
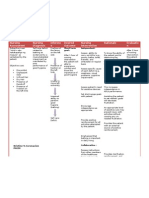
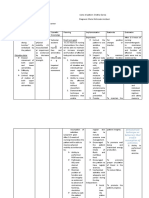
III. Nursing Care Plan: Assessment Diagnosis Goal Intervention Evaluation
III. Nursing Care Plan: Assessment Diagnosis Goal Intervention Evaluation
You might also like
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- Cerebrovascular Accident Nursing Care PlanDocument4 pagesCerebrovascular Accident Nursing Care PlanCyrus De Asis67% (12)
- NCP GunshotDocument13 pagesNCP GunshotMichael John F. Natividad0% (1)
- Discharge PlanningDocument5 pagesDischarge PlanningNoora KhalidNo ratings yet
- Ischemic Stroke NCPDocument11 pagesIschemic Stroke NCPJohannah DaroNo ratings yet
- Nursing Care Plan (ImpairedphyssicalDocument5 pagesNursing Care Plan (ImpairedphyssicalkuroroexileNo ratings yet
- NCP #1 Ineffective Cerebral Tissue PerfusionDocument4 pagesNCP #1 Ineffective Cerebral Tissue PerfusionsteffiNo ratings yet
- NCP Ineffective Cerebral Tissue PerfusionDocument2 pagesNCP Ineffective Cerebral Tissue PerfusionAngelo ︻╦̵̵͇̿̿̿̿╤── Bulacan50% (6)
- Anatomy and Physiology of CVADocument4 pagesAnatomy and Physiology of CVAKimsha ConcepcionNo ratings yet
- Nursing Care Plan Hemorrhagic StrokeDocument8 pagesNursing Care Plan Hemorrhagic StrokeJeffrey Dela Cruz50% (4)
- Impaired Verbal CommunicationDocument3 pagesImpaired Verbal CommunicationDesiree Deleon Guerrero0% (2)
- Impaired Verbal CommunicationDocument1 pageImpaired Verbal Communicationdana100% (3)
- Nursing Care Plan: Subjective: Short Term Goal: Independent: Short Term GoalDocument1 pageNursing Care Plan: Subjective: Short Term Goal: Independent: Short Term GoalDante Sales75% (4)
- Pathophysiology CVADocument2 pagesPathophysiology CVASewyel Garburi100% (6)
- "Mayroong Namuong Dugo Sa Utak Niya Kaya Hindi Maayos Ang Daloy NG Dugo Rito" As Verbalized by The Patient'sDocument4 pages"Mayroong Namuong Dugo Sa Utak Niya Kaya Hindi Maayos Ang Daloy NG Dugo Rito" As Verbalized by The Patient'sAllisson BeckersNo ratings yet
- Case Study EsrdDocument4 pagesCase Study EsrdSTEPHANIE JOSUENo ratings yet
- NCP For Impaired Physical MobilityDocument2 pagesNCP For Impaired Physical MobilityPrincess Averin Navarro50% (2)
- NCP CvaDocument4 pagesNCP CvamannyV1990100% (1)
- NCPDocument2 pagesNCPLyka Mae Imbat - PacnisNo ratings yet
- NCP - Tissue Perfusion (Cerebral)Document2 pagesNCP - Tissue Perfusion (Cerebral)moodlayers50% (6)
- NCP 1: Ineffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Cerebrovascular AccidentDocument14 pagesNCP 1: Ineffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Cerebrovascular AccidentKyle Jingco100% (2)
- Ineffective Tissue PerfusionDocument1 pageIneffective Tissue PerfusionEm Castillo50% (2)
- CVA-NCPDocument7 pagesCVA-NCPAiza Oronce0% (1)
- Ineffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7Document2 pagesIneffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7dana100% (4)
- Nursing Care Plan SeizureDocument2 pagesNursing Care Plan Seizuretimie_reyes100% (1)
- Nursing Care Plan (CVA)Document2 pagesNursing Care Plan (CVA)Mel Rodolfo50% (2)
- NCP For StrokeDocument4 pagesNCP For StrokeJASON OGALESCO100% (1)
- Self Care Deficit BahtingDocument1 pageSelf Care Deficit BahtingNaj SoliveresNo ratings yet
- Self Care DeficitDocument2 pagesSelf Care DeficitSj 斗力上75% (4)
- NCP CVA Impaired Physical Mobility 1Document2 pagesNCP CVA Impaired Physical Mobility 1Frency Anne Causo Pascual100% (1)
- NCP NeuroDocument20 pagesNCP NeuroNica Gaborne Navarro100% (3)
- CVA Activity IntoleranceDocument1 pageCVA Activity IntoleranceNursesLabs.com75% (4)
- NCP - Altered Tissue PerfusionDocument2 pagesNCP - Altered Tissue PerfusionLeigh Kristel Andrion0% (1)
- IMPAIRED PHYSICAL MOBILITY RT Neuromuscular Involvement (Right Sided Paresthesia Aeb Inability To Purposefully Move Body Parts.Document2 pagesIMPAIRED PHYSICAL MOBILITY RT Neuromuscular Involvement (Right Sided Paresthesia Aeb Inability To Purposefully Move Body Parts.Senyorita KHaye67% (3)
- Impaired Verbal CommunicationDocument3 pagesImpaired Verbal CommunicationCalimlim KimNo ratings yet
- NCP CvaDocument3 pagesNCP CvaJey PangilinanNo ratings yet
- Self Care DeficitDocument3 pagesSelf Care DeficitAddie Labitad100% (2)
- NCP Fracture Risk For InfectionDocument3 pagesNCP Fracture Risk For InfectionMiggsNo ratings yet
- Impaired Verbal CommunicationDocument2 pagesImpaired Verbal CommunicationEjay Barayuga100% (2)
- NCP - OsteosarcomaDocument5 pagesNCP - OsteosarcomaNelson Lacsamana100% (1)
- Post Open Reduction Internal Fixation PathophysiologyDocument3 pagesPost Open Reduction Internal Fixation PathophysiologyRizalyn QuindipanNo ratings yet
- Clonidine HydrochlorideDocument1 pageClonidine HydrochlorideLovelyn Joy Abubo CortezNo ratings yet
- Assessment Nursing Diagnosis Planning Implemantation Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Planning Implemantation Rationale EvaluationChloie Marie Rosalejos100% (1)
- NCP - Impaired Verbal Communication Related To Neuromascular Impairment As Manifested by AphaisaDocument2 pagesNCP - Impaired Verbal Communication Related To Neuromascular Impairment As Manifested by AphaisaKristina Angela CarbonNo ratings yet
- Nursing Care Plan CVADocument6 pagesNursing Care Plan CVAessevyNo ratings yet
- 14 Cerebrovascular Accident Nursing Care PlansDocument5 pages14 Cerebrovascular Accident Nursing Care PlansNickesha Mckenzie75% (4)
- NCP For CVADocument18 pagesNCP For CVAmolukas101100% (7)
- Stroke Nursing Care PlanDocument1 pageStroke Nursing Care PlanTracy Pearl100% (1)
- NCP - BedriddenDocument4 pagesNCP - Bedriddenadelaigner_racho589475% (4)
- NCP - Knowledge Deficit (Acromegaly)Document3 pagesNCP - Knowledge Deficit (Acromegaly)Kian HerreraNo ratings yet
- Spina Bifida NCPDocument3 pagesSpina Bifida NCPShahzad GulfamNo ratings yet
- JMJ Marist Brothers Notre Dame of Marbel University College of Arts and Sciences - Nursing Department Alunan Avenue, Koronadal City, South CotabatoDocument4 pagesJMJ Marist Brothers Notre Dame of Marbel University College of Arts and Sciences - Nursing Department Alunan Avenue, Koronadal City, South CotabatoJullie AgredaNo ratings yet
- Gout N C P BY BHERU LALDocument1 pageGout N C P BY BHERU LALBheru LalNo ratings yet
- Nursing Care Plan-1 Age: 50Y Medical Diagnoses: Fracture Assessment Nursing Diagnosis Planning Intervention Scientific Rationale EvaluationDocument2 pagesNursing Care Plan-1 Age: 50Y Medical Diagnoses: Fracture Assessment Nursing Diagnosis Planning Intervention Scientific Rationale EvaluationBheru LalNo ratings yet
- Case IcuDocument5 pagesCase IcuTrisha SuazoNo ratings yet
- Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective: "Maglisod Man Kog Short Term: Independent: - Establish RapportDocument3 pagesAssessment Diagnosis Planning Interventions Rationale Evaluation Subjective: "Maglisod Man Kog Short Term: Independent: - Establish RapportSergi Lee OrateNo ratings yet
- Activity IntoleranceDocument3 pagesActivity IntoleranceRaidis PangilinanNo ratings yet
- Cva NCP 1Document3 pagesCva NCP 1MarcieNo ratings yet
- NCP of Impaired MobilityDocument3 pagesNCP of Impaired MobilityHazel Cabrera0% (1)
- Assessment Diagnosis Scientific Explanation Planning Interventions Rationale Expected Outcome Subjective: O Short Term: Short TermDocument3 pagesAssessment Diagnosis Scientific Explanation Planning Interventions Rationale Expected Outcome Subjective: O Short Term: Short TermRaidis PangilinanNo ratings yet
- Subjective Data: Short Term Goal: Independent: 1. Monitor Patient's Vital Signs. 2. Determine Diagnosis That Short Term GoalDocument3 pagesSubjective Data: Short Term Goal: Independent: 1. Monitor Patient's Vital Signs. 2. Determine Diagnosis That Short Term GoalGeralyn KaeNo ratings yet
- Josue, Stephanie Canlas Batch 51 Reaction Paper Respiratory FailureDocument1 pageJosue, Stephanie Canlas Batch 51 Reaction Paper Respiratory FailureSTEPHANIE JOSUENo ratings yet
- Esrd Diagram PathophysiologyDocument3 pagesEsrd Diagram PathophysiologySTEPHANIE JOSUE100% (1)
- Esrd PathophysiologyDocument1 pageEsrd PathophysiologySTEPHANIE JOSUENo ratings yet
- Nuclear Medicine Technician or MedicalDocument2 pagesNuclear Medicine Technician or Medicalapi-79207760No ratings yet
- Trauma-Sensitive Yoga - Principles, Practice and ResearchDocument6 pagesTrauma-Sensitive Yoga - Principles, Practice and ResearchRichard Guerra100% (1)
- Just Another Sebaceous Cyst?: I. Clinical QuestionDocument3 pagesJust Another Sebaceous Cyst?: I. Clinical QuestionJaessa FelicianoNo ratings yet
- Cochlear-Implants Brochure 2Document2 pagesCochlear-Implants Brochure 2roroNo ratings yet
- Dr. Ashman's ENT Notes PDFDocument56 pagesDr. Ashman's ENT Notes PDFJulian GordonNo ratings yet
- Antibiotic Resistance: Key PointsDocument7 pagesAntibiotic Resistance: Key Pointsgeorgi.annaNo ratings yet
- Lilyasari2019 Article EconomicEvaluationOfSildenafilDocument9 pagesLilyasari2019 Article EconomicEvaluationOfSildenafilNajib Al FatinNo ratings yet
- History of Present IllnessDocument4 pagesHistory of Present Illnessegabe386No ratings yet
- Reading 5 Blood and Body DefensesDocument18 pagesReading 5 Blood and Body Defenseslephuongvy1406No ratings yet
- AntiemeticsDocument33 pagesAntiemeticsSaiNo ratings yet
- BLSPPT 180126100212 PDFDocument58 pagesBLSPPT 180126100212 PDFJerwynn Ilustre100% (1)
- Complex Regional Pain SyndromeDocument10 pagesComplex Regional Pain SyndromegeejeiNo ratings yet
- Physical TherapyDocument11 pagesPhysical TherapyEvelyn MedinaNo ratings yet
- Dissertation SalmonellaDocument7 pagesDissertation SalmonellaWriteMyPaperCoCanada100% (1)
- PANBIO IgM MAC ELISADocument5 pagesPANBIO IgM MAC ELISAmiss.JEJENo ratings yet
- Case Study 1Document9 pagesCase Study 1andry natanel tonyNo ratings yet
- TEP Jama 2022Document10 pagesTEP Jama 2022carla jazmin cortes rodriguezNo ratings yet
- Burns E 2013 PHD Thesis PDFDocument338 pagesBurns E 2013 PHD Thesis PDFDr-Rabia AlmamalookNo ratings yet
- Langdon, Helen (20 06 22)Document2 pagesLangdon, Helen (20 06 22)helen langdonNo ratings yet
- Collagenase For Enzymatic Debridement A.2Document8 pagesCollagenase For Enzymatic Debridement A.2Agung GinanjarNo ratings yet
- Management TB MOH Singapore PDFDocument123 pagesManagement TB MOH Singapore PDFLindsley GruvyNo ratings yet
- Coding Clinic 2nd QTR 2021Document24 pagesCoding Clinic 2nd QTR 2021haru haroon100% (1)
- ASPEN Critical Care - Susan BrantleyDocument44 pagesASPEN Critical Care - Susan BrantleyVitoria SilvaNo ratings yet
- PPTDocument29 pagesPPTAkosh BB100% (1)
- Acoustic Neuroma in PregnancyDocument3 pagesAcoustic Neuroma in PregnancyHovlantaNo ratings yet
- Audiological Evaluation: Dr. Shakuntala Misra National Rehabilitation University, LucknowDocument3 pagesAudiological Evaluation: Dr. Shakuntala Misra National Rehabilitation University, LucknowHarshit AmbeshNo ratings yet
- Sarah Brock - FinalresumetppDocument3 pagesSarah Brock - Finalresumetppapi-297710364No ratings yet
- Ppt. Surgery Wild AnimalsDocument165 pagesPpt. Surgery Wild AnimalsAsha RaniNo ratings yet
- M&E FrameworksDocument9 pagesM&E FrameworksErshadNo ratings yet
- Home Care For EpilepsyDocument16 pagesHome Care For Epilepsysanish4uNo ratings yet

























































































Download as docx, pdf, or txt
You might also like
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- Cerebrovascular Accident Nursing Care PlanDocument4 pagesCerebrovascular Accident Nursing Care PlanCyrus De Asis67% (12)
- NCP GunshotDocument13 pagesNCP GunshotMichael John F. Natividad0% (1)
- Discharge PlanningDocument5 pagesDischarge PlanningNoora KhalidNo ratings yet
- Ischemic Stroke NCPDocument11 pagesIschemic Stroke NCPJohannah DaroNo ratings yet
- Nursing Care Plan (ImpairedphyssicalDocument5 pagesNursing Care Plan (ImpairedphyssicalkuroroexileNo ratings yet
- NCP #1 Ineffective Cerebral Tissue PerfusionDocument4 pagesNCP #1 Ineffective Cerebral Tissue PerfusionsteffiNo ratings yet
- NCP Ineffective Cerebral Tissue PerfusionDocument2 pagesNCP Ineffective Cerebral Tissue PerfusionAngelo ︻╦̵̵͇̿̿̿̿╤── Bulacan50% (6)
- Anatomy and Physiology of CVADocument4 pagesAnatomy and Physiology of CVAKimsha ConcepcionNo ratings yet
- Nursing Care Plan Hemorrhagic StrokeDocument8 pagesNursing Care Plan Hemorrhagic StrokeJeffrey Dela Cruz50% (4)
- Impaired Verbal CommunicationDocument3 pagesImpaired Verbal CommunicationDesiree Deleon Guerrero0% (2)
- Impaired Verbal CommunicationDocument1 pageImpaired Verbal Communicationdana100% (3)
- Nursing Care Plan: Subjective: Short Term Goal: Independent: Short Term GoalDocument1 pageNursing Care Plan: Subjective: Short Term Goal: Independent: Short Term GoalDante Sales75% (4)
- Pathophysiology CVADocument2 pagesPathophysiology CVASewyel Garburi100% (6)
- "Mayroong Namuong Dugo Sa Utak Niya Kaya Hindi Maayos Ang Daloy NG Dugo Rito" As Verbalized by The Patient'sDocument4 pages"Mayroong Namuong Dugo Sa Utak Niya Kaya Hindi Maayos Ang Daloy NG Dugo Rito" As Verbalized by The Patient'sAllisson BeckersNo ratings yet
- Case Study EsrdDocument4 pagesCase Study EsrdSTEPHANIE JOSUENo ratings yet
- NCP For Impaired Physical MobilityDocument2 pagesNCP For Impaired Physical MobilityPrincess Averin Navarro50% (2)
- NCP CvaDocument4 pagesNCP CvamannyV1990100% (1)
- NCPDocument2 pagesNCPLyka Mae Imbat - PacnisNo ratings yet
- NCP - Tissue Perfusion (Cerebral)Document2 pagesNCP - Tissue Perfusion (Cerebral)moodlayers50% (6)
- NCP 1: Ineffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Cerebrovascular AccidentDocument14 pagesNCP 1: Ineffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Cerebrovascular AccidentKyle Jingco100% (2)
- Ineffective Tissue PerfusionDocument1 pageIneffective Tissue PerfusionEm Castillo50% (2)
- CVA-NCPDocument7 pagesCVA-NCPAiza Oronce0% (1)
- Ineffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7Document2 pagesIneffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Hemorrhage As Evidenced by GCS of 7dana100% (4)
- Nursing Care Plan SeizureDocument2 pagesNursing Care Plan Seizuretimie_reyes100% (1)
- Nursing Care Plan (CVA)Document2 pagesNursing Care Plan (CVA)Mel Rodolfo50% (2)
- NCP For StrokeDocument4 pagesNCP For StrokeJASON OGALESCO100% (1)
- Self Care Deficit BahtingDocument1 pageSelf Care Deficit BahtingNaj SoliveresNo ratings yet
- Self Care DeficitDocument2 pagesSelf Care DeficitSj 斗力上75% (4)
- NCP CVA Impaired Physical Mobility 1Document2 pagesNCP CVA Impaired Physical Mobility 1Frency Anne Causo Pascual100% (1)
- NCP NeuroDocument20 pagesNCP NeuroNica Gaborne Navarro100% (3)
- CVA Activity IntoleranceDocument1 pageCVA Activity IntoleranceNursesLabs.com75% (4)
- NCP - Altered Tissue PerfusionDocument2 pagesNCP - Altered Tissue PerfusionLeigh Kristel Andrion0% (1)
- IMPAIRED PHYSICAL MOBILITY RT Neuromuscular Involvement (Right Sided Paresthesia Aeb Inability To Purposefully Move Body Parts.Document2 pagesIMPAIRED PHYSICAL MOBILITY RT Neuromuscular Involvement (Right Sided Paresthesia Aeb Inability To Purposefully Move Body Parts.Senyorita KHaye67% (3)
- Impaired Verbal CommunicationDocument3 pagesImpaired Verbal CommunicationCalimlim KimNo ratings yet
- NCP CvaDocument3 pagesNCP CvaJey PangilinanNo ratings yet
- Self Care DeficitDocument3 pagesSelf Care DeficitAddie Labitad100% (2)
- NCP Fracture Risk For InfectionDocument3 pagesNCP Fracture Risk For InfectionMiggsNo ratings yet
- Impaired Verbal CommunicationDocument2 pagesImpaired Verbal CommunicationEjay Barayuga100% (2)
- NCP - OsteosarcomaDocument5 pagesNCP - OsteosarcomaNelson Lacsamana100% (1)
- Post Open Reduction Internal Fixation PathophysiologyDocument3 pagesPost Open Reduction Internal Fixation PathophysiologyRizalyn QuindipanNo ratings yet
- Clonidine HydrochlorideDocument1 pageClonidine HydrochlorideLovelyn Joy Abubo CortezNo ratings yet
- Assessment Nursing Diagnosis Planning Implemantation Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Planning Implemantation Rationale EvaluationChloie Marie Rosalejos100% (1)
- NCP - Impaired Verbal Communication Related To Neuromascular Impairment As Manifested by AphaisaDocument2 pagesNCP - Impaired Verbal Communication Related To Neuromascular Impairment As Manifested by AphaisaKristina Angela CarbonNo ratings yet
- Nursing Care Plan CVADocument6 pagesNursing Care Plan CVAessevyNo ratings yet
- 14 Cerebrovascular Accident Nursing Care PlansDocument5 pages14 Cerebrovascular Accident Nursing Care PlansNickesha Mckenzie75% (4)
- NCP For CVADocument18 pagesNCP For CVAmolukas101100% (7)
- Stroke Nursing Care PlanDocument1 pageStroke Nursing Care PlanTracy Pearl100% (1)
- NCP - BedriddenDocument4 pagesNCP - Bedriddenadelaigner_racho589475% (4)
- NCP - Knowledge Deficit (Acromegaly)Document3 pagesNCP - Knowledge Deficit (Acromegaly)Kian HerreraNo ratings yet
- Spina Bifida NCPDocument3 pagesSpina Bifida NCPShahzad GulfamNo ratings yet
- JMJ Marist Brothers Notre Dame of Marbel University College of Arts and Sciences - Nursing Department Alunan Avenue, Koronadal City, South CotabatoDocument4 pagesJMJ Marist Brothers Notre Dame of Marbel University College of Arts and Sciences - Nursing Department Alunan Avenue, Koronadal City, South CotabatoJullie AgredaNo ratings yet
- Gout N C P BY BHERU LALDocument1 pageGout N C P BY BHERU LALBheru LalNo ratings yet
- Nursing Care Plan-1 Age: 50Y Medical Diagnoses: Fracture Assessment Nursing Diagnosis Planning Intervention Scientific Rationale EvaluationDocument2 pagesNursing Care Plan-1 Age: 50Y Medical Diagnoses: Fracture Assessment Nursing Diagnosis Planning Intervention Scientific Rationale EvaluationBheru LalNo ratings yet
- Case IcuDocument5 pagesCase IcuTrisha SuazoNo ratings yet
- Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective: "Maglisod Man Kog Short Term: Independent: - Establish RapportDocument3 pagesAssessment Diagnosis Planning Interventions Rationale Evaluation Subjective: "Maglisod Man Kog Short Term: Independent: - Establish RapportSergi Lee OrateNo ratings yet
- Activity IntoleranceDocument3 pagesActivity IntoleranceRaidis PangilinanNo ratings yet
- Cva NCP 1Document3 pagesCva NCP 1MarcieNo ratings yet
- NCP of Impaired MobilityDocument3 pagesNCP of Impaired MobilityHazel Cabrera0% (1)
- Assessment Diagnosis Scientific Explanation Planning Interventions Rationale Expected Outcome Subjective: O Short Term: Short TermDocument3 pagesAssessment Diagnosis Scientific Explanation Planning Interventions Rationale Expected Outcome Subjective: O Short Term: Short TermRaidis PangilinanNo ratings yet
- Subjective Data: Short Term Goal: Independent: 1. Monitor Patient's Vital Signs. 2. Determine Diagnosis That Short Term GoalDocument3 pagesSubjective Data: Short Term Goal: Independent: 1. Monitor Patient's Vital Signs. 2. Determine Diagnosis That Short Term GoalGeralyn KaeNo ratings yet
- Josue, Stephanie Canlas Batch 51 Reaction Paper Respiratory FailureDocument1 pageJosue, Stephanie Canlas Batch 51 Reaction Paper Respiratory FailureSTEPHANIE JOSUENo ratings yet
- Esrd Diagram PathophysiologyDocument3 pagesEsrd Diagram PathophysiologySTEPHANIE JOSUE100% (1)
- Esrd PathophysiologyDocument1 pageEsrd PathophysiologySTEPHANIE JOSUENo ratings yet
- Nuclear Medicine Technician or MedicalDocument2 pagesNuclear Medicine Technician or Medicalapi-79207760No ratings yet
- Trauma-Sensitive Yoga - Principles, Practice and ResearchDocument6 pagesTrauma-Sensitive Yoga - Principles, Practice and ResearchRichard Guerra100% (1)
- Just Another Sebaceous Cyst?: I. Clinical QuestionDocument3 pagesJust Another Sebaceous Cyst?: I. Clinical QuestionJaessa FelicianoNo ratings yet
- Cochlear-Implants Brochure 2Document2 pagesCochlear-Implants Brochure 2roroNo ratings yet
- Dr. Ashman's ENT Notes PDFDocument56 pagesDr. Ashman's ENT Notes PDFJulian GordonNo ratings yet
- Antibiotic Resistance: Key PointsDocument7 pagesAntibiotic Resistance: Key Pointsgeorgi.annaNo ratings yet
- Lilyasari2019 Article EconomicEvaluationOfSildenafilDocument9 pagesLilyasari2019 Article EconomicEvaluationOfSildenafilNajib Al FatinNo ratings yet
- History of Present IllnessDocument4 pagesHistory of Present Illnessegabe386No ratings yet
- Reading 5 Blood and Body DefensesDocument18 pagesReading 5 Blood and Body Defenseslephuongvy1406No ratings yet
- AntiemeticsDocument33 pagesAntiemeticsSaiNo ratings yet
- BLSPPT 180126100212 PDFDocument58 pagesBLSPPT 180126100212 PDFJerwynn Ilustre100% (1)
- Complex Regional Pain SyndromeDocument10 pagesComplex Regional Pain SyndromegeejeiNo ratings yet
- Physical TherapyDocument11 pagesPhysical TherapyEvelyn MedinaNo ratings yet
- Dissertation SalmonellaDocument7 pagesDissertation SalmonellaWriteMyPaperCoCanada100% (1)
- PANBIO IgM MAC ELISADocument5 pagesPANBIO IgM MAC ELISAmiss.JEJENo ratings yet
- Case Study 1Document9 pagesCase Study 1andry natanel tonyNo ratings yet
- TEP Jama 2022Document10 pagesTEP Jama 2022carla jazmin cortes rodriguezNo ratings yet
- Burns E 2013 PHD Thesis PDFDocument338 pagesBurns E 2013 PHD Thesis PDFDr-Rabia AlmamalookNo ratings yet
- Langdon, Helen (20 06 22)Document2 pagesLangdon, Helen (20 06 22)helen langdonNo ratings yet
- Collagenase For Enzymatic Debridement A.2Document8 pagesCollagenase For Enzymatic Debridement A.2Agung GinanjarNo ratings yet
- Management TB MOH Singapore PDFDocument123 pagesManagement TB MOH Singapore PDFLindsley GruvyNo ratings yet
- Coding Clinic 2nd QTR 2021Document24 pagesCoding Clinic 2nd QTR 2021haru haroon100% (1)
- ASPEN Critical Care - Susan BrantleyDocument44 pagesASPEN Critical Care - Susan BrantleyVitoria SilvaNo ratings yet
- PPTDocument29 pagesPPTAkosh BB100% (1)
- Acoustic Neuroma in PregnancyDocument3 pagesAcoustic Neuroma in PregnancyHovlantaNo ratings yet
- Audiological Evaluation: Dr. Shakuntala Misra National Rehabilitation University, LucknowDocument3 pagesAudiological Evaluation: Dr. Shakuntala Misra National Rehabilitation University, LucknowHarshit AmbeshNo ratings yet
- Sarah Brock - FinalresumetppDocument3 pagesSarah Brock - Finalresumetppapi-297710364No ratings yet
- Ppt. Surgery Wild AnimalsDocument165 pagesPpt. Surgery Wild AnimalsAsha RaniNo ratings yet
- M&E FrameworksDocument9 pagesM&E FrameworksErshadNo ratings yet
- Home Care For EpilepsyDocument16 pagesHome Care For Epilepsysanish4uNo ratings yet