Download as pdf or txt
You might also like
- 9 - Internal Medicine Buzzwords Handout Oct 2023 John Michael RuizDocument8 pages9 - Internal Medicine Buzzwords Handout Oct 2023 John Michael RuizJohn Michael RuizNo ratings yet
- 100 Test Aarogya 2.0:: Mrs - Gunjan MisraDocument19 pages100 Test Aarogya 2.0:: Mrs - Gunjan Misramomo misraNo ratings yet
- EnalaprilDocument6 pagesEnalaprilEduardo EvangelistaNo ratings yet
- Randomized Controlled Clinical Trial of Corticosteroids Plus Ace-Inhibitors With Long-Term Follow-Up in Proteinuric Iga NephropathyDocument7 pagesRandomized Controlled Clinical Trial of Corticosteroids Plus Ace-Inhibitors With Long-Term Follow-Up in Proteinuric Iga Nephropathyguugle gogleNo ratings yet
- Akizawa 2009Document9 pagesAkizawa 2009PROF. ERWIN M. GLOBIO, MSITNo ratings yet
- Efficacy and Safety of Monascus Purpureus Went Rice in Subjects With HyperlipidemiaDocument8 pagesEfficacy and Safety of Monascus Purpureus Went Rice in Subjects With HyperlipidemiaAyshe SlocumNo ratings yet
- Turkjmedsci-50-354 PubmedDocument6 pagesTurkjmedsci-50-354 PubmedRizka Uda'aNo ratings yet
- Effecrof Exerciseon NAFLDDocument1 pageEffecrof Exerciseon NAFLDjihanvrpNo ratings yet
- Effects of Correction of Metabolic Acidosis On Blood Urea and Bone Metabolism in Patients With Mild To Moderate Chronic Kidney Disease A ProspectiveDocument7 pagesEffects of Correction of Metabolic Acidosis On Blood Urea and Bone Metabolism in Patients With Mild To Moderate Chronic Kidney Disease A ProspectiveHigh LowNo ratings yet
- Nastasio2018 1Document7 pagesNastasio2018 1Milagros Pichardo RodriguezNo ratings yet
- Adverse Event Chloroquine 1Document8 pagesAdverse Event Chloroquine 1Ingrid KoutioNo ratings yet
- Konishi 2008Document6 pagesKonishi 2008PROF. ERWIN M. GLOBIO, MSITNo ratings yet
- 60 TeneligliptinDocument9 pages60 Teneligliptinankit AcharyaNo ratings yet
- Effect of Restricted Protein Diet Supplemented WitDocument11 pagesEffect of Restricted Protein Diet Supplemented WitBogdan LeonardNo ratings yet
- Disclosure of Interest: None DeclaredDocument1 pageDisclosure of Interest: None DeclaredLilíNo ratings yet
- (2018) - Cyclosporine For Chronic Spontaneous Urticaria A Meta-Analysis and Systematic Review. The Journal of Allergy and Clinical ImmunologyDocument14 pages(2018) - Cyclosporine For Chronic Spontaneous Urticaria A Meta-Analysis and Systematic Review. The Journal of Allergy and Clinical ImmunologyelçinNo ratings yet
- X. Young 2011 HepDocument11 pagesX. Young 2011 HepJuan Carlos FloresNo ratings yet
- Reliability of Mini Nutritional Assessment in Hemodialysis Compared With Subjective Global AssessmentDocument6 pagesReliability of Mini Nutritional Assessment in Hemodialysis Compared With Subjective Global AssessmentyafanitaizzatiNo ratings yet
- Jurnal Kedokteran Dan Kesehatan Indonesia: Indonesian Journal of Medicine and HealthDocument8 pagesJurnal Kedokteran Dan Kesehatan Indonesia: Indonesian Journal of Medicine and HealthWendy ErikNo ratings yet
- Jurnal Kedokteran Dan Kesehatan Indonesia: Indonesian Journal of Medicine and HealthDocument8 pagesJurnal Kedokteran Dan Kesehatan Indonesia: Indonesian Journal of Medicine and HealthWendy ErikNo ratings yet
- DMJ 37 465Document10 pagesDMJ 37 465sn4s7nyxcbNo ratings yet
- A Prospective, Randomized Clinical Trial of Etelcalcetide in Patients Receiving Hemodialysis With Secondary Hyperparathyroidism (The DUET Trial)Document10 pagesA Prospective, Randomized Clinical Trial of Etelcalcetide in Patients Receiving Hemodialysis With Secondary Hyperparathyroidism (The DUET Trial)guugle gogleNo ratings yet
- Atrial Natriuretic Peptide For Management of Acute Kidney InjuryDocument12 pagesAtrial Natriuretic Peptide For Management of Acute Kidney InjuryHadsfrv KajdgygNo ratings yet
- Ref 9 - García AlmeidaDocument2 pagesRef 9 - García AlmeidajavierNo ratings yet
- Monotherapy With PCSK9iDocument7 pagesMonotherapy With PCSK9inuttchorrNo ratings yet
- Intradialytic Parenteral Nutrition Improves Protein and Energy Homeostasis in Chronic Hemodialysis PatientsDocument10 pagesIntradialytic Parenteral Nutrition Improves Protein and Energy Homeostasis in Chronic Hemodialysis PatientsBianca CheungNo ratings yet
- Jurnal Terapi ACE Inhibitors in Anthracycline Induced CardiotoxicityDocument6 pagesJurnal Terapi ACE Inhibitors in Anthracycline Induced CardiotoxicityalerohmadNo ratings yet
- Randomized Controlled Trial of Tinospora Crispa For Additional Therapy in Patients With Type 2 Diabetes MellitusDocument4 pagesRandomized Controlled Trial of Tinospora Crispa For Additional Therapy in Patients With Type 2 Diabetes MellitusEva SuryantiNo ratings yet
- Study of Plasma Level of Atorvastatin and Its Effect On Lipid ProfileDocument10 pagesStudy of Plasma Level of Atorvastatin and Its Effect On Lipid Profileheema valeraNo ratings yet
- Journal Amitriptilin Dan GabapentinDocument17 pagesJournal Amitriptilin Dan GabapentinRidho Mochine FisciensaNo ratings yet
- JCDR 11 FC01Document5 pagesJCDR 11 FC01Manmohan SinghNo ratings yet
- Journal of Research in Pharmacy PracticeDocument6 pagesJournal of Research in Pharmacy PracticeLasiaf AlaskaNo ratings yet
- NGAL Como Biomarcador en La Enfermedad Renal CrónicaDocument13 pagesNGAL Como Biomarcador en La Enfermedad Renal CrónicaventasNo ratings yet
- Pi Is 0973688315002650Document1 pagePi Is 0973688315002650ella faotNo ratings yet
- Jurnal Bingg 1Document5 pagesJurnal Bingg 1Tasya AuliaNo ratings yet
- 2010 Stuard Pycnogenol Improves Kidney Function in Metabolic SyndromeDocument6 pages2010 Stuard Pycnogenol Improves Kidney Function in Metabolic Syndromeindoglo1No ratings yet
- RJVP - 7 - 2 - 39-52 Feline StudyDocument14 pagesRJVP - 7 - 2 - 39-52 Feline StudyIvannia ArayaNo ratings yet
- Kuthiroly2021 Article LipoproteinLipaseDeficiencyDocument7 pagesKuthiroly2021 Article LipoproteinLipaseDeficiencybrajendra singhNo ratings yet
- Prop. 2Document10 pagesProp. 2Kenya Isabel Contreras IslasNo ratings yet
- Febuxostat Therapy For Patients With Stage 3 CKD and Asymptomatic Hyperuricemia: A Randomized TrialDocument13 pagesFebuxostat Therapy For Patients With Stage 3 CKD and Asymptomatic Hyperuricemia: A Randomized TrialAndreas AdiwinataNo ratings yet
- A Supplemental Intravenous Amino Acid Infusion SusDocument8 pagesA Supplemental Intravenous Amino Acid Infusion Susmargareth silaenNo ratings yet
- RCT ArticleDocument8 pagesRCT ArticleelpisNo ratings yet
- A Metabolomic Analysis of Thiol Response For Standard and Modified N-Acetyl Cysteine Treatment Regimens in Patients With Acetaminophen OverdoseDocument14 pagesA Metabolomic Analysis of Thiol Response For Standard and Modified N-Acetyl Cysteine Treatment Regimens in Patients With Acetaminophen OverdosePaweł KowalczukNo ratings yet
- Estimation of Protein Intake Using Urinary Urea Nitrogen in CirrhosisDocument5 pagesEstimation of Protein Intake Using Urinary Urea Nitrogen in CirrhosisSvt Mscofficial2No ratings yet
- An Observational Study On-Management of Anemia in CKD Using Erythropoietin AlphaDocument10 pagesAn Observational Study On-Management of Anemia in CKD Using Erythropoietin AlphaTJPRC PublicationsNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Saban 2016Document7 pagesSaban 2016Hervita YeniNo ratings yet
- 25200931Document7 pages25200931Mustika Dwi SusilowatiNo ratings yet
- Mycophenolate Mofetil Versus Azathioprine in The Maintenance Therapy of Lupus NephritisDocument6 pagesMycophenolate Mofetil Versus Azathioprine in The Maintenance Therapy of Lupus NephritisdkjoshiameNo ratings yet
- Liu 2018Document7 pagesLiu 2018Süññy MäñèNo ratings yet
- Sulodexide For Kidney Protection in Type 2 Diabetes PatientsDocument8 pagesSulodexide For Kidney Protection in Type 2 Diabetes PatientsFerdinand YuzonNo ratings yet
- CKD - A Novel Approach To Adenine-Induced Chronic Kidney Disease Associated Anemia in RodentDocument17 pagesCKD - A Novel Approach To Adenine-Induced Chronic Kidney Disease Associated Anemia in RodentCher IshNo ratings yet
- CEH Art 46773-10Document7 pagesCEH Art 46773-10Sabina DiktaNo ratings yet
- Effects of Probiotic Supplementation On Lipid Profile of Women With Rheumatoid Arthritis: A Randomized Placebo-Controlled Clinical TrialDocument7 pagesEffects of Probiotic Supplementation On Lipid Profile of Women With Rheumatoid Arthritis: A Randomized Placebo-Controlled Clinical Trialsufiah istthyNo ratings yet
- Ator Simvas OkDocument7 pagesAtor Simvas OkGatiNo ratings yet
- 1 s2.0 S0753332218367970 MainDocument10 pages1 s2.0 S0753332218367970 Maintrinda ireneNo ratings yet
- Standardized Laboratory Monitoring With Use of Isotretinoin in Acne - Hansen2016Document6 pagesStandardized Laboratory Monitoring With Use of Isotretinoin in Acne - Hansen2016Blu Punto ArtNo ratings yet
- Nutritional Status Among Peritoneal Dialysis Patients After Oral Supplement With ONCE Dialyze FormulaDocument7 pagesNutritional Status Among Peritoneal Dialysis Patients After Oral Supplement With ONCE Dialyze FormulanuvitaNo ratings yet
- Assessment of Quality of Life in A Double-Blind, Randomized Clinical Trial of Imidapril and Captopril For Hypertensive Chinese in TaiwanDocument7 pagesAssessment of Quality of Life in A Double-Blind, Randomized Clinical Trial of Imidapril and Captopril For Hypertensive Chinese in TaiwanSherllen ChandraNo ratings yet
- Original Article: A. Kashiwagi, H. Takahashi, H. Ishikawa, S. Yoshida, K. Kazuta, A. Utsuno & E. UeyamaDocument9 pagesOriginal Article: A. Kashiwagi, H. Takahashi, H. Ishikawa, S. Yoshida, K. Kazuta, A. Utsuno & E. UeyamadbcooperdkNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderFrom EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Clinical Pathway TB Org AnakDocument2 pagesClinical Pathway TB Org AnakRengganis PutriNo ratings yet
- Hubungan Kadar Hba1C Dengan Profil Lipid Pada Pasien Kaki Diabetik Di Rsup Prof. Dr. R. D. Kandou ManadoDocument6 pagesHubungan Kadar Hba1C Dengan Profil Lipid Pada Pasien Kaki Diabetik Di Rsup Prof. Dr. R. D. Kandou ManadoRengganis PutriNo ratings yet
- Habitual Coffee Intake, Genetic Polymorphisms, and Type 2 DiabetesDocument8 pagesHabitual Coffee Intake, Genetic Polymorphisms, and Type 2 DiabetesRengganis PutriNo ratings yet
- NCCLDocument5 pagesNCCLRengganis PutriNo ratings yet
- Kasus Tuberkulosis Dengan Riwayat Diabettes Mellitus Di Wilayah Prevalensi Tinggi Diabettes MellitusDocument8 pagesKasus Tuberkulosis Dengan Riwayat Diabettes Mellitus Di Wilayah Prevalensi Tinggi Diabettes MellitusRengganis PutriNo ratings yet
- Relationship Among Hba1C and Lipid Profile in Punajbi Type 2 Diabetic PopulationDocument4 pagesRelationship Among Hba1C and Lipid Profile in Punajbi Type 2 Diabetic PopulationRengganis PutriNo ratings yet
- WJH 8 1075Document13 pagesWJH 8 1075Rengganis PutriNo ratings yet
- Glucocorticoid-Induced Diabetes Mellitus: An Important But Overlooked ProblemDocument10 pagesGlucocorticoid-Induced Diabetes Mellitus: An Important But Overlooked ProblemRengganis PutriNo ratings yet
- No. Nama No RM DR2 Profil Lipid Status Hepatitis Ureum/ Creatinine Elektrolit CKMB Troponin I Asam UratDocument11 pagesNo. Nama No RM DR2 Profil Lipid Status Hepatitis Ureum/ Creatinine Elektrolit CKMB Troponin I Asam UratRengganis PutriNo ratings yet
- Review Article: Glucocorticoids and Type 2 Diabetes: From Physiology To PathologyDocument10 pagesReview Article: Glucocorticoids and Type 2 Diabetes: From Physiology To PathologyRengganis PutriNo ratings yet
- Gastroenterology: World Journal ofDocument19 pagesGastroenterology: World Journal ofRengganis PutriNo ratings yet
- 9b19d4c3aeaf6700970f468f6e200b5bDocument1 page9b19d4c3aeaf6700970f468f6e200b5bRengganis PutriNo ratings yet
- In Patients With Chronic Renal Failure: Long-Term Effects of A New Ketoacid-Amino Acid SupplementDocument6 pagesIn Patients With Chronic Renal Failure: Long-Term Effects of A New Ketoacid-Amino Acid SupplementRengganis PutriNo ratings yet
- Two Cases of Successful Pregnancy in Patients With Gitelman's SyndromeDocument6 pagesTwo Cases of Successful Pregnancy in Patients With Gitelman's SyndromeRengganis PutriNo ratings yet
- Kocyigit 2012Document8 pagesKocyigit 2012Rengganis PutriNo ratings yet
- JCTH 2016 00035Document8 pagesJCTH 2016 00035Rengganis PutriNo ratings yet
- Efficacy of The Essential Amino Acids and Keto-Analogues On The CKD Progression Rate in Real Practice in Russia - City Nephrology Registry Data For Outpatient ClinicDocument9 pagesEfficacy of The Essential Amino Acids and Keto-Analogues On The CKD Progression Rate in Real Practice in Russia - City Nephrology Registry Data For Outpatient ClinicRengganis PutriNo ratings yet
- Platelets-To-Lymphocyte Ratio Is A Good Predictor of Liver Fibrosis and Insulin Resistance in Hepatitis C Virus-Related Liver DiseaseDocument5 pagesPlatelets-To-Lymphocyte Ratio Is A Good Predictor of Liver Fibrosis and Insulin Resistance in Hepatitis C Virus-Related Liver DiseaseRengganis PutriNo ratings yet
- Na Hypo MyxedemaDocument4 pagesNa Hypo Myxedemaanderson roberto oliveira de sousaNo ratings yet
- Biomarkers in Kidney Disease PDFDocument1,212 pagesBiomarkers in Kidney Disease PDFAndreea AdaNo ratings yet
- Allied Health Science: B.Sc. Dialysis TechnologyDocument26 pagesAllied Health Science: B.Sc. Dialysis TechnologyNk Tower0% (1)
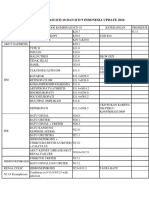
- Kode Kombinasi Icd 10 Dan Icd 9 Indonesia Update 2019Document11 pagesKode Kombinasi Icd 10 Dan Icd 9 Indonesia Update 2019[pml100% (1)
- Dukungan Keluarga Dan Faktor-Faktor Yang Mempengaruhi Kecemasan Pasien HemodialisaDocument8 pagesDukungan Keluarga Dan Faktor-Faktor Yang Mempengaruhi Kecemasan Pasien HemodialisaHelda Putri ArieskaNo ratings yet
- Hepatorrenal PrimerDocument17 pagesHepatorrenal PrimerDianaScandaOlveraCabreraNo ratings yet
- Hypomagnesemia & HypermagnesemiaDocument18 pagesHypomagnesemia & HypermagnesemiaLanzen DragneelNo ratings yet
- Nephrosclerosis PathophysiologyDocument14 pagesNephrosclerosis PathophysiologyAllene Paderanga0% (1)
- Renal BiopsyDocument4 pagesRenal BiopsyDeshan AdikariNo ratings yet
- Gambaran Dari: Acute Kidney Injury (Aki) : Dr. Hasan BasriDocument22 pagesGambaran Dari: Acute Kidney Injury (Aki) : Dr. Hasan BasriLiana Ika SuwandyNo ratings yet
- American Burn AssociationDocument13 pagesAmerican Burn AssociationRaka GhufranNo ratings yet
- Hubungan Asupan Zat Gizi Makro Terhadap Status GizDocument10 pagesHubungan Asupan Zat Gizi Makro Terhadap Status GizJulia KhaerunisaNo ratings yet
- Early Urine Output Predicts Graft Survival After KidneyDocument3 pagesEarly Urine Output Predicts Graft Survival After Kidneygiancarlor368No ratings yet
- BubreDocument10 pagesBubreharryNo ratings yet
- NURSING CARE PLAN - DialysisExpoDocument2 pagesNURSING CARE PLAN - DialysisExpoDANIELLA MALARANG MELNo ratings yet
- Dialysis ModuleDocument10 pagesDialysis Moduleapi-370434100No ratings yet
- Use of Interpreters For Non-Native English Speaking Kidney Allograft Recipients and Outcomes After Kidney TransplantationDocument6 pagesUse of Interpreters For Non-Native English Speaking Kidney Allograft Recipients and Outcomes After Kidney TransplantationPeertechz Publications Inc.No ratings yet
- Glucovance Tablet Salut Selaput 500 mg-5 MG - Metformin Hidroklorida-Glibenclaminde - DKL1715809217C1 - 2021 - 0Document16 pagesGlucovance Tablet Salut Selaput 500 mg-5 MG - Metformin Hidroklorida-Glibenclaminde - DKL1715809217C1 - 2021 - 0Felesia MissyNo ratings yet
- FPTP - Amoxicillin - Clavulanic Acid in Cats With & Without Chronic Kidney DiseaseDocument2 pagesFPTP - Amoxicillin - Clavulanic Acid in Cats With & Without Chronic Kidney DiseaseMabe AguirreNo ratings yet
- Onconephrology: Update in Anticancer Drug-Related NephrotoxicityDocument13 pagesOnconephrology: Update in Anticancer Drug-Related NephrotoxicityFreddy Shanner Chávez VásquezNo ratings yet
- ACP 100 PrimerDocument28 pagesACP 100 PrimerJennyNo ratings yet
- Etiology and Diagnosis of Prerenal Disease and Acute Tubular Necrosis in Acute Kidney Injury in Adults - UpToDateDocument22 pagesEtiology and Diagnosis of Prerenal Disease and Acute Tubular Necrosis in Acute Kidney Injury in Adults - UpToDatecuentaparatrabajosdelau10No ratings yet
- CNNDocument21 pagesCNNAshleyNo ratings yet
- Aubf RidleyDocument17 pagesAubf Ridleyabigail lausNo ratings yet
- Effect ModificationDocument64 pagesEffect ModificationDani Yitu MedanituNo ratings yet
- High Blood PressureDocument62 pagesHigh Blood PressureF SupportNo ratings yet
- A4.Fundamentals - 25item With RationaleDocument4 pagesA4.Fundamentals - 25item With RationaleBlardy Falking You Benchod BlardyNo ratings yet
- Jurnal Tentang GinjalDocument5 pagesJurnal Tentang GinjalnaveenNo ratings yet