Download as pdf or txt
You might also like
- Nebosh Igc1 Past ExamDocument15 pagesNebosh Igc1 Past Examkamy21481% (21)
- Snake Bite ToxiconDocument14 pagesSnake Bite ToxiconAETCM Emergency medicine100% (1)
- WPC in Ice CreamDocument5 pagesWPC in Ice CreamIvan MojsaNo ratings yet
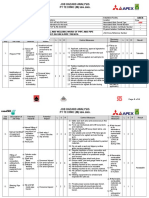
- JSA Fitting and Welding Work For Pipe Trench InstalationDocument6 pagesJSA Fitting and Welding Work For Pipe Trench InstalationVishnu VijayanNo ratings yet
- t180 6902502 SM 7-09Document961 pagest180 6902502 SM 7-09vadim vadim100% (3)
- Polyvalent Snake Antivenom Product InformationDocument9 pagesPolyvalent Snake Antivenom Product Informationumarn1582No ratings yet
- Treatment Protocol of Snake Bite: Kaushik.H.M 080201388Document23 pagesTreatment Protocol of Snake Bite: Kaushik.H.M 080201388tiruchanurNo ratings yet
- Antivenom PolyvalentDocument10 pagesAntivenom PolyvalentRifai ArfanNo ratings yet
- Sii Polyvalent AntiDocument4 pagesSii Polyvalent AntiMico AprueboNo ratings yet
- Sarpa All BasicsDocument11 pagesSarpa All BasicsRavichandra MentheNo ratings yet
- Polyvalent Snake Antivenom Safety Data SheetDocument6 pagesPolyvalent Snake Antivenom Safety Data SheetJoel TendoNo ratings yet
- Bites Snake SpiderDocument7 pagesBites Snake Spiderzenagit123456No ratings yet
- Treatment Protocol of SnakebiteDocument23 pagesTreatment Protocol of SnakebiteEduconsultNo ratings yet
- Antivenom Therapy SBG2021Document5 pagesAntivenom Therapy SBG2021anju sulishaNo ratings yet
- Drug Alert: Anti Snake Venom (Asv) Reactions - A PerspectiveDocument2 pagesDrug Alert: Anti Snake Venom (Asv) Reactions - A PerspectiveKUSUMSKNo ratings yet
- Canigen l4 Epar Product Information - en PDFDocument21 pagesCanigen l4 Epar Product Information - en PDFKris Pam Gorion PerezNo ratings yet
- ToxicDocument4 pagesToxicRachel RodríguezNo ratings yet
- Snakebite Poisoning Viva2019Document6 pagesSnakebite Poisoning Viva2019Meer HomerNo ratings yet
- Therapeutic Contraindications in Exotic PetsDocument14 pagesTherapeutic Contraindications in Exotic Pets黃皓No ratings yet
- 1 Snake BiteDocument8 pages1 Snake BiteMatthew Wei Hua CaiNo ratings yet
- Nobivac l4 Epar Product Information - enDocument18 pagesNobivac l4 Epar Product Information - enakshaygarande4048No ratings yet
- API Snakebite ManagementDocument3 pagesAPI Snakebite Managementsyed aquibNo ratings yet
- Enfoque de Emergencias de Las Intoxicaciones Animales. 2000Document6 pagesEnfoque de Emergencias de Las Intoxicaciones Animales. 2000Jakeline MezNo ratings yet
- Anaphylaxis Articulo CompletoDocument6 pagesAnaphylaxis Articulo CompletoFrancelia Quiñonez RuvalcabaNo ratings yet
- Revised: December 2015 AN: 01163/2015: TH THDocument6 pagesRevised: December 2015 AN: 01163/2015: TH THDavid WalshNo ratings yet
- ANAPHYLAXISDocument21 pagesANAPHYLAXISMicah TuringanNo ratings yet
- Leva FlukeDocument5 pagesLeva FlukeراجيرحمةربهNo ratings yet
- Training CasesDocument8 pagesTraining CasesManisanthosh KumarNo ratings yet
- Birds and Exotics - MCannon PDFDocument42 pagesBirds and Exotics - MCannon PDFAl OyNo ratings yet
- Snake Bite 1234Document23 pagesSnake Bite 1234awais ahmedNo ratings yet
- SPC LutalyzeDocument13 pagesSPC LutalyzeSatriyo Setyo UtomoNo ratings yet
- Pedia PracticalDocument29 pagesPedia Practicalanurag tripathyNo ratings yet
- Anestesia en Ovejas y CabrasDocument13 pagesAnestesia en Ovejas y CabrasAlejandra Castiñeyras ZapataNo ratings yet
- Snake Bite - Indian Guidelines and ProtocolDocument3 pagesSnake Bite - Indian Guidelines and ProtocolSushobhanSarkarNo ratings yet
- Rtc-Scent 2012 05 Octaplex ProtocolDocument1 pageRtc-Scent 2012 05 Octaplex Protocolirene aureliaNo ratings yet
- ASCIA Guidelines Acute Management Anaphylaxis Dec2016Document5 pagesASCIA Guidelines Acute Management Anaphylaxis Dec2016kkkssbbNo ratings yet
- Vomito en Perros Con Agua Oxigenada (Estudio Científico)Document6 pagesVomito en Perros Con Agua Oxigenada (Estudio Científico)sasasaNo ratings yet
- Pre Anesthetic Agent NoteDocument18 pagesPre Anesthetic Agent Notefcrackers989No ratings yet
- Antidotes in Clinical Practice SeminarDocument77 pagesAntidotes in Clinical Practice Seminarkhaled eissaNo ratings yet
- Algae: What Are The Symptoms of Amnesic Shellfish Poisoning?Document33 pagesAlgae: What Are The Symptoms of Amnesic Shellfish Poisoning?Alexandria P. OrcajadaNo ratings yet
- Algae: What Are The Symptoms of Amnesic Shellfish Poisoning?Document28 pagesAlgae: What Are The Symptoms of Amnesic Shellfish Poisoning?ElizaMayBarrettoNo ratings yet
- Redback Spider FactsDocument3 pagesRedback Spider FactsPradeep WalaweNo ratings yet
- Drug StudyDocument7 pagesDrug StudyCarson BirthNo ratings yet
- ASCIA Acute Management of Anaphylaxis Guidelines 2015Document4 pagesASCIA Acute Management of Anaphylaxis Guidelines 2015tom8989No ratings yet
- Syok Anafilaksis 1Document4 pagesSyok Anafilaksis 1Mariatun Zahro NasutionNo ratings yet
- Managing Anaphylactic Shock Journal of Modern Pharmacy 2006Document3 pagesManaging Anaphylactic Shock Journal of Modern Pharmacy 2006Saputro AbdiNo ratings yet
- Clinical Management Protocol and Infection Control GuidelinesDocument16 pagesClinical Management Protocol and Infection Control Guidelinesalfaz lakhaniNo ratings yet
- GUT Decontamination: Clinical Toxicology 4 Pharm DDocument39 pagesGUT Decontamination: Clinical Toxicology 4 Pharm DFeroze FathimaNo ratings yet
- Snake Bits: Introduced by D. Abdallah Abd El Rahman Ali MohammediaDocument17 pagesSnake Bits: Introduced by D. Abdallah Abd El Rahman Ali MohammediaSalah Elbadawy100% (1)
- BiologicsDocument76 pagesBiologicsMylaCambriNo ratings yet
- Infanrix Ipv Pi AuDocument16 pagesInfanrix Ipv Pi Ausamm1982No ratings yet
- Drug InfoDocument11 pagesDrug InfoArjun SinghNo ratings yet
- Box Jellyfish Antivenom: Before You Are Given ItDocument1 pageBox Jellyfish Antivenom: Before You Are Given ItringpieceNo ratings yet
- Drug StudyDocument10 pagesDrug StudyBandana RajpootNo ratings yet
- AmoxitidDocument5 pagesAmoxitidelcapitano vegetaNo ratings yet
- Anaphylaxis Wallchart 2018Document1 pageAnaphylaxis Wallchart 2018simranNo ratings yet
- 10 1016@j Jpainsymman 2010 07 001Document5 pages10 1016@j Jpainsymman 2010 07 001Hugo Robles GómezNo ratings yet
- Box Jellyfish CMI - Dec08Document2 pagesBox Jellyfish CMI - Dec08ringpieceNo ratings yet
- Revised: January 2020 AN: 01190/2019: - Strongylus Vulgaris (Adult Stages) - Strongylus Edentatus (Adult Stages)Document7 pagesRevised: January 2020 AN: 01190/2019: - Strongylus Vulgaris (Adult Stages) - Strongylus Edentatus (Adult Stages)nicola vercoeNo ratings yet
- Suxamethonium Apnoea (Succinlycholine or Scoline Apnoea) (SA)Document2 pagesSuxamethonium Apnoea (Succinlycholine or Scoline Apnoea) (SA)amonlisaNo ratings yet
- Castration and OVH in CatsDocument1 pageCastration and OVH in CatsIbad Ur RahmanNo ratings yet
- Snake Bite ManagementDocument49 pagesSnake Bite ManagementChhabilal Bastola100% (1)
- Nissan Murano EngineMechanical ServiceManualDocument40 pagesNissan Murano EngineMechanical ServiceManualReza BahramiNo ratings yet
- Artepillin C As An Outstanding Phenolic Compound of Brazilian Green Propolis For Disease Treatment: A Review On Pharmacological AspectsDocument13 pagesArtepillin C As An Outstanding Phenolic Compound of Brazilian Green Propolis For Disease Treatment: A Review On Pharmacological AspectslyviaNo ratings yet
- BOOSTDocument16 pagesBOOSTChristous PkNo ratings yet
- Work Immersion Portfolio: Jhon Carlo Cera CatindoyDocument22 pagesWork Immersion Portfolio: Jhon Carlo Cera CatindoyJoel DufaleNo ratings yet
- CA1 Online Class 2Document13 pagesCA1 Online Class 2kemerutNo ratings yet
- Audio Frequency Amplifier Applications: Absolute Maximum RatingsDocument5 pagesAudio Frequency Amplifier Applications: Absolute Maximum RatingsDinh NguyenNo ratings yet
- Page 1 of 17Document17 pagesPage 1 of 17RamBabuMeenaNo ratings yet
- BSC Thesis - Eva Lind FellsDocument18 pagesBSC Thesis - Eva Lind FellsHanna Kate EnriquezNo ratings yet
- Reservoir Simulation Report UKCSDocument190 pagesReservoir Simulation Report UKCSValar MorghulisNo ratings yet
- Rojek Advance Solutions Employee HandbookDocument32 pagesRojek Advance Solutions Employee HandbookJämes ScarlétteNo ratings yet
- Recrystallization: Figure 1. Structure of AnilineDocument3 pagesRecrystallization: Figure 1. Structure of AnilineClaire Anne Caringal100% (1)
- Divya Kit Online All ProductsDocument6 pagesDivya Kit Online All ProductsDivya KitNo ratings yet
- Watts Zone Controls and Valves - 2Document16 pagesWatts Zone Controls and Valves - 2Sid KherNo ratings yet
- 1 - Vasudeo Joshi PDFDocument52 pages1 - Vasudeo Joshi PDFKoushik DeyNo ratings yet
- Pemerintah Kabupaten Klungkung Dinas Kesehatan: Jalan Gajah Mada No. 55 Semarapura Telp. (0366) 21150Document4 pagesPemerintah Kabupaten Klungkung Dinas Kesehatan: Jalan Gajah Mada No. 55 Semarapura Telp. (0366) 21150anggaNo ratings yet
- Biology Higher Level Paper 1: 8810-6001 17 Pages © International Baccalaureate Organization 2010Document17 pagesBiology Higher Level Paper 1: 8810-6001 17 Pages © International Baccalaureate Organization 2010Victor Junhe SONG [11S1]No ratings yet
- Legal Medicine NotesDocument57 pagesLegal Medicine NotesAnonymous pJnKhhxNo ratings yet
- Humms 11 Pasay Diass s2 q1 w2Document20 pagesHumms 11 Pasay Diass s2 q1 w2Victoria De Los SantosNo ratings yet
- Proposed Rule: Medicare: Electronic Prescription Drug Program E-PrescribingDocument20 pagesProposed Rule: Medicare: Electronic Prescription Drug Program E-PrescribingJustia.comNo ratings yet
- General PediatricsDocument21 pagesGeneral PediatricsShanmugam Balasubramaniam100% (2)
- Safety Data Sheet: Armohib 31Document12 pagesSafety Data Sheet: Armohib 31Dr. Pushkar ShuklaNo ratings yet
- ?CCS Template Guide Attachment 3 V2?Document32 pages?CCS Template Guide Attachment 3 V2?Umair HussainNo ratings yet
- A Healing Story About GuyabanoDocument4 pagesA Healing Story About GuyabanoZena Bezabih100% (1)
- Installation, Operation, & Maintenance ManualDocument48 pagesInstallation, Operation, & Maintenance ManualEdinsonUribeTorresNo ratings yet
- Competency Dictionary-PAO-PRCSDDocument2 pagesCompetency Dictionary-PAO-PRCSDJaymark L. AgmataNo ratings yet
- Ankylosing SpondylitisDocument34 pagesAnkylosing SpondylitisAnumeha SrivastavaNo ratings yet