Download as pdf or txt
You might also like
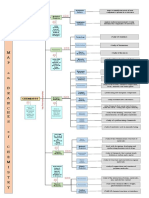
- Concept MapDocument1 pageConcept MapLesley Joy T. BaldonadoNo ratings yet
- Cohen, R., & Velho, V. Update On Respiratory Disease From Coal Mine and Silica DustDocument16 pagesCohen, R., & Velho, V. Update On Respiratory Disease From Coal Mine and Silica DustAlekseiNo ratings yet
- Hnizdo 2003Document8 pagesHnizdo 2003Dang QuanNo ratings yet
- Coal Workers' Pneumoconiosis (Black Lung Disease) - Practice Essentials, Pathophysiology, EtiologyDocument7 pagesCoal Workers' Pneumoconiosis (Black Lung Disease) - Practice Essentials, Pathophysiology, EtiologyامينNo ratings yet
- Gabungan Jurnal Pertambangan Andini Desti AmaliaDocument16 pagesGabungan Jurnal Pertambangan Andini Desti AmaliaIndri KusmawatiNo ratings yet
- Contribution of Air Pollution To COPD and Small Airway DysfunctionDocument8 pagesContribution of Air Pollution To COPD and Small Airway DysfunctionWahyuNo ratings yet
- Coal Workers' Lung Diseases: Attfield, Michael D. Petsonk, Edward L. Wagner, Gregory RDocument5 pagesCoal Workers' Lung Diseases: Attfield, Michael D. Petsonk, Edward L. Wagner, Gregory Rdwi rahwatiNo ratings yet
- Nihms 1066509Document21 pagesNihms 1066509Vostie1811No ratings yet
- Coal Worker PneumoconiosisDocument10 pagesCoal Worker Pneumoconiosisdrmohamed2017No ratings yet
- Original ContributionDocument10 pagesOriginal Contributionelisabeth apriliaNo ratings yet
- Scientific Evidence of Health Effects From Coal Use in Energy GenerationDocument18 pagesScientific Evidence of Health Effects From Coal Use in Energy GenerationAlejandraNo ratings yet
- Mortality in Miners With Coal-Workers PneumoconioDocument12 pagesMortality in Miners With Coal-Workers PneumoconiometaNo ratings yet
- Liu2020 REDACCION 1Document18 pagesLiu2020 REDACCION 1LUIS ANGEL MEZA PEREZNo ratings yet
- Part A-12-Wood Dust Allergies - Q&ADocument8 pagesPart A-12-Wood Dust Allergies - Q&Afernanda1rondelliNo ratings yet
- Coal Worker'S Pneumoconiosis: (Artikel Review)Document11 pagesCoal Worker'S Pneumoconiosis: (Artikel Review)dicky rhestuNo ratings yet
- Nickel CarcinogenesisDocument31 pagesNickel CarcinogenesisIvan SotoNo ratings yet
- Pulmonary Aspects of Nitrogen Dioxide Toxicity: J.B. Buick, R.C. Lowry, T.R.A. MageeDocument9 pagesPulmonary Aspects of Nitrogen Dioxide Toxicity: J.B. Buick, R.C. Lowry, T.R.A. MageeJason PacilNo ratings yet
- Occupational Silica Exposure and Risk of Various Diseases: An Analysis Using Death Certificates From 27 States of The United StatesDocument9 pagesOccupational Silica Exposure and Risk of Various Diseases: An Analysis Using Death Certificates From 27 States of The United StatesDang QuanNo ratings yet
- Occupational Health Aspects of Quartz in Bituminous Coal Fly Ash in Israel 2009Document21 pagesOccupational Health Aspects of Quartz in Bituminous Coal Fly Ash in Israel 2009Rani Nasrasyam ZalmaNo ratings yet
- Cardiovascular Effects of Particulate Air PollutionDocument16 pagesCardiovascular Effects of Particulate Air Pollutionpao.pearanda1998No ratings yet
- Sílica e Cancer HSE UKDocument86 pagesSílica e Cancer HSE UKAirton MarinhoNo ratings yet
- Environmental Research: Jimyung Park, Hyung-Jun Kim, Chang-Hoon Lee, Chang Hyun Lee, Hyun Woo LeeDocument8 pagesEnvironmental Research: Jimyung Park, Hyung-Jun Kim, Chang-Hoon Lee, Chang Hyun Lee, Hyun Woo LeeJoaquim Lorenzetti BrancoNo ratings yet
- Fpubh 10 882569Document13 pagesFpubh 10 882569Katalin BodorNo ratings yet
- Work-Related Chronic Obstructive Pulmonary Disease (COPD) Statistics in Great Britain, 2020Document7 pagesWork-Related Chronic Obstructive Pulmonary Disease (COPD) Statistics in Great Britain, 2020Maral GanbilegNo ratings yet
- Chapter 18 - Carcinogenicity of Metal Co - 2015 - Handbook On The Toxicology ofDocument28 pagesChapter 18 - Carcinogenicity of Metal Co - 2015 - Handbook On The Toxicology ofChanWingSanNo ratings yet
- 501 981 2 PB PDFDocument8 pages501 981 2 PB PDFReyza HasnyNo ratings yet
- Silicosis in Artificial Stone Workers: Spectrum of Radiological High-Resolution CT Chest FindingsDocument9 pagesSilicosis in Artificial Stone Workers: Spectrum of Radiological High-Resolution CT Chest FindingsFabio GigliottiNo ratings yet
- Critical Review: Metals in Cigarette SmokeDocument5 pagesCritical Review: Metals in Cigarette Smokemia palacioNo ratings yet
- CoalDocument8 pagesCoalFA MonsterNo ratings yet
- Miners' PhthisisDocument17 pagesMiners' PhthisisTom MillerNo ratings yet
- Caramori 2019Document16 pagesCaramori 2019Dusan MilovanovicNo ratings yet
- Foy Et Al 2012Document8 pagesFoy Et Al 2012Usman AliNo ratings yet
- Air Pullution and Liver CancerDocument10 pagesAir Pullution and Liver CancerjuanNo ratings yet
- Silica Silicosis TuberculosisDocument11 pagesSilica Silicosis TuberculosisAndrewNo ratings yet
- Faculty of Technology: ReportDocument13 pagesFaculty of Technology: ReportAsmi SyamimNo ratings yet
- Molhave 1997Document14 pagesMolhave 1997VISHALNo ratings yet
- DidiDocument12 pagesDidiAndreea DamianNo ratings yet
- Air Pollution As An Early Determinant of COPD: Zhuyi Lu, Patrice Coll, Bernard Maitre, Ralph Epaud and Sophie LanoneDocument13 pagesAir Pollution As An Early Determinant of COPD: Zhuyi Lu, Patrice Coll, Bernard Maitre, Ralph Epaud and Sophie LanoneywtmyxpezickztrkcfNo ratings yet
- Exposure To Metal Welding Fume Particles and Risk For Cardiovascular Disease in Denmark: A Prospective Cohort StudyDocument7 pagesExposure To Metal Welding Fume Particles and Risk For Cardiovascular Disease in Denmark: A Prospective Cohort StudyseliNo ratings yet
- COLE-HUNTER Long Term Air PollutionDocument10 pagesCOLE-HUNTER Long Term Air PollutionPaula VasconcellosNo ratings yet
- Urban Air Quality and Health - Two Steps Forward, One Step Back 2019Document3 pagesUrban Air Quality and Health - Two Steps Forward, One Step Back 2019Micaela RusñakNo ratings yet
- EScholarship UC Item 0fq156mxDocument11 pagesEScholarship UC Item 0fq156mxDian MaulidaNo ratings yet
- Lung ConsolidationDocument7 pagesLung ConsolidationpaulNo ratings yet
- OccupationalDocument145 pagesOccupationalpaulNo ratings yet
- Pneumoconiosis: Name and SynonymsDocument17 pagesPneumoconiosis: Name and Synonymsgasai gasaiNo ratings yet
- Research Article Exposure To Air Pollution Exacerbates Inflammation in Rats With Preexisting COPDDocument12 pagesResearch Article Exposure To Air Pollution Exacerbates Inflammation in Rats With Preexisting COPDĐạt NguyễnNo ratings yet
- Occupational Lung DiseasesDocument14 pagesOccupational Lung DiseasesEgy BagusNo ratings yet
- COPD Emphysema and The Onset of Lung Cancer A Systematic - 2016 - Cancer LetteDocument5 pagesCOPD Emphysema and The Onset of Lung Cancer A Systematic - 2016 - Cancer Lettegacclogin1989No ratings yet
- Pollution and Respiratory Disease: Can Diet or Supplements Help? A ReviewDocument14 pagesPollution and Respiratory Disease: Can Diet or Supplements Help? A ReviewEgy SunandaNo ratings yet
- Covid 19 and Ozone 65-372Document8 pagesCovid 19 and Ozone 65-372Iurydouglas AcioleNo ratings yet
- Clinical Respiratory J - 2017 - Sarkar - Tuberculosis Associated Chronic Obstructive Pulmonary DiseaseDocument11 pagesClinical Respiratory J - 2017 - Sarkar - Tuberculosis Associated Chronic Obstructive Pulmonary DiseaseAgatha GeraldyneNo ratings yet
- Occupation As A Risk Factor of Small Cell Lung Cancer: Scientific Reports - (2023) 13:4727Document7 pagesOccupation As A Risk Factor of Small Cell Lung Cancer: Scientific Reports - (2023) 13:4727wulanesterNo ratings yet
- Fan Y 2020 Association of Occupational Dust Exposure With Combined Chronic Obstructive Pulmonary Disease and PneumoconiosisDocument10 pagesFan Y 2020 Association of Occupational Dust Exposure With Combined Chronic Obstructive Pulmonary Disease and PneumoconiosisVostie1811No ratings yet
- FORO 2 - Exposición Ocupacional Al Polvo de Sílice y Riesgo de Cáncer de Pulmón, Un Metanálisis Actualizado de Estudios EpidemiológicosDocument17 pagesFORO 2 - Exposición Ocupacional Al Polvo de Sílice y Riesgo de Cáncer de Pulmón, Un Metanálisis Actualizado de Estudios EpidemiológicosRoberto GonzalesNo ratings yet
- Biomedical Journal: SciencedirectDocument22 pagesBiomedical Journal: SciencedirectmsdhaniaNo ratings yet
- Beryllium: Handbook On The Toxicology of Metals 4EDocument19 pagesBeryllium: Handbook On The Toxicology of Metals 4EChanWingSanNo ratings yet
- Paper 2 PDFDocument18 pagesPaper 2 PDFShailendra TripathiNo ratings yet
- Indoor Air - 2021 - Andersen - Emissions of Soot PAHs Ultrafine Particles NOx and Other Health Relevant Compounds FromDocument16 pagesIndoor Air - 2021 - Andersen - Emissions of Soot PAHs Ultrafine Particles NOx and Other Health Relevant Compounds Fromnathalia.talinho2No ratings yet
- A Systematic Review of Cytogenetic Studies Conducted in Human Populations Exposed To Cadmium CompoundsDocument29 pagesA Systematic Review of Cytogenetic Studies Conducted in Human Populations Exposed To Cadmium CompoundsSabiho GinoNo ratings yet
- F. Analytical Methods For The Study of Air Pollution (Uvod, Ist Monit Lon Anal Metode Za Nox I So2)Document11 pagesF. Analytical Methods For The Study of Air Pollution (Uvod, Ist Monit Lon Anal Metode Za Nox I So2)Ivana BanićevićNo ratings yet
- Schmeling - The Role of Hydrothermal Cooling of The Oceanic Lithosphere For Ocean Floor Bathymetry 2017Document19 pagesSchmeling - The Role of Hydrothermal Cooling of The Oceanic Lithosphere For Ocean Floor Bathymetry 2017utsav mannuNo ratings yet
- 01 Atomic Structures WSDocument34 pages01 Atomic Structures WSAreeba EjazNo ratings yet
- E M II: Synchronous MachineDocument10 pagesE M II: Synchronous MachineAkashman ShakyaNo ratings yet
- Will or Going To 90069Document2 pagesWill or Going To 90069Dragana ZafirovskaNo ratings yet
- Arturo Pomar by Bill Wall: Maestros (Pomar, My 50 Games With Masters) - Pomar Was Only 14 at TheDocument3 pagesArturo Pomar by Bill Wall: Maestros (Pomar, My 50 Games With Masters) - Pomar Was Only 14 at TheKartik ShroffNo ratings yet
- Justin Bieber Is - Famous Singer.: (You Must Read Out The Whole Sentence.)Document2 pagesJustin Bieber Is - Famous Singer.: (You Must Read Out The Whole Sentence.)Irene De la FuenteNo ratings yet
- Break Even AnalysisDocument18 pagesBreak Even AnalysisSMHE100% (10)
- Tools, Materials and Equipment in Nail Care: Learning Activity Sheet Week 1 Quarter 1Document8 pagesTools, Materials and Equipment in Nail Care: Learning Activity Sheet Week 1 Quarter 1Barbara PosoNo ratings yet
- Cubicost Tas & TRB Elementary Quiz - AnswerDocument9 pagesCubicost Tas & TRB Elementary Quiz - AnswerChee HernNo ratings yet
- How To Retract BPS Data Back To R3 When There Is No Standard RetractorDocument3 pagesHow To Retract BPS Data Back To R3 When There Is No Standard Retractorraphavega2010No ratings yet
- Barcode Scanner, Wireless Barcode Scanner, DC5112 Barcode ScannerDocument3 pagesBarcode Scanner, Wireless Barcode Scanner, DC5112 Barcode ScannerdcodeNo ratings yet
- L2 - Cryptococcus NeoformansDocument44 pagesL2 - Cryptococcus Neoformansdvph2fck6qNo ratings yet
- World Red Cross DayDocument17 pagesWorld Red Cross DayAshwani K SharmaNo ratings yet
- RUNET BETONexpress v21Document2 pagesRUNET BETONexpress v21Angeles Juliana MorenoNo ratings yet
- Assignment 11 STM DavisDocument8 pagesAssignment 11 STM Davisrajesh laddhaNo ratings yet
- Hot Vs Cold Lab Lesson PlanDocument4 pagesHot Vs Cold Lab Lesson Planapi-497020000No ratings yet
- ICH Quality Guidelines - AnuragDocument4 pagesICH Quality Guidelines - AnuragAnurag BhardwajNo ratings yet
- Agent ListDocument23 pagesAgent ListMayuresh ShakyawarNo ratings yet
- Paper 3 On Stan LeeDocument5 pagesPaper 3 On Stan Leeapi-545773326No ratings yet
- Introduction To The Ibm Dataops Methodology and PracticeDocument30 pagesIntroduction To The Ibm Dataops Methodology and PracticeGriseldaNo ratings yet
- Adavantages of Historical ResearchDocument2 pagesAdavantages of Historical ResearchClemence JeniferNo ratings yet
- ISquare - Setup Guide For Fresh UsersDocument12 pagesISquare - Setup Guide For Fresh UsersWQDNo ratings yet
- 25 Duas From The Holy QuranDocument4 pages25 Duas From The Holy QuranKhan Amir Younus KamalNo ratings yet
- Basket 1159913 DataDocument13 pagesBasket 1159913 DataMartin SuchomelNo ratings yet
- Book SoftDocument318 pagesBook SoftBrian Takudzwa MuzembaNo ratings yet
- The Art of Perfumery-Septimus PiesseDocument431 pagesThe Art of Perfumery-Septimus PiesseHornoEnElNo ratings yet
- CHAVEZ 2017 Data Driven Supply Chains Manufacturing Capability and Customer SatisfactionDocument14 pagesCHAVEZ 2017 Data Driven Supply Chains Manufacturing Capability and Customer SatisfactionRodolfo StraussNo ratings yet
- EPM-1183 Ethics, Code of Conduct & Professional PracticeDocument41 pagesEPM-1183 Ethics, Code of Conduct & Professional PracticeDev ThackerNo ratings yet
- Petition For Writ of Kalikasan (Marj)Document4 pagesPetition For Writ of Kalikasan (Marj)Myka FloresNo ratings yet