Download as pdf or txt
You might also like
- Saying No To Vaccin - DR SHERRI TENPENNYDocument5 pagesSaying No To Vaccin - DR SHERRI TENPENNYJunior Jusme100% (2)
- Vaxxed Vs Unvaxxed Study - The Study The CDC Refused To Do (Phase 1)Document5 pagesVaxxed Vs Unvaxxed Study - The Study The CDC Refused To Do (Phase 1)Tim BrownNo ratings yet
- Reflections On The Distance Learning ProgramDocument6 pagesReflections On The Distance Learning ProgramEL BertNo ratings yet
- ICAN White Paper With Cover PageDocument38 pagesICAN White Paper With Cover Pagejudymw2000No ratings yet
- Annotated Bibliography On VaccinationsDocument4 pagesAnnotated Bibliography On VaccinationsRyan MarshNo ratings yet
- Belgian DPA Registry of Processing Activities Template 20170907 enDocument71 pagesBelgian DPA Registry of Processing Activities Template 20170907 enNicola FioriNo ratings yet
- Linamar Corporation: Health & Safety at WorkDocument10 pagesLinamar Corporation: Health & Safety at WorkRavi KumawatNo ratings yet
- Pak Suzuki Motors Company Limited: Operations Management: Teacher: Sir Khurram AminDocument4 pagesPak Suzuki Motors Company Limited: Operations Management: Teacher: Sir Khurram AminWarda TariqNo ratings yet
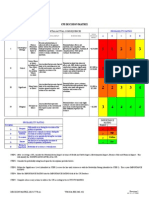
- Decision MatrixDocument12 pagesDecision Matrixrdos14No ratings yet
- Naip Response - Daniel BoyleDocument7 pagesNaip Response - Daniel Boyleapi-241125450No ratings yet
- Policy BriefDocument10 pagesPolicy Briefapi-438364488No ratings yet
- Retraction-Ileal-lymphoid-nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenDocument1 pageRetraction-Ileal-lymphoid-nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenOutlawHealthNo ratings yet
- Research Paper Outline VaccinesDocument9 pagesResearch Paper Outline Vaccinessvgkjqbnd100% (1)
- Letter of Non-Consent To Mandatory or Coerced COVID-19 VaccinesDocument72 pagesLetter of Non-Consent To Mandatory or Coerced COVID-19 VaccinesMark LaceyNo ratings yet
- VACCINATION DANGERS - The Health Hazards of Disease Prevention - BSEM-2011Document45 pagesVACCINATION DANGERS - The Health Hazards of Disease Prevention - BSEM-2011bigbill138No ratings yet
- Lucija Tomljenovic - The Vaccination Policy and The Code of Practice of The JCVIDocument45 pagesLucija Tomljenovic - The Vaccination Policy and The Code of Practice of The JCVITratincica StewartNo ratings yet
- Running Head: Analysis of A U.S. Health Care Policy 1Document6 pagesRunning Head: Analysis of A U.S. Health Care Policy 1api-520930030No ratings yet
- Smallpox (Variola Virus) Infection: Developing Drugs For Treatment or PreventionDocument16 pagesSmallpox (Variola Virus) Infection: Developing Drugs For Treatment or PreventionPriya JainNo ratings yet
- V VV Vvaccine Accine Accine Accine Accine Safety Safety Safety Safety SafetyDocument12 pagesV VV Vvaccine Accine Accine Accine Accine Safety Safety Safety Safety SafetyJandre ShancezNo ratings yet
- Vaccines - The Week in Review - 3 January 2011Document16 pagesVaccines - The Week in Review - 3 January 2011davidrcurryNo ratings yet
- The Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionFrom EverandThe Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionNo ratings yet
- English 101 Final EssayDocument13 pagesEnglish 101 Final EssayHa HangNo ratings yet
- Dol Osha 18oct21Document7 pagesDol Osha 18oct21Chris DriverNo ratings yet
- Are Vaccines SafeDocument3 pagesAre Vaccines SafeJun Kai Ong100% (1)
- Guidance For IndustryDocument14 pagesGuidance For IndustryRamboNo ratings yet
- Swine Flu White PaperDocument94 pagesSwine Flu White Paperlocopr1100% (1)
- California Bill 2015 LucijaDocument17 pagesCalifornia Bill 2015 Lucijaapi-246003035No ratings yet
- Report EssayDocument5 pagesReport Essayapi-534909132No ratings yet
- The Awareness Level On The Benefit1Document12 pagesThe Awareness Level On The Benefit1Joshua ValledorNo ratings yet
- ControlGroup PilotSurvey SummaryGuideDocument17 pagesControlGroup PilotSurvey SummaryGuidegabrielaizcorbeNo ratings yet
- Vaccine White Paper 2017Document34 pagesVaccine White Paper 2017indianajones13100% (1)
- National Adult Immunization Plan: The National Vaccine Program OfficeDocument67 pagesNational Adult Immunization Plan: The National Vaccine Program OfficeNavdeep GogiaNo ratings yet
- 2022 VaccineInjuryTreatmentGuide 4-29-22 FINALDocument26 pages2022 VaccineInjuryTreatmentGuide 4-29-22 FINALYonathan Rojas100% (1)
- Continuing To Follow The Science - An Open Letter From Pfizer Chairman and CEO Dr. Albert Bourla - PfizerDocument4 pagesContinuing To Follow The Science - An Open Letter From Pfizer Chairman and CEO Dr. Albert Bourla - PfizerJohn DoeNo ratings yet
- phsc002 Video ScriptDocument4 pagesphsc002 Video Scriptapi-301372772No ratings yet
- U D C C E: Niversity of Haka Pplied Hemistry and Hemical NgineeringDocument6 pagesU D C C E: Niversity of Haka Pplied Hemistry and Hemical NgineeringMD: Shamim HossainNo ratings yet
- KSLING1Document5 pagesKSLING1Clarita BangunNo ratings yet
- Ican Vs CDC Lawsuit PRDocument3 pagesIcan Vs CDC Lawsuit PRJamie White100% (5)
- FDA Petitioned by Experts, Here's Why...Document5 pagesFDA Petitioned by Experts, Here's Why...stummel6636No ratings yet
- A Position Paper About Vaccines To Fight Infectious DiseasesDocument6 pagesA Position Paper About Vaccines To Fight Infectious DiseasesJonas Belen PerezNo ratings yet
- The Plausible Link Between Vaccines and Autism Has Not Been DebunkedDocument7 pagesThe Plausible Link Between Vaccines and Autism Has Not Been DebunkedSofia marisa fernandesNo ratings yet
- Bracing Ourselves Sham Vaccine StudiesDocument11 pagesBracing Ourselves Sham Vaccine StudiesGary Null100% (4)
- Reporte 2020 de La Oficina de Asuntos Globales de Estados UnidosDocument72 pagesReporte 2020 de La Oficina de Asuntos Globales de Estados UnidosAristegui NoticiasNo ratings yet
- Una Caca de Articulo CientificoDocument3 pagesUna Caca de Articulo Cientificojignacio89No ratings yet
- (Vaccine Package Inserts Carry Warnings) Best Practices For Physicians Writing A Medical Exemption To VaccinationDocument27 pages(Vaccine Package Inserts Carry Warnings) Best Practices For Physicians Writing A Medical Exemption To VaccinationSY LodhiNo ratings yet
- Nvicp 1980Document106 pagesNvicp 1980Gene XeneNo ratings yet
- Bio TerrorismDocument33 pagesBio TerrorismergiNo ratings yet
- Vaccine HesitancyDocument2 pagesVaccine HesitancyFred smithNo ratings yet
- Vacuna Minnesota 2008 HpvreportDocument28 pagesVacuna Minnesota 2008 Hpvreportapi-26512586No ratings yet
- Policy Brief FinalDocument5 pagesPolicy Brief Finalapi-311881661No ratings yet
- Garner 1511222Document17 pagesGarner 1511222Bj LongNo ratings yet
- 18 Facts About Vaccine RisksDocument2 pages18 Facts About Vaccine Risksmacgeekinside1412No ratings yet
- Identifying Post-Vaccination Complications & Their Causes: An Analysis of Covid-19 Patient DataDocument4 pagesIdentifying Post-Vaccination Complications & Their Causes: An Analysis of Covid-19 Patient DataconisbraNo ratings yet
- The Vaccine Injury Compensation Program (VICP) : Who Can File A Claim?Document2 pagesThe Vaccine Injury Compensation Program (VICP) : Who Can File A Claim?Mommyx44No ratings yet
- Coronavirus Vaccine - Summary of Yellow Card Reporting: Data Included: 09/12/2020 To 07/03/2021Document17 pagesCoronavirus Vaccine - Summary of Yellow Card Reporting: Data Included: 09/12/2020 To 07/03/2021José BacigalupoNo ratings yet
- Vaccines Final DraftDocument6 pagesVaccines Final Draftapi-456880732No ratings yet
- Coronavirus Vaccine - Summary of Yellow Card Reporting 28.02.21Document17 pagesCoronavirus Vaccine - Summary of Yellow Card Reporting 28.02.21Zsi GaNo ratings yet
- A Critical Review Evaluation of The Efficacy of Covid19 Vaccines in EnglandDocument14 pagesA Critical Review Evaluation of The Efficacy of Covid19 Vaccines in EnglandvalgurNo ratings yet
- RRL 01 07 22Document9 pagesRRL 01 07 22Ponce GuerreroNo ratings yet
- Letter On Behalf of Physicians Regarding Covid 19 Vaccine InjuriDocument42 pagesLetter On Behalf of Physicians Regarding Covid 19 Vaccine InjuriDaniyaNo ratings yet
- Brainstorming About Vaccines-1 1Document6 pagesBrainstorming About Vaccines-1 1api-242698568No ratings yet
- Unanswered Questions From The Vaccine Injury Compensation ProgramDocument65 pagesUnanswered Questions From The Vaccine Injury Compensation ProgramHeather X Rhodes100% (1)
- Summary of Vax-Unvax by Robert F. Kennedy Jr.: Let the Science Speak (Children’s Health Defense)From EverandSummary of Vax-Unvax by Robert F. Kennedy Jr.: Let the Science Speak (Children’s Health Defense)No ratings yet
- Vaccine Injuries: Documented Adverse Reactions to VaccinesFrom EverandVaccine Injuries: Documented Adverse Reactions to VaccinesRating: 2.5 out of 5 stars2.5/5 (3)
- Chnchal - Samsung CSRDocument4 pagesChnchal - Samsung CSRMamta NarulaNo ratings yet
- The Role of HR Managers in International Mergers and Acquisitions: A Multiple Case StudyDocument23 pagesThe Role of HR Managers in International Mergers and Acquisitions: A Multiple Case StudyOmar QudahNo ratings yet
- Career Report AssignmentDocument2 pagesCareer Report Assignmentapi-364906297No ratings yet
- Buss Org 1Document17 pagesBuss Org 1NaigAnipseNo ratings yet
- Fatigue Management Plan: (XXX Company (XXX Company)Document9 pagesFatigue Management Plan: (XXX Company (XXX Company)Sunday Augustine ChibuzoNo ratings yet
- Sim v. NLRCDocument14 pagesSim v. NLRCjoycebaylonNo ratings yet
- Lecture 1 Global and National Situation in OSHDocument29 pagesLecture 1 Global and National Situation in OSHShaira Eiram ZayasNo ratings yet
- IT Academy ERR WorkbookDocument30 pagesIT Academy ERR Workbooksean12266727No ratings yet
- Labor Relations Case DigestDocument23 pagesLabor Relations Case DigestImma FoosaNo ratings yet
- INDIA: Bonded Labour in IndiaDocument3 pagesINDIA: Bonded Labour in Indianludelhi2009No ratings yet
- Social Security in IndiaDocument4 pagesSocial Security in IndiaBoina RamshaNo ratings yet
- MD Shamsur Rahman: Career ObjectiveDocument3 pagesMD Shamsur Rahman: Career ObjectiveShamsur RahmanNo ratings yet
- TAPA TSR 2008 Audit Form PDFDocument3 pagesTAPA TSR 2008 Audit Form PDFReneeNo ratings yet
- HR Thesis Topics For PHDDocument7 pagesHR Thesis Topics For PHDmitzilarrickakron100% (2)
- Tax 1 Cases On Allowable DeductionsDocument45 pagesTax 1 Cases On Allowable DeductionsREJFREEFALLNo ratings yet
- State Law Guide - Employment Rights For Victims of Domestic or Sexual ViolenceDocument32 pagesState Law Guide - Employment Rights For Victims of Domestic or Sexual ViolenceLegal MomentumNo ratings yet
- G.R. No. 159577 May 3, 2006 Charlito PEÑARANDA, Petitioner, Baganga Plywood Corporation and Hudson Chua, RespondentsDocument62 pagesG.R. No. 159577 May 3, 2006 Charlito PEÑARANDA, Petitioner, Baganga Plywood Corporation and Hudson Chua, RespondentsJoannah SalamatNo ratings yet
- Krystel Smalls Senior Recruiter AIRSDocument2 pagesKrystel Smalls Senior Recruiter AIRSkrystelsmallsNo ratings yet
- WEBSITE RA-100249 - MECHANICAL ENGINEER - Baguio - 8-2022Document55 pagesWEBSITE RA-100249 - MECHANICAL ENGINEER - Baguio - 8-2022Mark Anthony NalapoNo ratings yet
- Hema Nagpal: Vice President Human ResourcesDocument3 pagesHema Nagpal: Vice President Human ResourcesKushal SainNo ratings yet
- Hitachi Electronic Products (M) Sdn. Bhd. - Group 5Document25 pagesHitachi Electronic Products (M) Sdn. Bhd. - Group 5NUR ADAWIYYAH BINTI AZMAN KTNNo ratings yet
- Internship ReportDocument117 pagesInternship ReportMeghaa Dasari100% (1)
- Leadership VolkswagenDocument18 pagesLeadership Volkswagenkanishka katariaNo ratings yet
- D. Principles and Policies of The Philippine GovernmentDocument25 pagesD. Principles and Policies of The Philippine GovernmentYen055No ratings yet
- Chapter 7 Training and Development Chapter DescriptionDocument11 pagesChapter 7 Training and Development Chapter DescriptionOliver Fenianos50% (2)