Download as pdf or txt
You might also like
- Business and Society Stakeholders Ethics Public Policy 17Th Edition Anne Lawrence Full ChapterDocument67 pagesBusiness and Society Stakeholders Ethics Public Policy 17Th Edition Anne Lawrence Full Chaptermichael.lynch15578% (9)
- Hi-Survey Road User Manual-EN-20200330Document276 pagesHi-Survey Road User Manual-EN-20200330Mauricio RuizNo ratings yet
- Socket PreservationDocument24 pagesSocket PreservationFadly RasyidNo ratings yet
- (A. Basak) Analogue Electronic Circuits and SystemDocument376 pages(A. Basak) Analogue Electronic Circuits and SystemRusman Santai KaawuNo ratings yet
- Computer Project 1: Assignment 1.1Document10 pagesComputer Project 1: Assignment 1.1Nelu TurcanuNo ratings yet
- Sakurai Solutions 5-1 5-2Document8 pagesSakurai Solutions 5-1 5-2Raza Ali RazaNo ratings yet
- DARPA Accomplishments Vol 2Document410 pagesDARPA Accomplishments Vol 2sunburngr100% (1)
- 1 s2.0 S1067251621003495 MainDocument6 pages1 s2.0 S1067251621003495 MainMaria Gabriela CristanchoNo ratings yet
- Association Between Cardiovascular Diseases and Apical Periodontitis An Umbrella ReviewDocument13 pagesAssociation Between Cardiovascular Diseases and Apical Periodontitis An Umbrella ReviewSaadAzizNo ratings yet
- 32 01 09 GrazinaDocument16 pages32 01 09 GrazinaDisty ANo ratings yet
- Neutrophil To Lymphocyte Ratio and Periprosthetic Joint Infection A Systematic Review and Meta-AnalysisDocument8 pagesNeutrophil To Lymphocyte Ratio and Periprosthetic Joint Infection A Systematic Review and Meta-AnalysisJD2750No ratings yet
- 2010 - Epidemioloy of Ulcerative Keratitis in Northern CaliforniaDocument7 pages2010 - Epidemioloy of Ulcerative Keratitis in Northern CaliforniaPrasetya AnugrahNo ratings yet
- Epidemiology of Periodontitis: Chapter 6Document30 pagesEpidemiology of Periodontitis: Chapter 6Atziry LopezNo ratings yet
- Evidence-Based Diagnostics Adult Septic ArthritisDocument27 pagesEvidence-Based Diagnostics Adult Septic ArthritisLobozNo ratings yet
- OM Stafilococo (Clase Observacionales)Document7 pagesOM Stafilococo (Clase Observacionales)Jairo Camilo Guevara FaríasNo ratings yet
- 1 s2.0 S0140673619329897 MainDocument12 pages1 s2.0 S0140673619329897 MainMaharani Sari NastitiNo ratings yet
- Wandell 2018Document10 pagesWandell 2018Bảo Trân NguyễnNo ratings yet
- Yang 2014Document11 pagesYang 2014Prayitno SetiawanNo ratings yet
- Periodontal Disease, Edentulism, and Pancreatic Cancer: A Meta-AnalysisDocument11 pagesPeriodontal Disease, Edentulism, and Pancreatic Cancer: A Meta-AnalysisSmaranda GavrilNo ratings yet
- Epidemiology and Clinical Characteristics of Episcleritis and Scleritis in Olmsted County, MinnesotaDocument8 pagesEpidemiology and Clinical Characteristics of Episcleritis and Scleritis in Olmsted County, MinnesotaApriansyah Arfandy AzisNo ratings yet
- Lingen Et Al-2011-Oral DiseasesDocument16 pagesLingen Et Al-2011-Oral DiseasesSAMUEL ESCARESNo ratings yet
- Risk Factors For Medication-Related Osteonecrosis of The Jaws - A Systematic ReviewDocument10 pagesRisk Factors For Medication-Related Osteonecrosis of The Jaws - A Systematic ReviewP.No ratings yet
- 10 1016@j Prosdent 2020 04 001Document8 pages10 1016@j Prosdent 2020 04 001Luis Miguel ValenciaNo ratings yet
- Oral Cancer Grading SystemDocument42 pagesOral Cancer Grading SystemMadhura ShekatkarNo ratings yet
- Clinical Presentation, Management, and Prognosis of Pseudogout in Joint Arthroplasty: A Retrospective Cohort StudyDocument7 pagesClinical Presentation, Management, and Prognosis of Pseudogout in Joint Arthroplasty: A Retrospective Cohort StudyPutri Aswariyah RamliNo ratings yet
- Cassina 2019Document6 pagesCassina 2019dewaprasatyaNo ratings yet
- Pediatric JournalDocument11 pagesPediatric JournalHenny WijayaNo ratings yet
- Diagnosing OsteomyelitisDocument12 pagesDiagnosing Osteomyelitisna huNo ratings yet
- Infect oDocument8 pagesInfect ovanstrahlenamNo ratings yet
- Chung 2014Document6 pagesChung 2014Retno ManggalihNo ratings yet
- Cystic Lesions of The Jaws A Retrospective ClinicopathologicDocument11 pagesCystic Lesions of The Jaws A Retrospective ClinicopathologicThành Luân NguyễnNo ratings yet
- 10.1007@s00404 019 05301 XDocument11 pages10.1007@s00404 019 05301 XAbdElilah KoNo ratings yet
- Research: ArticleDocument4 pagesResearch: ArticleMuthu KumarNo ratings yet
- Epidemi IbdDocument9 pagesEpidemi IbdShanaz NovriandinaNo ratings yet
- Manejo de Neoplasia Intraepitelial AnalDocument10 pagesManejo de Neoplasia Intraepitelial AnalLibertad DíazNo ratings yet
- Prognostic Nomogram For Patients With Tongue Squamous Cell Carcinoma: A SEER-based StudyDocument15 pagesPrognostic Nomogram For Patients With Tongue Squamous Cell Carcinoma: A SEER-based Studymahmud.meftahNo ratings yet
- Factors For Second Non-Diagnostic Ultrasound-Guided Fine-Needle Aspiration Cytology in Thyroid NodulesDocument10 pagesFactors For Second Non-Diagnostic Ultrasound-Guided Fine-Needle Aspiration Cytology in Thyroid Nodulesmiguel saba sabaNo ratings yet
- HealthcareDocument13 pagesHealthcareMaria Liliana Calderon MaciasNo ratings yet
- Definisi Klasifikasi Etiologi Dan ManifeDocument11 pagesDefinisi Klasifikasi Etiologi Dan ManifenatassyamarizNo ratings yet
- Prolonged Breastfeeding Is Associated With Lower.30Document3 pagesProlonged Breastfeeding Is Associated With Lower.30ingridspulerNo ratings yet
- Primary Subacute Hematogenous Osteomyelitis in Children: A Clearer Bacteriological EtiologyDocument6 pagesPrimary Subacute Hematogenous Osteomyelitis in Children: A Clearer Bacteriological EtiologymiNo ratings yet
- Papola 2018Document56 pagesPapola 2018sajith4457No ratings yet
- Metanálisis y Revisión SisemáticaDocument9 pagesMetanálisis y Revisión SisemáticaPEDRO LUIS LOPEZ VILLALVAZONo ratings yet
- Prognostic JournalDocument6 pagesPrognostic JournalElpida WNo ratings yet
- 77d8 PDFDocument7 pages77d8 PDFRosyid PrasetyoNo ratings yet
- 1 s2.0 S1201971209003063 MainDocument4 pages1 s2.0 S1201971209003063 Mainlee zaraNo ratings yet
- Risk of Atrial Fibrillation According To Cancer Type: A Nationwide Population-Based StudyDocument12 pagesRisk of Atrial Fibrillation According To Cancer Type: A Nationwide Population-Based StudyBryan NguyenNo ratings yet
- Mortensen 2020Document9 pagesMortensen 2020sajith4457No ratings yet
- Ijo 58 4 5188 PDFDocument12 pagesIjo 58 4 5188 PDFriri sariNo ratings yet
- The Cascade of Care in Diagnosis and Treatment of Latent Tuberculosis Infection: A Systematic Review and Meta-AnalysisDocument10 pagesThe Cascade of Care in Diagnosis and Treatment of Latent Tuberculosis Infection: A Systematic Review and Meta-AnalysisArdi_xNo ratings yet
- The Diagnostic Criteria For Chronic EndometritisDocument7 pagesThe Diagnostic Criteria For Chronic EndometritisyuriescaidaNo ratings yet
- 1 s2.0 S0923753419374125 MainDocument7 pages1 s2.0 S0923753419374125 MainGabriela MonteiroNo ratings yet
- Surgical Neurology International: Socioeconomic Status Does Not Affect Prognosis in Patients With Glioblastoma MultiformeDocument9 pagesSurgical Neurology International: Socioeconomic Status Does Not Affect Prognosis in Patients With Glioblastoma MultiformeALINo ratings yet
- Epidemiology of Periodontal Older: Disease Among AdultsDocument18 pagesEpidemiology of Periodontal Older: Disease Among AdultsDiana Choiro WNo ratings yet
- Journal of Dentistry: Review ArticleDocument13 pagesJournal of Dentistry: Review ArticleNidia TorreaNo ratings yet
- Risk of Leukemia After DengueDocument7 pagesRisk of Leukemia After DengueJoão Marcos Germano SouzaNo ratings yet
- Surgical Site Infections Latest Literature Update March 2019Document42 pagesSurgical Site Infections Latest Literature Update March 2019shah hassaanNo ratings yet
- Prevalence and Associated Factors of HIV Infection Among Pregnant Women Attending Antenatal Care at The Yaoundé Central HospitalDocument6 pagesPrevalence and Associated Factors of HIV Infection Among Pregnant Women Attending Antenatal Care at The Yaoundé Central HospitalnabilahbilqisNo ratings yet
- Cam4 9 8333Document12 pagesCam4 9 8333Mithua ghoshNo ratings yet
- Prevention of Surgical Site Infections in Orthopaedic Surgery: A Synthesis of Current RecommendationsDocument16 pagesPrevention of Surgical Site Infections in Orthopaedic Surgery: A Synthesis of Current RecommendationsPankaj VatsaNo ratings yet
- The Oncologist 2003 Weinstein 278 92Document15 pagesThe Oncologist 2003 Weinstein 278 92Josne J. PaezNo ratings yet
- Research Article: The Analysis of Etiology and Risk Factors For 192 Cases of Neonatal SepsisDocument7 pagesResearch Article: The Analysis of Etiology and Risk Factors For 192 Cases of Neonatal Sepsisflorentina lulutNo ratings yet
- HIV Infectivity Per Coital ActDocument8 pagesHIV Infectivity Per Coital Actkedirali921No ratings yet
- Pinto 2020Document14 pagesPinto 2020s7ybkjhb44No ratings yet
- Escholarship UC Item 8cz3v9zdDocument9 pagesEscholarship UC Item 8cz3v9zdGabriela LemNo ratings yet
- Medoral 29 E135Document10 pagesMedoral 29 E135Maria CorenaNo ratings yet
- Frozen Section Pathology: Diagnostic ChallengesFrom EverandFrozen Section Pathology: Diagnostic ChallengesAlain C. BorczukNo ratings yet
- Calcifying Odontogenic Cyst A Report of Two Clinical Cases 2019Document4 pagesCalcifying Odontogenic Cyst A Report of Two Clinical Cases 2019Fadly RasyidNo ratings yet
- Odontogenic Cysts and Neoplasms 2017 PDFDocument46 pagesOdontogenic Cysts and Neoplasms 2017 PDFFadly RasyidNo ratings yet
- Odontogenic Cysts An Update 2017 PDFDocument6 pagesOdontogenic Cysts An Update 2017 PDFFadly RasyidNo ratings yet
- Odontogenic Cysts 2015Document11 pagesOdontogenic Cysts 2015Fadly RasyidNo ratings yet
- Odontogenic Cysts and Tumors What Radiologists Need To Know 2019Document22 pagesOdontogenic Cysts and Tumors What Radiologists Need To Know 2019Fadly RasyidNo ratings yet
- Fan Heater - B-011 - Data SheetsDocument9 pagesFan Heater - B-011 - Data SheetsNadim Ahmad SiddiqueNo ratings yet
- Fourth Quarter Exam in TLE Grade SevenDocument5 pagesFourth Quarter Exam in TLE Grade SevenShabby Gay Trogani83% (12)
- EW74Ëó+ Á+ ÚDocument9 pagesEW74Ëó+ Á+ Úundibal rivasNo ratings yet
- Dr. Jufri Latief (Neuromuskuler Problems)Document28 pagesDr. Jufri Latief (Neuromuskuler Problems)EmirNo ratings yet
- FS-C5100-C5200-C5300 PartsDocument47 pagesFS-C5100-C5200-C5300 PartsDennis LeeNo ratings yet
- Q1. As A Production Manager For RMC, What Do You Recommend? Why??Document2 pagesQ1. As A Production Manager For RMC, What Do You Recommend? Why??MUNSIF JAWEEDNo ratings yet
- Updating The Canadian Standards Association Offshore Structures CodeDocument6 pagesUpdating The Canadian Standards Association Offshore Structures CodenabiloucheNo ratings yet
- Serial Adder Mealy Modelling ProgramDocument22 pagesSerial Adder Mealy Modelling ProgrambcemailidNo ratings yet
- Methods?: Condoms Internal Condoms Sexually Transmissible Infections (Stis)Document25 pagesMethods?: Condoms Internal Condoms Sexually Transmissible Infections (Stis)Alecia R. CastilloNo ratings yet
- Unit 4 NotesDocument60 pagesUnit 4 NotesVikas RathodNo ratings yet
- 2006 Philippines Road ClassificationDocument44 pages2006 Philippines Road ClassificationpetiepanNo ratings yet
- Nclex Boot CampDocument24 pagesNclex Boot CampMariekris Sangalang100% (12)
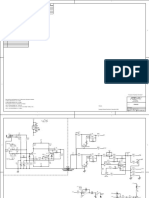
- Peavey Xr8000 SCHDocument12 pagesPeavey Xr8000 SCHLisandro Orrego SalvadorNo ratings yet
- Artikel Review BiodegradasiDocument6 pagesArtikel Review BiodegradasiEka Ayu NingtyasNo ratings yet
- Experiment 4 Turbine CharacteristicsDocument12 pagesExperiment 4 Turbine CharacteristicsChong Ru YinNo ratings yet
- Nabcep AppendixesDocument32 pagesNabcep AppendixeshockpinNo ratings yet
- PPP-Eclipse-E05 Module 05 IDUsDocument11 pagesPPP-Eclipse-E05 Module 05 IDUsJervy SegarraNo ratings yet
- Biology Form 5: 5.1: MENDEL'S ExperimentDocument29 pagesBiology Form 5: 5.1: MENDEL'S Experimentveronica francisNo ratings yet
- Plag - ReportDocument6 pagesPlag - ReportMehedi HasanNo ratings yet
- Motion Information and MediaDocument39 pagesMotion Information and Mediajadeshades12No ratings yet
- Project 1 - School - Architecture Design - HandoutDocument6 pagesProject 1 - School - Architecture Design - Handoutawais anjumNo ratings yet
- Ram Janm Bhumi Babri Masjid - Ayodhya BenchDocument251 pagesRam Janm Bhumi Babri Masjid - Ayodhya BenchNaresh KadyanNo ratings yet
- Lesson Plan Format (Acad)Document4 pagesLesson Plan Format (Acad)Aienna Lacaya MatabalanNo ratings yet
- Three Dimensional GeometryDocument3 pagesThree Dimensional GeometryTaqi IsmailNo ratings yet