Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- IPAQ SFScoringDocument5 pagesIPAQ SFScoringmolen67% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Personal StatementDocument2 pagesPersonal StatementSabha RabayaNo ratings yet
- Sindrom ChoreaDocument12 pagesSindrom ChoreamolenNo ratings yet
- Dopamed - Id Atrialfibrillation Handout PDFDocument12 pagesDopamed - Id Atrialfibrillation Handout PDFmolenNo ratings yet
- PatofisiologiDocument4 pagesPatofisiologimolenNo ratings yet
- Management of Edema in Nephrotic Syndrome PDFDocument10 pagesManagement of Edema in Nephrotic Syndrome PDFmolenNo ratings yet
- Preterm+Prelabour+Rupture+of+the+Membranes Sept2015Document12 pagesPreterm+Prelabour+Rupture+of+the+Membranes Sept2015molenNo ratings yet
- PDFDocument3 pagesPDFmolenNo ratings yet
- Kuliah Mineral 2015-2016Document20 pagesKuliah Mineral 2015-2016molenNo ratings yet
- Nephrotic Syndrome in Children: January 2013Document7 pagesNephrotic Syndrome in Children: January 2013molenNo ratings yet
- List Game Software Film 1Document304 pagesList Game Software Film 1molenNo ratings yet
- Acute Abdomen - Block Emergency: DR Ruankha SpbaDocument24 pagesAcute Abdomen - Block Emergency: DR Ruankha SpbamolenNo ratings yet
- Preconception Care Presentation SlidesDocument15 pagesPreconception Care Presentation SlidesLucy AsconaNo ratings yet
- Pemeriksaan Terkini Hepatitis Virus: Prof. Dr. Jusak Nugraha, DR, MS, SPPK (K) Lab Patologi Klinik FK UnairDocument53 pagesPemeriksaan Terkini Hepatitis Virus: Prof. Dr. Jusak Nugraha, DR, MS, SPPK (K) Lab Patologi Klinik FK UnairMuh YunusNo ratings yet
- BRVO PPT by Dr. Chinmay KharadeDocument31 pagesBRVO PPT by Dr. Chinmay KharadeChinmay KharadeNo ratings yet
- Biochem Nucleic Acid ReviewerDocument5 pagesBiochem Nucleic Acid ReviewerGabrielle FranciscoNo ratings yet
- What Is Canavan BrochureDocument4 pagesWhat Is Canavan BrochureYamihush MuthuKumarNo ratings yet
- Achalasia: An Overview of Diagnosis and Treatment: ReviewDocument14 pagesAchalasia: An Overview of Diagnosis and Treatment: ReviewHarliaNo ratings yet
- Nsth06 22.Rs - BalgirDocument16 pagesNsth06 22.Rs - Balgirjeyakar.mz8442No ratings yet
- Classification of Veneer PreparationsDocument11 pagesClassification of Veneer PreparationsVinisha Vipin SharmaNo ratings yet
- APNC 520 Exam 10 Study Guide Musculoskeletal DisordersDocument15 pagesAPNC 520 Exam 10 Study Guide Musculoskeletal DisordersMariaNo ratings yet
- Molecular Diagnostics Proposal: International University-Vietnam National University School of BiotechnologyDocument27 pagesMolecular Diagnostics Proposal: International University-Vietnam National University School of BiotechnologyGia HoàngNo ratings yet
- StsDocument3 pagesStsAvarosa100% (1)
- Nervous System Lab ReportDocument6 pagesNervous System Lab Reportapi-269993638No ratings yet
- Full Chapter The Zebrafish Cellular and Developmental Biology Part B Developmental Biology 4Th Edition H William Detrich PDFDocument64 pagesFull Chapter The Zebrafish Cellular and Developmental Biology Part B Developmental Biology 4Th Edition H William Detrich PDFjoseph.wright687100% (6)
- Stop AIDS. Keep The Promise.: L'Automédicat-ion Au Liban NordDocument13 pagesStop AIDS. Keep The Promise.: L'Automédicat-ion Au Liban Nordhussein bitarNo ratings yet
- Please Write Your Answer Briefly and ConciselyDocument7 pagesPlease Write Your Answer Briefly and ConciselyFRISKA CHRISTININGRUMNo ratings yet
- Outcome of Treatment in Adults With Acute Lymphoblastic Leukemia: Analysis of The LALA-94 TrialDocument22 pagesOutcome of Treatment in Adults With Acute Lymphoblastic Leukemia: Analysis of The LALA-94 TrialJoseph TheThirdNo ratings yet
- Biotehnologija GMO RegulativaDocument39 pagesBiotehnologija GMO RegulativaTatjana MarinkovicNo ratings yet
- KP Burning Mouth SyndromeDocument23 pagesKP Burning Mouth SyndromemuhammadNo ratings yet
- Asfa 2013Document140 pagesAsfa 2013bib22No ratings yet
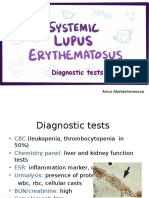
- PBL 3 - SLE (Diagnostic Tests)Document9 pagesPBL 3 - SLE (Diagnostic Tests)Ainur AbdrakhmanovaNo ratings yet
- Silk'n Lipo - Clinical OverviewDocument10 pagesSilk'n Lipo - Clinical OverviewFit BoxxNo ratings yet
- Entrance Exam Hema WITH ANSWERSDocument7 pagesEntrance Exam Hema WITH ANSWERSReda SoNo ratings yet
- ForteBio App Note 1Document2 pagesForteBio App Note 1Fernando OviedoNo ratings yet
- MG PosterDocument1 pageMG PosterNataShini RajaRatnamNo ratings yet
- Genetics 2581 OutlineDocument35 pagesGenetics 2581 OutlineBhawaniJainNo ratings yet
- OSCE in Pediatrics, 2011Document267 pagesOSCE in Pediatrics, 2011floare de colt0% (1)
- Health: Fat-Soluble Vitamins No. 9.315Document4 pagesHealth: Fat-Soluble Vitamins No. 9.315Jade Kenneth Gonzales LomansocNo ratings yet
- Nucleic Acids 2015Document72 pagesNucleic Acids 2015meh100% (1)
- The Origins of Individualized Vitamin D3 Therapy For MSDocument1 pageThe Origins of Individualized Vitamin D3 Therapy For MSIon PopaNo ratings yet