Download as pdf or txt
You might also like
- العربية للناشئين كتاب التلميذ 1 PDFDocument231 pagesالعربية للناشئين كتاب التلميذ 1 PDFdirisaya100% (23)
- Introduction To Global Health 1Document38 pagesIntroduction To Global Health 1Enniie Akkanclalluecaiiankqmu100% (2)
- Power System Analysis II: Instructor: E-Mail: Office PhoneDocument66 pagesPower System Analysis II: Instructor: E-Mail: Office PhoneSelah TalepNo ratings yet
- Partners in Reduce, Reuse and RecycleDocument27 pagesPartners in Reduce, Reuse and RecycleRana RashidNo ratings yet
- The Emergence of Non-Communicable Disease in Indonesia: Dyah PurnamasariDocument2 pagesThe Emergence of Non-Communicable Disease in Indonesia: Dyah Purnamasarinene_luciaNo ratings yet
- Jurnal Penyakit Tidak Menular 1Document8 pagesJurnal Penyakit Tidak Menular 1IsrayaniNo ratings yet
- Pencegahan Dini Terhadap Penyakit Tidak 3a78b22fDocument8 pagesPencegahan Dini Terhadap Penyakit Tidak 3a78b22fmasNo ratings yet
- Konsumsi Makanan Berisiko Faktor Penyebab Penyakit Tidak MenularDocument6 pagesKonsumsi Makanan Berisiko Faktor Penyebab Penyakit Tidak MenularMuh NursyamsuNo ratings yet
- Karakteristik Penderita Hipertensi Di Puskesmas Titi Papan Kecamatan Medan Deli TAHUN 2012 Rio Iskandar, Rasmaliah, HiswaniDocument12 pagesKarakteristik Penderita Hipertensi Di Puskesmas Titi Papan Kecamatan Medan Deli TAHUN 2012 Rio Iskandar, Rasmaliah, HiswaniFarmasi RSUDNo ratings yet
- 10951-Article Text-36416-1-10-20201020Document8 pages10951-Article Text-36416-1-10-20201020Septy KawaiNo ratings yet
- Chapter OneDocument7 pagesChapter OneIvan grâceNo ratings yet
- Health Impact Framework Research Paper - Grisnel RosarioDocument10 pagesHealth Impact Framework Research Paper - Grisnel Rosarioapi-694898823No ratings yet
- Lifestyle Diseases Affecting The Nursing Faculty at Tarlac State University During Covid 19 PandemicDocument19 pagesLifestyle Diseases Affecting The Nursing Faculty at Tarlac State University During Covid 19 PandemicDeinielle Magdangal RomeroNo ratings yet
- NCD ScreeningDocument2 pagesNCD ScreeningAnant KumarNo ratings yet
- Diabetes What Challenges Lie Ahead For VietnamDocument9 pagesDiabetes What Challenges Lie Ahead For VietnamIik PandaranggaNo ratings yet
- Prevalence and Risk Factors For ChronicDocument10 pagesPrevalence and Risk Factors For ChronicKhoirul AnamNo ratings yet
- 261 Practice of Adults On Prevention of Hypertension and Associated Factors in Dessie Administrative City, Ethiopia, 2016Document12 pages261 Practice of Adults On Prevention of Hypertension and Associated Factors in Dessie Administrative City, Ethiopia, 2016Vibhor Kumar JainNo ratings yet
- Healthframework PaperDocument9 pagesHealthframework Paperapi-449184986No ratings yet
- MetabolismeDocument8 pagesMetabolismeAnonymous QCMhA4wNgBNo ratings yet
- A Case Report of Family MedicineDocument5 pagesA Case Report of Family Medicineanisnabilah raziNo ratings yet
- GRP No 8Document12 pagesGRP No 8alkinhamisiNo ratings yet
- Kecendrungan Penyakit Tidak Menular Dan Penelitiannya DJ IndoneslaDocument11 pagesKecendrungan Penyakit Tidak Menular Dan Penelitiannya DJ IndoneslaAbu siddiq AbrorNo ratings yet
- Jurnal 3Document5 pagesJurnal 3Mira D. Yuliana KoreNo ratings yet
- Families Family Policy and The SDGs (1) - 102-129Document28 pagesFamilies Family Policy and The SDGs (1) - 102-129Sylvia MaharanyNo ratings yet
- HypertensionDocument14 pagesHypertensionEvediciNo ratings yet
- Jurnal Aulia Abidzah, S.K.M PDFDocument10 pagesJurnal Aulia Abidzah, S.K.M PDFJamilah Sinaga100% (1)
- INTRODUCTIO1Document3 pagesINTRODUCTIO1steffy christNo ratings yet
- 3 11 38 983Document5 pages3 11 38 983Rumela Ganguly ChakrabortyNo ratings yet
- Mohan Et Al 2010 Epidemiology of Cardiovascular Disease in Type 2 Diabetes The Indian ScenarioDocument13 pagesMohan Et Al 2010 Epidemiology of Cardiovascular Disease in Type 2 Diabetes The Indian ScenarioAKASH BISWASNo ratings yet
- 89-Article Text-248-3-10-20191208Document16 pages89-Article Text-248-3-10-20191208Rizal MantovaniNo ratings yet
- Final File 56bf50335aa094.82062560Document4 pagesFinal File 56bf50335aa094.82062560nithya nithyaNo ratings yet
- Christ The KingDocument6 pagesChrist The KingAnonymous LPp1PuzFPQNo ratings yet
- 404-Article Text-780-1-10-20210910Document9 pages404-Article Text-780-1-10-20210910Ferdi JrNo ratings yet
- Heart Disease Mortality in The Philippines From 1960 To 2019: A Big Data AnalysisDocument13 pagesHeart Disease Mortality in The Philippines From 1960 To 2019: A Big Data AnalysisIJPHSNo ratings yet
- Karakteristik Penderita Hipertensi Di Puskesmas Titi Papan Kecamatan Medan Deli TAHUN 2012 Rio Iskandar, Rasmaliah, HiswaniDocument12 pagesKarakteristik Penderita Hipertensi Di Puskesmas Titi Papan Kecamatan Medan Deli TAHUN 2012 Rio Iskandar, Rasmaliah, HiswaniNabila NatasyaNo ratings yet
- 04CH Community BellDocument38 pages04CH Community BellBen KisebeNo ratings yet
- Epidemiology - Diabetes and Kidney Disease PDFDocument12 pagesEpidemiology - Diabetes and Kidney Disease PDFSharyna EmyraNo ratings yet
- Public Health Perspectives Journal: Prastuti Esaningsih - Ari Yuniastuti. Oktia Woro Kasmini HandayaniDocument9 pagesPublic Health Perspectives Journal: Prastuti Esaningsih - Ari Yuniastuti. Oktia Woro Kasmini HandayaniMuhammad Anwar AnsoriNo ratings yet
- Prevalence of Diabetes Mellitus in Patients Seeking Medical Care at Morogoro Regional Referral Hospital in TanzaniaDocument8 pagesPrevalence of Diabetes Mellitus in Patients Seeking Medical Care at Morogoro Regional Referral Hospital in TanzaniaEmmanuel MpaliyeNo ratings yet
- NIgeriaDocument15 pagesNIgeriaMarcos Chusin MontesdeocaNo ratings yet
- International Journal of Aging Research (ISSN:2637-3742) Primary Prevention of Alzheimer's Disease in IndonesiaDocument8 pagesInternational Journal of Aging Research (ISSN:2637-3742) Primary Prevention of Alzheimer's Disease in IndonesiasarahNo ratings yet
- Chronic Disease & Emergent Issues in Global HealthDocument16 pagesChronic Disease & Emergent Issues in Global HealthRai AlfiahNo ratings yet
- Epidemiologi (3) : (Epidemiologi Penyakit Tidak Menular)Document10 pagesEpidemiologi (3) : (Epidemiologi Penyakit Tidak Menular)Daw AddawNo ratings yet
- Cardiovascular Disease Risk Level of The Division Office Personnel of The Department of Education, Division of BohoDocument15 pagesCardiovascular Disease Risk Level of The Division Office Personnel of The Department of Education, Division of BohoPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Cardiovascular Diseases (CVDS) Morbidity MortalityDocument5 pagesCardiovascular Diseases (CVDS) Morbidity MortalityBen ObiNo ratings yet
- Nutrients 14 02649 - Tugas STR KeperawatanDocument15 pagesNutrients 14 02649 - Tugas STR KeperawatanteemgevzNo ratings yet
- ArticlesDocument955 pagesArticlesMuhammad ChohanNo ratings yet
- PHR211Public Health: Chronic Disease EpidemiologyDocument21 pagesPHR211Public Health: Chronic Disease EpidemiologyNuhu SibaNo ratings yet
- 1 PBDocument8 pages1 PBCM GabriellaNo ratings yet
- نسخة ProposalDocument17 pagesنسخة Proposalriham alrahbiNo ratings yet
- Risk Factors of Hypertension in The ElderlyDocument7 pagesRisk Factors of Hypertension in The ElderlyMashar yonoNo ratings yet
- Lifestyle Diseases Affecting The Nursing Faculty at Tarlac State University During Covid 19 PandemicDocument71 pagesLifestyle Diseases Affecting The Nursing Faculty at Tarlac State University During Covid 19 PandemicDeinielle Magdangal RomeroNo ratings yet
- Bagian 3Document11 pagesBagian 3DheaNo ratings yet
- ijph-68-1606137Document11 pagesijph-68-1606137Karuna PrasanthNo ratings yet
- Good Paper KAP Cut Off Two LevelsDocument18 pagesGood Paper KAP Cut Off Two LevelsSiti Hadijah Aspan, M.PHNo ratings yet
- Unit 2 HS 3310 Epidemiology Written AssignmentDocument5 pagesUnit 2 HS 3310 Epidemiology Written AssignmentBen ObiNo ratings yet
- Resume Jurnal AKLDocument8 pagesResume Jurnal AKLLenggogeni HumairaNo ratings yet
- CVD lancet paperDocument15 pagesCVD lancet paperChilshu ChandranNo ratings yet
- ArunachalamDocument84 pagesArunachalamLAXMI DEVINo ratings yet
- Artikel Jkep Mei 2020-Putu, Jathu, DitaDocument13 pagesArtikel Jkep Mei 2020-Putu, Jathu, DitaDita SulistyowatiNo ratings yet
- Geldsetzer2018 HPDocument10 pagesGeldsetzer2018 HPzeenat04hashmiNo ratings yet
- Pa Nag Iot Akos 2015Document7 pagesPa Nag Iot Akos 2015Gabriel ParizotoNo ratings yet
- Readmissions Final ReportDocument46 pagesReadmissions Final ReportRiki Permana PutraNo ratings yet
- Jurnal Keakuratan Lily W 2014Document8 pagesJurnal Keakuratan Lily W 2014Riki Permana PutraNo ratings yet
- Hack Pasword Vba ExcelDocument4 pagesHack Pasword Vba ExcelRiki Permana Putra100% (1)
- (LIT) LS90 LS110 LS160 BrochureDocument20 pages(LIT) LS90 LS110 LS160 BrochureJuan Carlos Reinhold Niembro SuchowitzkiNo ratings yet
- NIH Public Access: Heavy Metals Toxicity and The EnvironmentDocument30 pagesNIH Public Access: Heavy Metals Toxicity and The EnvironmentAliyu AbdulqadirNo ratings yet
- GCC Lab Manual Mahesh Kumar PDFDocument130 pagesGCC Lab Manual Mahesh Kumar PDFMohan ReddyNo ratings yet
- Semi-Detailed Lesson Plan For Grade-7 Mathematics Prepared By: Jennelyn G. Malayno ObjectivesDocument2 pagesSemi-Detailed Lesson Plan For Grade-7 Mathematics Prepared By: Jennelyn G. Malayno Objectivesjennelyn malaynoNo ratings yet
- 253-Falcon 20F-5BR SN 273 N17DQDocument6 pages253-Falcon 20F-5BR SN 273 N17DQteuiragNo ratings yet
- What Are Free Particles in Quantum MechanicsDocument21 pagesWhat Are Free Particles in Quantum MechanicskalshinokovNo ratings yet
- PDF Empowerment Series Psychopathology A Competency Based Assessment Model For Social Workers Susan W Gray Ebook Full ChapterDocument54 pagesPDF Empowerment Series Psychopathology A Competency Based Assessment Model For Social Workers Susan W Gray Ebook Full Chaptersharon.weintraub470100% (3)
- Arts 9 - Q4 - Mod4 - ChoreographyMovementAndGesturesFromWesternClassicalPlaysOperas - v4Document15 pagesArts 9 - Q4 - Mod4 - ChoreographyMovementAndGesturesFromWesternClassicalPlaysOperas - v4Nikko PatunganNo ratings yet
- 7451 Planiseal288 GBDocument4 pages7451 Planiseal288 GBHendyKoNo ratings yet
- KPMG China Pharmaceutical 201106Document62 pagesKPMG China Pharmaceutical 201106merc2No ratings yet
- Kara Resume 2014Document1 pageKara Resume 2014api-248363003No ratings yet
- Improved WoodDocument17 pagesImproved WoodPavo33% (3)
- Lab 3Document23 pagesLab 3RAMESH KUMARNo ratings yet
- Chapter 2 Synchronous MachinespptDocument53 pagesChapter 2 Synchronous MachinespptraygharNo ratings yet
- Project On FacebookDocument12 pagesProject On FacebookKrish ShewaniNo ratings yet
- Advantage Answers File - UNT 2017Document132 pagesAdvantage Answers File - UNT 2017Brandon RogersNo ratings yet
- Sindh Government Promotion RulesDocument41 pagesSindh Government Promotion RulesseoresercherNo ratings yet
- Grade7 Final DemoDocument5 pagesGrade7 Final DemoMarygrace VictorioNo ratings yet
- ICoMaSEdu Paper TemplateDocument6 pagesICoMaSEdu Paper TemplateRusly HidayahNo ratings yet
- Reporting VerbsDocument4 pagesReporting VerbsMaksat AbetayevNo ratings yet
- Disaster Management and Emergency Response Planning (DMERP-01)Document8 pagesDisaster Management and Emergency Response Planning (DMERP-01)Taimoor AhmadNo ratings yet
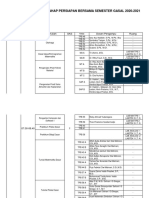
- JADWAL KULIAH TPB SMT GASAL TA 2020 2021 Rev 5Document49 pagesJADWAL KULIAH TPB SMT GASAL TA 2020 2021 Rev 5shin yongriNo ratings yet
- E. B. Magalona National High School Summative Test in CSS 10 Quarter 1 Week 1 Multiple Choice. Choose The Letter of The Correct AnswerDocument2 pagesE. B. Magalona National High School Summative Test in CSS 10 Quarter 1 Week 1 Multiple Choice. Choose The Letter of The Correct Answerric jason pedralNo ratings yet
- Marinediesels - Co.uk - Members Section Starting and Reversing MAN B&W Air Start Distributor OperationDocument2 pagesMarinediesels - Co.uk - Members Section Starting and Reversing MAN B&W Air Start Distributor OperationArun SNo ratings yet
- Brochure UNIPVDocument20 pagesBrochure UNIPVPurushoth KumarNo ratings yet
- Reduction Beta GammaDocument7 pagesReduction Beta GammaBhushan Chaudhary100% (1)
- Practical and Assignment 6Document3 pagesPractical and Assignment 6ioleNo ratings yet
- Global Crisis ManagementDocument8 pagesGlobal Crisis ManagementSantanu Thomas DeyNo ratings yet