Download as pdf or txt
You might also like
- Drugs Behaviour and Modern Society Canadian 1st Edition Hamilton Test BankDocument62 pagesDrugs Behaviour and Modern Society Canadian 1st Edition Hamilton Test Banksarahmontgomerynteqbfmczs100% (16)
- Drug Education and Vice ControlDocument59 pagesDrug Education and Vice ControlJvnRodz P Gmlm90% (10)
- William H. Soine - Clandestine Drug SynthesisDocument34 pagesWilliam H. Soine - Clandestine Drug SynthesisAnonymous Gb9EyW83% (6)
- Sscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssDocument4 pagesSscchhiizzoopphhrreenniiaa: Ccuurrrreenntt Ttrreeaattm Meenntt CcoonnssiiddeerraattiioonnssLeslie CitromeNo ratings yet
- PerioperativeDocument15 pagesPerioperativeJEFFERSON MUÑOZNo ratings yet
- DosingSGAPosterWCBPHandout CITROME 2005Document4 pagesDosingSGAPosterWCBPHandout CITROME 2005Leslie CitromeNo ratings yet
- Commentary: Novel Application For G Protein - Biased Mu Opioid Receptor Agonists in Opioid Relapse PreventionDocument2 pagesCommentary: Novel Application For G Protein - Biased Mu Opioid Receptor Agonists in Opioid Relapse PreventionIntan AyuNo ratings yet
- References: Monotherapy Versus Polypharmacy For Hospitalized Psychiatric PatientsDocument1 pageReferences: Monotherapy Versus Polypharmacy For Hospitalized Psychiatric PatientsLeslie CitromeNo ratings yet
- Roux 2013Document7 pagesRoux 2013andrew herringNo ratings yet
- HHS Public AccessDocument19 pagesHHS Public Accessyeremias setyawanNo ratings yet
- The Behavioral Effects of The Antidepressant Tianeptine Require The Mu-Opioid ReceptorDocument12 pagesThe Behavioral Effects of The Antidepressant Tianeptine Require The Mu-Opioid ReceptorAgnieszka HajdukNo ratings yet
- Jurnal Jiwa 2Document18 pagesJurnal Jiwa 2Yolanda Karoline PasaribuNo ratings yet
- Short-Term and Long-Term Evaluation of Selective Serotonin Reuptake Inhibitors in The Treatment of Panic Disorder: Fluoxetine Vs CitalopramDocument6 pagesShort-Term and Long-Term Evaluation of Selective Serotonin Reuptake Inhibitors in The Treatment of Panic Disorder: Fluoxetine Vs CitalopramBakhita MaryamNo ratings yet
- Effects of Ascending Buprenorphine Doses On Measur - 2019 - Journal of SubstanceDocument7 pagesEffects of Ascending Buprenorphine Doses On Measur - 2019 - Journal of SubstanceARACELY RAFAELA CORNEJO MARTINEZNo ratings yet
- Actigraphic Measurements in Opioid Detoxification With Methadone or BuprenorphineDocument8 pagesActigraphic Measurements in Opioid Detoxification With Methadone or BuprenorphineSaiber PanNo ratings yet
- Vivtrol InductionDocument18 pagesVivtrol InductionElly NuñezNo ratings yet
- Relapse in Outpatient Treatment For Marijuana Dependence: Brent A. Moore PH.D., Alan J. Budney, PH.DDocument5 pagesRelapse in Outpatient Treatment For Marijuana Dependence: Brent A. Moore PH.D., Alan J. Budney, PH.DAntonio Tejero PocielloNo ratings yet
- Cannabis Withdrawal: A Review of Neurobiological Mechanisms and Sex DifferencesDocument7 pagesCannabis Withdrawal: A Review of Neurobiological Mechanisms and Sex DifferencesRaúl AñariNo ratings yet
- NIH Public Access: Buprenorphine-Nalxone Therapy in Pain ManagementDocument25 pagesNIH Public Access: Buprenorphine-Nalxone Therapy in Pain ManagementyoiiiNo ratings yet
- Jurnalnantipsychotic PDFDocument9 pagesJurnalnantipsychotic PDFamiaslimNo ratings yet
- Psychotherapy Plus Antidepressant For Panic Disorder With or Without Agoraphobia Systematic ReviewDocument8 pagesPsychotherapy Plus Antidepressant For Panic Disorder With or Without Agoraphobia Systematic ReviewRizky AmNo ratings yet
- Substance Use Disorder in Physicians After Completion of Training in Anesthesiology in The United States From 1977 To 2013Document8 pagesSubstance Use Disorder in Physicians After Completion of Training in Anesthesiology in The United States From 1977 To 2013David LedezmaNo ratings yet
- Prevalence of Substance Misuse in First-Episode Psychosis - Cantwell Et AlDocument5 pagesPrevalence of Substance Misuse in First-Episode Psychosis - Cantwell Et Almess.benhamoudaNo ratings yet
- Subjective Effectiveness of Ibogaine Treatment For Problematic Opioid Consumption: Short-And Long-Term Outcomes and Current Psychological FunctioningDocument9 pagesSubjective Effectiveness of Ibogaine Treatment For Problematic Opioid Consumption: Short-And Long-Term Outcomes and Current Psychological FunctioningB. ZapoteNo ratings yet
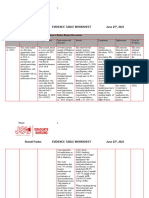
- BP DNP Evidence Table WorksheetDocument43 pagesBP DNP Evidence Table Worksheetapi-706947027No ratings yet
- Dixon 1990Document11 pagesDixon 1990MaulNo ratings yet
- A Preliminary Trial: Double-Blind Comparison of Nefazodone, Bupropion-SR, and Placebo in The Treatment of Cannabis DependenceDocument12 pagesA Preliminary Trial: Double-Blind Comparison of Nefazodone, Bupropion-SR, and Placebo in The Treatment of Cannabis DependenceJai KunvarNo ratings yet
- Therapeutics: A Benjamin Srivastava, John J Mariani, Frances R LevinDocument11 pagesTherapeutics: A Benjamin Srivastava, John J Mariani, Frances R LevinPsiquiatria 2021-2No ratings yet
- Benzodiazepines in Schizophrenia Is There A Trend Towards Long Term PrescribingDocument3 pagesBenzodiazepines in Schizophrenia Is There A Trend Towards Long Term PrescribingMaulida 04No ratings yet
- A Prospective Observational Study On Assessment of Prescription Pattern Among Patients Suffering From Cervical and Lumbar PainDocument10 pagesA Prospective Observational Study On Assessment of Prescription Pattern Among Patients Suffering From Cervical and Lumbar PaindrziaapollohospitalsNo ratings yet
- Bupropion 1Document22 pagesBupropion 1Robert MovileanuNo ratings yet
- Precision Medicine in Alcohol Dependence A Controlled Trial Testing Pharmacotherapy Response Among Reward and Relief Drinking PhenotypesDocument9 pagesPrecision Medicine in Alcohol Dependence A Controlled Trial Testing Pharmacotherapy Response Among Reward and Relief Drinking Phenotypes陳弘儒No ratings yet
- Crow Et Al-2009-International Journal of Eating DisordersDocument8 pagesCrow Et Al-2009-International Journal of Eating DisordersRosarioNo ratings yet
- National Use of Prescription Medications For Insomnia: NHANES 1999-2010Document10 pagesNational Use of Prescription Medications For Insomnia: NHANES 1999-2010Agustina ZairidaNo ratings yet
- Treatment of Acute Opoid Withdrawal With IbogaineDocument9 pagesTreatment of Acute Opoid Withdrawal With IbogaineMaggotskinNo ratings yet
- Five Year Follow Up of Bilateral Stimulation of The Subthalamic Nucleus in Advanced Parkinson's DiseaseDocument10 pagesFive Year Follow Up of Bilateral Stimulation of The Subthalamic Nucleus in Advanced Parkinson's DiseaseRicardo GarciaNo ratings yet
- Medicina 56 00453Document3 pagesMedicina 56 00453Michael UNo ratings yet
- FIBROMYALGIADocument11 pagesFIBROMYALGIAAmalia Dwi AriskaNo ratings yet
- Evaluation of Treatment-Resistant SchizophreniaDocument12 pagesEvaluation of Treatment-Resistant SchizophreniaFlo RenceNo ratings yet
- Pharma - HistoryDocument3 pagesPharma - HistoryJm AshiiNo ratings yet
- Nihms 1753461Document30 pagesNihms 1753461Michael UNo ratings yet
- Perception and Practice Among Emergency Medicine Health Care Providers Regarding Discharging Patients After Opioid AdministrationDocument15 pagesPerception and Practice Among Emergency Medicine Health Care Providers Regarding Discharging Patients After Opioid AdministrationSUPHAWICH KHOIKAEWNo ratings yet
- (25599283 - Journal of Psychedelic Studies) Long-Lasting Analgesic Effect of The Psychedelic Drug Changa - A Case ReportDocument7 pages(25599283 - Journal of Psychedelic Studies) Long-Lasting Analgesic Effect of The Psychedelic Drug Changa - A Case ReportMariaNo ratings yet
- New Frontiers in Obesity Treatment - GLP-1 and Nascent Nutrient-Stimulated Hormone-Based TherapeuticsDocument18 pagesNew Frontiers in Obesity Treatment - GLP-1 and Nascent Nutrient-Stimulated Hormone-Based TherapeuticssacarrilNo ratings yet
- Bup L Termaintainance PDFDocument5 pagesBup L Termaintainance PDFnarasimhahanNo ratings yet
- HHS Public Access: Fish Oil and Depression: The Skinny On FatsDocument13 pagesHHS Public Access: Fish Oil and Depression: The Skinny On FatsIqbal AbdillahNo ratings yet
- Acute Effects of Drug Abuse in Schizophrenic Patients: Clinical Observations and Patients' Self-ReportsDocument11 pagesAcute Effects of Drug Abuse in Schizophrenic Patients: Clinical Observations and Patients' Self-ReportsAnonymous uyScQy4No ratings yet
- Methadone Treatment in The U.S.ADocument43 pagesMethadone Treatment in The U.S.Aleeperlhan2000No ratings yet
- Marijuana Dependence Not Just Smoke andDocument14 pagesMarijuana Dependence Not Just Smoke andŁukasz OwsiankoNo ratings yet
- SNRI - Simptome de DiscontinuareDocument9 pagesSNRI - Simptome de DiscontinuareRobert MovileanuNo ratings yet
- Mackay 1997Document12 pagesMackay 1997Julio JuarezNo ratings yet
- Basic Principles in PharmacologyDocument30 pagesBasic Principles in Pharmacologyemmahpkemoi5No ratings yet
- Poor Medication Adherence and Risk of Relapse Associated With Continued Cannabis Use in Patients With First-Episode Psychosis: A Prospective AnalysisDocument7 pagesPoor Medication Adherence and Risk of Relapse Associated With Continued Cannabis Use in Patients With First-Episode Psychosis: A Prospective AnalysisArif IrpanNo ratings yet
- Methods of Detoxification and Their Role in Treating Patients With Opioid DependenceDocument3 pagesMethods of Detoxification and Their Role in Treating Patients With Opioid DependenceAndy PurnomoNo ratings yet
- This Document Contains Text Automatically Extracted From A PDF or Image File. Formatting May Have Been Lost and Not All Text May Have Been RecognizedDocument27 pagesThis Document Contains Text Automatically Extracted From A PDF or Image File. Formatting May Have Been Lost and Not All Text May Have Been RecognizedМатиас Себальос ГусманNo ratings yet
- Opioid Dystonia 1Document1 pageOpioid Dystonia 1PuneetNo ratings yet
- Incidence Duration Side Effects Those Rated BothersomeDocument7 pagesIncidence Duration Side Effects Those Rated BothersomeRogério Ramos MarquesNo ratings yet
- Involvement of Mu-, Delta-And Kappa-Opioid Receptor Subtypes in The Discriminative-Stimulus Effects of Delta-9-Tetrahydrocannabinol (THC) in RatsDocument9 pagesInvolvement of Mu-, Delta-And Kappa-Opioid Receptor Subtypes in The Discriminative-Stimulus Effects of Delta-9-Tetrahydrocannabinol (THC) in RatsGabriel MontoyaNo ratings yet
- Asian J. Med. Pharm. Res. 2 (3) 47-52, 2012Document6 pagesAsian J. Med. Pharm. Res. 2 (3) 47-52, 2012juandellibroNo ratings yet
- Nabiximols For Opioid-Treated Cancer Patients With Poorly-Controlled Chronic PainDocument12 pagesNabiximols For Opioid-Treated Cancer Patients With Poorly-Controlled Chronic PainffdandreaNo ratings yet
- Traditional Chinese Medicine For Treatment of FibromyalgiaDocument14 pagesTraditional Chinese Medicine For Treatment of FibromyalgiaMiki ShimizuNo ratings yet
- 10 1 1 152 5618 PDFDocument30 pages10 1 1 152 5618 PDFWichitra SisuwanNo ratings yet
- Handbook of Methadone Prescribing and Buprenorphine TherapyFrom EverandHandbook of Methadone Prescribing and Buprenorphine TherapyNo ratings yet
- GPHC Pre-Registration Complete Exam Question List JUNE 2017 - NOV 2021Document50 pagesGPHC Pre-Registration Complete Exam Question List JUNE 2017 - NOV 2021Summer Sunshine TVNo ratings yet
- Drug Education and Vice ControlDocument12 pagesDrug Education and Vice ControlJhuan Paulo Aquino ClavecillasNo ratings yet
- Opium Poppy Cultivation and Heroin Processing in Southeast AsiaDocument37 pagesOpium Poppy Cultivation and Heroin Processing in Southeast Asiaj0sipa007No ratings yet
- Fernanda Sobrino JMPDocument63 pagesFernanda Sobrino JMPJ. Fernando G. R.No ratings yet
- CDI 101 Second SemDocument252 pagesCDI 101 Second SemJopat Dejesus50% (2)
- Addiction A Very Short Introduction Keith Humphreys Full ChapterDocument67 pagesAddiction A Very Short Introduction Keith Humphreys Full Chapterjustin.martin277100% (5)
- QuickCheck Eval FinalDocument7 pagesQuickCheck Eval Final19999999999No ratings yet
- Naresh ChemistryDocument15 pagesNaresh Chemistryrohit balotNo ratings yet
- 10 Kinds of Drug AbuseDocument10 pages10 Kinds of Drug AbuseJennifer Piloton CañeteNo ratings yet
- Chapter 95 - The Drug Control and Enforcement Act PDFDocument113 pagesChapter 95 - The Drug Control and Enforcement Act PDFEsther MaugoNo ratings yet
- Drugs and Ra 9165Document98 pagesDrugs and Ra 9165Athynna LiquitNo ratings yet
- Drug Abuse & Prevention Word DockDocument9 pagesDrug Abuse & Prevention Word DockBasmah AnsariNo ratings yet
- Drugs Class 12 ProjectDocument20 pagesDrugs Class 12 ProjectJitender MorNo ratings yet
- Drug Education and Vice ControlDocument86 pagesDrug Education and Vice ControlArt-J Cuaresma FidelNo ratings yet
- ADD VOCAB txtNEWDocument6 pagesADD VOCAB txtNEWLaura PlatónNo ratings yet
- American Heart of Darkness: Volume I The Transformation of The American Republic Into A PathocracyDocument453 pagesAmerican Heart of Darkness: Volume I The Transformation of The American Republic Into A PathocracyRobert Kirkconnell100% (1)
- Missouri Counties Sue Drug Companies Over Opioid CrisisDocument274 pagesMissouri Counties Sue Drug Companies Over Opioid CrisisSam ClancyNo ratings yet
- Glamour and Despair. For Many It Generated An Excitement, A DicingDocument5 pagesGlamour and Despair. For Many It Generated An Excitement, A DicingParag SharmaNo ratings yet
- Therapeutic Drug Monitoring: ToxicologyDocument4 pagesTherapeutic Drug Monitoring: ToxicologyDorothy ReyesNo ratings yet
- Break Addictions HabitsDocument294 pagesBreak Addictions HabitsDawud Muhammad100% (2)
- Drugs and Drug Policy BibliographyDocument20 pagesDrugs and Drug Policy BibliographyJohn M. SmithNo ratings yet
- Drug Interdiction PDFDocument356 pagesDrug Interdiction PDFBryan JacobsonNo ratings yet
- Simon Parsons - Kennedy PaperDocument8 pagesSimon Parsons - Kennedy Papermuhamad bakliziNo ratings yet
- Jurnal Data P4GN 2014 - Edisi 2015 - ENDocument242 pagesJurnal Data P4GN 2014 - Edisi 2015 - ENAnti NarkobaNo ratings yet
- Managing Amphetamine Dependence: Malcolm BruceDocument8 pagesManaging Amphetamine Dependence: Malcolm BrucejuraiddinNo ratings yet
- NSTP Midterms ReviewerDocument2 pagesNSTP Midterms ReviewerMark Jayson0% (1)
- Erich Goode On DrugsDocument36 pagesErich Goode On DrugsAna SzerencsesNo ratings yet