puzzle and Number The Pictures 7531Raquel NoeliaNo ratings yet
- General and Local AnesthesiaDocument1 pageGeneral and Local Anesthesiaahmedhelper300No ratings yet
- Daftar PustakaDocument2 pagesDaftar Pustakasantis_8No ratings yet
- CetakDocument140 pagesCetakFuzoh MfzNo ratings yet
- ObjectiveDocument2 pagesObjectiveMarvinNo ratings yet
- OSU Orthopaedics Accomplishments Report 2010Document32 pagesOSU Orthopaedics Accomplishments Report 2010osuorthopaedicsNo ratings yet
- რკინადეფიციტური ანემიაDocument25 pagesრკინადეფიციტური ანემიაoliko maglakvelidzeNo ratings yet
- 37.mon Tieng Anh - Chuyen Lam Son - Thanh Hoa - Lan 2 - (Hoctai - VN)Document20 pages37.mon Tieng Anh - Chuyen Lam Son - Thanh Hoa - Lan 2 - (Hoctai - VN)Thúy HiềnNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Professional Nursing Practice Key Points Professional Nursing PracticeDocument3 pagesLewis: Medical-Surgical Nursing, 10 Edition: Professional Nursing Practice Key Points Professional Nursing PracticePrincess AgarwalNo ratings yet
- Jurnal Terindeks ScopusDocument8 pagesJurnal Terindeks ScopusAyu Sisca PrastiwiNo ratings yet
- Leeds Studies in English: Magic and MedicineDocument32 pagesLeeds Studies in English: Magic and MedicineSimonida Mona VulićNo ratings yet