Download as pdf or txt
You might also like
- Bikini in 3 - Phase 1Document22 pagesBikini in 3 - Phase 1micheleNo ratings yet
- Cushing's SyndromeDocument35 pagesCushing's SyndromeShankara Pillai100% (3)
- Addison Disease: Diagnosis and Initial ManagementDocument4 pagesAddison Disease: Diagnosis and Initial ManagementTeguh RahNo ratings yet
- The Black Book of TattooingDocument124 pagesThe Black Book of Tattooingmind_warps80% (15)
- N.C Endocrinology (Cushing Syndrome) : Lebanese University Faculty of Public Health 4th BranchDocument12 pagesN.C Endocrinology (Cushing Syndrome) : Lebanese University Faculty of Public Health 4th Branchayah omairiNo ratings yet
- Cushings, Addisons and Acromegaly: DR J Storrow FY2Document38 pagesCushings, Addisons and Acromegaly: DR J Storrow FY2abdalkhalidNo ratings yet
- CushingDocument4 pagesCushingavinash dhameriyaNo ratings yet
- Cushing'S Syndrome: Reported By: Group 4Document37 pagesCushing'S Syndrome: Reported By: Group 4Jovelle AlcantaraNo ratings yet
- Adrenocortical DisordersDocument73 pagesAdrenocortical DisordersReunita ConstantiaNo ratings yet
- Endocrinology Course Content: Semester (5) Clinical Pharmacy CourseDocument91 pagesEndocrinology Course Content: Semester (5) Clinical Pharmacy CourseSadigMukhNo ratings yet
- Cushing's Disease: A Case Presentation of BSN 3YB-7Document69 pagesCushing's Disease: A Case Presentation of BSN 3YB-7MARIA STEPHANY DELA CRUZ100% (1)
- CushingDocument26 pagesCushingAlexSusantoNo ratings yet
- EN8 - HypercortisolismDocument11 pagesEN8 - Hypercortisolismsbobine.imsNo ratings yet
- Cushings SyndromeDocument18 pagesCushings SyndromeBijay SharmaNo ratings yet
- Endocrinology Teaching CasesDocument47 pagesEndocrinology Teaching CasesBinta BaptisteNo ratings yet
- What Is CushingDocument10 pagesWhat Is CushingkuroroexileNo ratings yet
- Referensi Telaah Jurnal Ensefalopati Hipertensi - Dinda Permatasari 11120192124Document2 pagesReferensi Telaah Jurnal Ensefalopati Hipertensi - Dinda Permatasari 11120192124Dinda PermatasariNo ratings yet
- Adrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing SyndromeDocument46 pagesAdrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing Syndromeyuyu tuptupNo ratings yet
- Cushing SyndromeDocument15 pagesCushing Syndromeandrea.maungca.mnlNo ratings yet
- Cushing Syndrome: Clinical ManifestationsDocument4 pagesCushing Syndrome: Clinical ManifestationsMikko Anthony Pingol AlarconNo ratings yet
- Liyon - Endocrine GlandDocument26 pagesLiyon - Endocrine GlandLiyon BasnetNo ratings yet
- AACE Abstracts 2019 Los AngelesDocument357 pagesAACE Abstracts 2019 Los Angelesmimran1974No ratings yet
- Cushing's Syndrome: HypercortisolismDocument22 pagesCushing's Syndrome: HypercortisolismA HNo ratings yet
- Cushing's Syndrome, Addison's Disease and Hyperparathyroidism.Document29 pagesCushing's Syndrome, Addison's Disease and Hyperparathyroidism.pranjl100% (1)
- Anaesthetic Management of Obese PatientDocument53 pagesAnaesthetic Management of Obese PatientpriyadikkalaNo ratings yet
- Group D Case Study Cushing SyndromeDocument6 pagesGroup D Case Study Cushing SyndromeMari IllustriousNo ratings yet
- Cushing SyndromeDocument9 pagesCushing SyndromealyakaramyNo ratings yet
- Tutorial 10 CorticosteroidsDocument16 pagesTutorial 10 CorticosteroidsToqa ElmansouryNo ratings yet
- 40vedant EtalDocument4 pages40vedant EtaleditorijmrhsNo ratings yet
- Progressive Muscle Weakness: More There Than Meets The Eye: Im Board ReviewDocument7 pagesProgressive Muscle Weakness: More There Than Meets The Eye: Im Board Reviewbdalcin5512No ratings yet
- Diagnosis: Cushing's SyndromeDocument3 pagesDiagnosis: Cushing's SyndromeYoga KarsendaNo ratings yet
- Adrenal Insufficiency and Cushing's Disease-1Document34 pagesAdrenal Insufficiency and Cushing's Disease-1Mwanja MosesNo ratings yet
- DKA To CRFDocument4 pagesDKA To CRFMark Anthony YabresNo ratings yet
- Cushing SyndromDocument12 pagesCushing SyndromIka AnisaNo ratings yet
- CusingDocument7 pagesCusingmariahelenaneiNo ratings yet
- 4c Aguilar Gasmen Quitoriano Rabena Valeros Viado VillalobosDocument19 pages4c Aguilar Gasmen Quitoriano Rabena Valeros Viado VillalobosBitz Basos ViadoNo ratings yet
- 30 Manuscript Addison's DiseaseDocument10 pages30 Manuscript Addison's Diseasekint manlangitNo ratings yet
- Group 1 Patho (Rodriguez)Document30 pagesGroup 1 Patho (Rodriguez)Dinarkram Rabreca EculNo ratings yet
- Adrenal InsufficiencyDocument25 pagesAdrenal InsufficiencyMustafa Salam M.NooriNo ratings yet
- Cushing's SyndromeDocument9 pagesCushing's Syndromemuzamiljoyia07No ratings yet
- 28-23 - Cushing Syndrome (Hypercortisolism)Document8 pages28-23 - Cushing Syndrome (Hypercortisolism)Sergio VasquezNo ratings yet
- Causes of Diffuse Hyperpigmentation EndocrinopathiesDocument9 pagesCauses of Diffuse Hyperpigmentation EndocrinopathiesAbdul QuyyumNo ratings yet
- Hypothyroidism: Brief Definition Prevalence Risk FactorsDocument8 pagesHypothyroidism: Brief Definition Prevalence Risk FactorsJennifer BeguinwaNo ratings yet
- Cushing TH 4Document13 pagesCushing TH 4syaymaNo ratings yet
- SC Pediatrics and Review 2014Document5 pagesSC Pediatrics and Review 2014sheyla alegreNo ratings yet
- Cushing's - Syndrome - Nov 2010Document35 pagesCushing's - Syndrome - Nov 2010Jim Jose AntonyNo ratings yet
- Cushings Syndrome: Signs and Symptoms Body System Signs and SymptomsDocument6 pagesCushings Syndrome: Signs and Symptoms Body System Signs and SymptomshappyhappylandNo ratings yet
- CUSHINGDocument12 pagesCUSHINGCarlos alvarezNo ratings yet
- Cushing's Syndrome Is A Disorder That Occurs When Your Body Makes Too Much ofDocument6 pagesCushing's Syndrome Is A Disorder That Occurs When Your Body Makes Too Much ofIra C. SarapatNo ratings yet
- NCMB316 Week 7: Course Unit 6Document5 pagesNCMB316 Week 7: Course Unit 6Armand Bong SantiagoNo ratings yet
- Journal of DiabetesDocument6 pagesJournal of DiabetesSartika Rizky HapsariNo ratings yet
- Ep171905 CRDocument6 pagesEp171905 CRTantri SyahtiraNo ratings yet
- Week 5 Endokrin WO - Michael GeraldilDocument5 pagesWeek 5 Endokrin WO - Michael GeraldilMichael GNo ratings yet
- Cushing's SyndromeDocument4 pagesCushing's SyndromeZainab AliNo ratings yet
- Cushing's SyndromeDocument35 pagesCushing's SyndromeYoga KarsendaNo ratings yet
- Medical Emergencies in Rehabilitation MedicineDocument24 pagesMedical Emergencies in Rehabilitation MedicineAzza El Awar100% (1)
- Nursing Care of Client With Endocrine DisorderDocument93 pagesNursing Care of Client With Endocrine DisorderApril_Anne_Vel_343No ratings yet
- Cushing'S Syndrome: PathophysiologyDocument7 pagesCushing'S Syndrome: PathophysiologyNorsida LailiNo ratings yet
- Stroke Volume Predicts Nocturnal Hypoxemia in The Acute Ischemic Stroke After Intravenous ThrombolysisDocument8 pagesStroke Volume Predicts Nocturnal Hypoxemia in The Acute Ischemic Stroke After Intravenous ThrombolysisPutri Rahmadhani Ngakpaniklage AsdsNo ratings yet
- Journal Reading Neurology - Slide 2Document10 pagesJournal Reading Neurology - Slide 2Putri Rahmadhani Ngakpaniklage AsdsNo ratings yet
- Eath Naphylactic HockDocument15 pagesEath Naphylactic HockPutri Rahmadhani Ngakpaniklage AsdsNo ratings yet
- Mapping Aqsa 1 Jumat 10 MEI 2019Document7 pagesMapping Aqsa 1 Jumat 10 MEI 2019Putri Rahmadhani Ngakpaniklage AsdsNo ratings yet
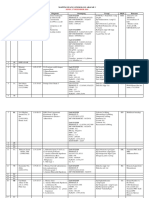
- Mapping Aqsa I Rabu 1 Mei 2019Document6 pagesMapping Aqsa I Rabu 1 Mei 2019Putri Rahmadhani Ngakpaniklage AsdsNo ratings yet
- Stood Ley 2016Document7 pagesStood Ley 2016Putri Rahmadhani Ngakpaniklage AsdsNo ratings yet
- 1 s2.0 S2451993617300890 Main PDFDocument4 pages1 s2.0 S2451993617300890 Main PDFPutri Rahmadhani Ngakpaniklage AsdsNo ratings yet
- Mapping Arafah 2 (Senin, 17 Desember 2018)Document4 pagesMapping Arafah 2 (Senin, 17 Desember 2018)Putri Rahmadhani Ngakpaniklage AsdsNo ratings yet
- The Role of Perceived BarriersDocument12 pagesThe Role of Perceived Barriersrodana100No ratings yet
- Clinical Psychology For Trainees 3rd Ed.Document363 pagesClinical Psychology For Trainees 3rd Ed.saeedz2100% (5)
- Brooks Cole Empowerment Series Becoming An Effective Policy Advocate 7th Edition Jansson Solutions ManualDocument23 pagesBrooks Cole Empowerment Series Becoming An Effective Policy Advocate 7th Edition Jansson Solutions Manualdariusadele6ncs100% (36)
- Allen Medical 2019Document144 pagesAllen Medical 2019Ricardo SalazarNo ratings yet
- Business Ethics Dissertation PDFDocument6 pagesBusiness Ethics Dissertation PDFWriteMyPaperOneDaySingapore100% (1)
- Maitri Anahita - December 2021Document25 pagesMaitri Anahita - December 2021Rock paperNo ratings yet
- 1ST Speaker - Debate Speech - ExampleDocument4 pages1ST Speaker - Debate Speech - ExampleZULAIKHA WIRANo ratings yet
- Introduction To HRMDocument12 pagesIntroduction To HRMmbusa josephNo ratings yet
- Chronic Disease An Economic PerspectiveDocument60 pagesChronic Disease An Economic PerspectiveJiva TuksNo ratings yet
- Polar FA20 User Manual EnglishDocument31 pagesPolar FA20 User Manual EnglishAndrés Cruz RiveraNo ratings yet
- Effect of Pregnancy On Some Hematological and Biochemical Parameters in Pregnant Chinese Water Deer (Hydropotes Inermis)Document9 pagesEffect of Pregnancy On Some Hematological and Biochemical Parameters in Pregnant Chinese Water Deer (Hydropotes Inermis)陳克論No ratings yet
- Clinical Profile of Patients of Central Serous Chorioretinopathy Presented To The Tertiary Health Care CentreDocument4 pagesClinical Profile of Patients of Central Serous Chorioretinopathy Presented To The Tertiary Health Care CentreIJAR JOURNALNo ratings yet
- S2 ReadingDocument2 pagesS2 ReadingHoàng Bùi TânNo ratings yet
- Test Bank For Health Assessment in Nursing 3 Har CDR Edition Janet R WeberDocument36 pagesTest Bank For Health Assessment in Nursing 3 Har CDR Edition Janet R Weberexundateseller.mqr0ps100% (43)
- Classic 120.2 125.2 GERNI ManualDocument26 pagesClassic 120.2 125.2 GERNI Manualbackch9011No ratings yet
- USSEC Aquaculture PDFDocument4 pagesUSSEC Aquaculture PDFLulzim LumiNo ratings yet
- ENEMADocument4 pagesENEMAMariah Alexis EncinaNo ratings yet
- S M A R T: 201 A TEST #3 Define and Discuss The Purpose of Outcome IdentificationDocument6 pagesS M A R T: 201 A TEST #3 Define and Discuss The Purpose of Outcome IdentificationLindsay JonesNo ratings yet
- Abhishek Patil ScopusDocument11 pagesAbhishek Patil ScopussunilNo ratings yet
- Ongoing / Upcoming Activities at Manifa CHF Project: HSE HSEDocument12 pagesOngoing / Upcoming Activities at Manifa CHF Project: HSE HSERahil TasawarNo ratings yet
- Res. No. - Distribution of Hygiene KitsDocument2 pagesRes. No. - Distribution of Hygiene KitsMariel AzonNo ratings yet
- HeavymetalinKelantanRiver PDFDocument20 pagesHeavymetalinKelantanRiver PDFwan marlinNo ratings yet
- AP Psychology Module 66+67Document5 pagesAP Psychology Module 66+67kyuuNo ratings yet
- Factsheet: E-Health in EstoniaDocument2 pagesFactsheet: E-Health in EstoniaNasrullah roslanNo ratings yet
- Violation of Children's RightsDocument2 pagesViolation of Children's RightsAna Matilde De Lavalle De La CruzNo ratings yet
- FTC Complaint On Novant Health Acquisition AgreementDocument20 pagesFTC Complaint On Novant Health Acquisition AgreementEmma KoryntaNo ratings yet
- 110-Article Text-249-1-10-20210509Document10 pages110-Article Text-249-1-10-20210509Elizabethan VictoriaNo ratings yet
- Full Chapter The Vaccine Book 2Nd Edition Barry R Bloom PDFDocument53 pagesFull Chapter The Vaccine Book 2Nd Edition Barry R Bloom PDFroy.rowland894100% (2)