Download as pdf or txt
You might also like
- Foundation of Special and Inclusive Education Post TestDocument12 pagesFoundation of Special and Inclusive Education Post TestNico John Bauzon Capua100% (10)
- Association of Adolescent HypertensionDocument7 pagesAssociation of Adolescent HypertensionluluNo ratings yet
- NIH Public Access: Author ManuscriptDocument20 pagesNIH Public Access: Author ManuscriptchameleonNo ratings yet
- Premature Atherosclerotic Cardiovascular Disease Trends in INcidence, Related Risk FactorDocument14 pagesPremature Atherosclerotic Cardiovascular Disease Trends in INcidence, Related Risk FactorAda DaiNo ratings yet
- Cardiovascular Disease in Children With Chronic Kidney Disease 2012Document8 pagesCardiovascular Disease in Children With Chronic Kidney Disease 2012fitriNo ratings yet
- The Prevalence of Resistant Hypertension Among TypDocument7 pagesThe Prevalence of Resistant Hypertension Among TypProfessor Kamel AjlouniNo ratings yet
- LIPITENSION: Interplay Between Dyslipidemia and HypertensionDocument6 pagesLIPITENSION: Interplay Between Dyslipidemia and HypertensionhimaNo ratings yet
- Burden of Heart Failure Patients in A Tertiary Level Cardiac HospitalDocument6 pagesBurden of Heart Failure Patients in A Tertiary Level Cardiac HospitalHasan Pallab MarufNo ratings yet
- NIH Public AccessDocument16 pagesNIH Public AccessaudiNo ratings yet
- Tgs Jurnal 1Document7 pagesTgs Jurnal 1suciNo ratings yet
- HipertensionDocument21 pagesHipertensionGrupo 3737No ratings yet
- Presion arteRIAL AcvDocument39 pagesPresion arteRIAL AcvOscar David Gamarra PerezNo ratings yet
- Age Risk Factors Heart FailureDocument9 pagesAge Risk Factors Heart FailureAnonymous NeRC5JYiSNo ratings yet
- Homocysteine, Ischemic Stroke, and Coronary Heart Disease in Hypertensive PatientsDocument12 pagesHomocysteine, Ischemic Stroke, and Coronary Heart Disease in Hypertensive PatientsIndah SundariNo ratings yet
- Psoriasis With Vascular DiseaseDocument4 pagesPsoriasis With Vascular Diseasemegh dutNo ratings yet
- 10 1161@hypertensionaha 117 09801Document17 pages10 1161@hypertensionaha 117 09801junediNo ratings yet
- J Jacc 2020 04 038Document10 pagesJ Jacc 2020 04 038manos iabanjiNo ratings yet
- Jurnal AnakDocument9 pagesJurnal AnakIndah IndrianiNo ratings yet
- Clinical Features of Transient Ischemic Attack or Ischemic Stroke Patients at High Recurrence Risk in IndonesiaDocument7 pagesClinical Features of Transient Ischemic Attack or Ischemic Stroke Patients at High Recurrence Risk in IndonesiaRivana カイドウ 雅治No ratings yet
- Strokeaha 119 024156Document7 pagesStrokeaha 119 024156Renan LopesNo ratings yet
- Nihms 368707Document19 pagesNihms 368707Moh SuprayogiNo ratings yet
- Orthostatic Hypotension Predicts Mortality in Middle-Aged AdultsDocument8 pagesOrthostatic Hypotension Predicts Mortality in Middle-Aged AdultsTaufiqur Rohman ChimeraNo ratings yet
- 8002 Vane0tDocument7 pages8002 Vane0tAbe AbeNo ratings yet
- Nejmoa 2109191Document12 pagesNejmoa 2109191Cristian NavaNo ratings yet
- Maturitas: SciencedirectDocument6 pagesMaturitas: SciencedirectDaniel QuirogaNo ratings yet
- Circulationaha 107 703389 PDFDocument7 pagesCirculationaha 107 703389 PDFlidia_694187376No ratings yet
- Cardiovascular Risk Factors in Childhood and Carotid Artery Intima-Media Thickness in AdulthoodDocument7 pagesCardiovascular Risk Factors in Childhood and Carotid Artery Intima-Media Thickness in AdulthoodDharmanna RathodNo ratings yet
- NIH Public Access: Type 2 Diabetes Mellitus and Hypertension: An UpdateDocument21 pagesNIH Public Access: Type 2 Diabetes Mellitus and Hypertension: An Updateyongky amaloNo ratings yet
- New Coronary Heart Disease Risk Factors - 2022 - AjmDocument2 pagesNew Coronary Heart Disease Risk Factors - 2022 - AjmBladimir CentenoNo ratings yet
- Jaha 113 000447Document11 pagesJaha 113 000447lilik eko pranantyoNo ratings yet
- Jurnal Observasional AnalitikDocument9 pagesJurnal Observasional AnalitikJethro BudimanNo ratings yet
- Manuscripts BestDocument15 pagesManuscripts BestAbdikarinNo ratings yet
- 2001 Relationship of Blood Pressure To 25-Year Mortality Due To Coronary Heart Disease, Cardiovascular Diseases, and All Causes in Young Adult MenDocument8 pages2001 Relationship of Blood Pressure To 25-Year Mortality Due To Coronary Heart Disease, Cardiovascular Diseases, and All Causes in Young Adult MencarlosNo ratings yet
- The Effect of Depression On Adherence To Antihypertensive Medications in Elderly Individuals With HypertensionDocument11 pagesThe Effect of Depression On Adherence To Antihypertensive Medications in Elderly Individuals With HypertensionNadia SariNo ratings yet
- Farmacocinetica e Genero - Grupo 2Document17 pagesFarmacocinetica e Genero - Grupo 2Paula ValeriNo ratings yet
- Association of Proteinuria and Incident Atrial Fibrillation in Patients With Diabetes Mellitus: A Population Based Senior Cohort StudyDocument10 pagesAssociation of Proteinuria and Incident Atrial Fibrillation in Patients With Diabetes Mellitus: A Population Based Senior Cohort StudydrkhengkiNo ratings yet
- 1998 Framingham - Prediction Coronary Hearth Disease Using Risk Factor CategoriesDocument12 pages1998 Framingham - Prediction Coronary Hearth Disease Using Risk Factor CategoriesJenny PinillaNo ratings yet
- New England Journal Medicine: The ofDocument9 pagesNew England Journal Medicine: The ofDias PradikaNo ratings yet
- Jamacardiology Dugani 2021 Oi 200091 1617381063.26688Document11 pagesJamacardiology Dugani 2021 Oi 200091 1617381063.26688SanNo ratings yet
- PneumoDocument6 pagesPneumoOlivia Chandra DeviNo ratings yet
- 1314-Article Text-2323-3-10-20190705Document7 pages1314-Article Text-2323-3-10-20190705VennyNo ratings yet
- Epidemiology, Aetiology, and Management of IschaemicDocument12 pagesEpidemiology, Aetiology, and Management of IschaemicKhairunNisaNo ratings yet
- Familial Clustering of Hypertensive Target Organ Damage in The CommunityDocument8 pagesFamilial Clustering of Hypertensive Target Organ Damage in The CommunityAnisa Iswari Pombaile-NgurawanNo ratings yet
- Diabetes, The Metabolic Syndrome, and Ischemic Stroke: Epidemiology and Possible MechanismsDocument10 pagesDiabetes, The Metabolic Syndrome, and Ischemic Stroke: Epidemiology and Possible MechanismsFelia AlyciaNo ratings yet
- CME - Are HemoglobinDocument4 pagesCME - Are HemoglobinIqmal AprilianNo ratings yet
- Correa 2018Document52 pagesCorrea 2018Esteban Matus MuñozNo ratings yet
- HIV Infection and Incidence of Cardiovascular Diseases: An Analysis of A Large Healthcare DatabaseDocument16 pagesHIV Infection and Incidence of Cardiovascular Diseases: An Analysis of A Large Healthcare DatabaseFajar SukmajayaNo ratings yet
- Investigation and Treatment of High Blood Pressure in Young PeopleDocument7 pagesInvestigation and Treatment of High Blood Pressure in Young PeopleTania Krisna PutriNo ratings yet
- Thyroid Status and Death Risk in US Veterans WithDocument13 pagesThyroid Status and Death Risk in US Veterans WithrojorojilloNo ratings yet
- Blood Pressure in Older Adults The Importance of FrailtyDocument14 pagesBlood Pressure in Older Adults The Importance of FrailtyolgaguerreroNo ratings yet
- Women and HTN-Wenger Et Al 2016Document7 pagesWomen and HTN-Wenger Et Al 2016Bumbum AtaunNo ratings yet
- Cotr134 19Document7 pagesCotr134 19tony wNo ratings yet
- Articulo 2Document7 pagesArticulo 2Gina GuisamanoNo ratings yet
- Coronary Heart Disease Is A Multifactorial Disease: N. PoulterDocument4 pagesCoronary Heart Disease Is A Multifactorial Disease: N. PoulterParamitha HarmanNo ratings yet
- Atherosclerosis: SciencedirectDocument7 pagesAtherosclerosis: SciencedirectRay HannaNo ratings yet
- Association Between Multiple Cardiovascular Risk FactorsDocument7 pagesAssociation Between Multiple Cardiovascular Risk FactorsRicardo CarminatoNo ratings yet
- Manejo de La HTA en Adulto MayorDocument11 pagesManejo de La HTA en Adulto MayorFacundo Ariel AlvarengaNo ratings yet
- Jaha 120 016671Document19 pagesJaha 120 016671SALMA HANINANo ratings yet
- Hypertension in Adolescents and Young Adults Referred To A Tertiary Hypertension Clinic in Cape Town, South AfricaDocument5 pagesHypertension in Adolescents and Young Adults Referred To A Tertiary Hypertension Clinic in Cape Town, South AfricahanifahNo ratings yet
- 2118 FullDocument10 pages2118 FullSergiu NiculitaNo ratings yet
- Gender Differences in the Pathogenesis and Management of Heart DiseaseFrom EverandGender Differences in the Pathogenesis and Management of Heart DiseaseNo ratings yet
- Diagnosis and Management of Bacterial ConjunctivitisDocument6 pagesDiagnosis and Management of Bacterial ConjunctivitisJonathan JoseNo ratings yet
- Ama Journal of EthicsDocument5 pagesAma Journal of EthicsJonathan JoseNo ratings yet
- Nawanto A Prastowo Departemen Fisiologi FK AtmajayaDocument27 pagesNawanto A Prastowo Departemen Fisiologi FK AtmajayaJonathan JoseNo ratings yet
- Oxygen TherapyDocument64 pagesOxygen TherapyJonathan JoseNo ratings yet
- Isolation GuidelinesDocument203 pagesIsolation GuidelinesAlifia TrisnaningrumNo ratings yet
- MD LogbookDocument47 pagesMD LogbookAhmad fayazNo ratings yet
- Solid Dosage Forms in Unani System of Medicine AnDocument7 pagesSolid Dosage Forms in Unani System of Medicine AnSiddharth JainNo ratings yet
- LBM 6 Blok 20 SGD 1Document8 pagesLBM 6 Blok 20 SGD 1Ani LabibahNo ratings yet
- Cancer Immunotherapy: Dra. Cristina Nadal Oncologia Medica Hospital Clinic BarcelonaDocument63 pagesCancer Immunotherapy: Dra. Cristina Nadal Oncologia Medica Hospital Clinic BarcelonaOlga Peña HernandezNo ratings yet
- Benito Lorenzo V Gsis LaborDocument2 pagesBenito Lorenzo V Gsis LaborAirra MaeNo ratings yet
- Nursing Practice IVDocument16 pagesNursing Practice IVJohn wewNo ratings yet
- A Case Study On Madhumeha W.S.R To Type 2 Diabetes Mellitus Treated With Chandra Kala GudikaDocument7 pagesA Case Study On Madhumeha W.S.R To Type 2 Diabetes Mellitus Treated With Chandra Kala GudikaIJAR JOURNALNo ratings yet
- Jurnal SkizofreniaDocument9 pagesJurnal SkizofreniaAbdul HamidNo ratings yet
- Difference Between Genetic and Non Genetic RnaDocument1 pageDifference Between Genetic and Non Genetic RnaMatin Ahmad KhanNo ratings yet
- Epidemiology and Treatment of Multiple Sclerosis in Elderly PopulationsDocument14 pagesEpidemiology and Treatment of Multiple Sclerosis in Elderly PopulationsLütfiye ÇiftçiNo ratings yet
- Supliment-2022 RJC PDFDocument320 pagesSupliment-2022 RJC PDFSimona IonitaNo ratings yet
- Cervical CancerDocument2 pagesCervical CancerLicio LentimoNo ratings yet
- SITXFSA001 Student Assessment TasksDocument24 pagesSITXFSA001 Student Assessment TasksMukta AktherNo ratings yet
- Propagation Techniques in PepperDocument4 pagesPropagation Techniques in PepperDr.Eswara Reddy SiddareddyNo ratings yet
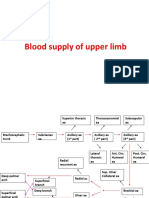
- Blood Supply of Upper LimbDocument36 pagesBlood Supply of Upper Limbteklay100% (2)
- Republic v. Cagandahan, G.R. No. 166676, 12 September 2008Document1 pageRepublic v. Cagandahan, G.R. No. 166676, 12 September 2008Jovelan V. EscañoNo ratings yet
- "Double Stigma": Forced Sterilization of Women Living With HIV in Kenya and NamibiaDocument4 pages"Double Stigma": Forced Sterilization of Women Living With HIV in Kenya and NamibiaPopulation & Development Program (PopDev)No ratings yet
- Nike 2021 Code Leadership Standards - FinalDocument131 pagesNike 2021 Code Leadership Standards - FinalJonathan Alexander Catú PérezNo ratings yet
- Diagnosis and Correction of Uterine Torsion in Cattle and BuffaloesDocument13 pagesDiagnosis and Correction of Uterine Torsion in Cattle and Buffaloesgnpoba100% (12)
- Argumentati Ve Essay: Sri Rejeki, S.P D., M.PDDocument11 pagesArgumentati Ve Essay: Sri Rejeki, S.P D., M.PDRahma OktaviaNo ratings yet
- Activity 18 AgingDocument27 pagesActivity 18 AgingKendrix Aguiluz FlorendoNo ratings yet
- CV Prof. DR., Zairin Noor (English) - March 2019Document19 pagesCV Prof. DR., Zairin Noor (English) - March 2019Nina EvelynaNo ratings yet
- Gmail Maxicare EReady Advance PDFDocument7 pagesGmail Maxicare EReady Advance PDFShirelyNo ratings yet
- Addiction Recovery ManagementDocument71 pagesAddiction Recovery ManagementThe Stacie Mathewson FoundationNo ratings yet
- Cocoa Pest ManagementDocument13 pagesCocoa Pest ManagementAprilia WilonaNo ratings yet
- Hoërskool Roodepoort: COVID-19 PolicyDocument24 pagesHoërskool Roodepoort: COVID-19 PolicyScarfacembali MbaliNo ratings yet
- Case 2 ECTOPIC PREGNANCY MahilumDocument27 pagesCase 2 ECTOPIC PREGNANCY MahilumEduard GarchitorenaNo ratings yet
- Herpetic StomatitisDocument21 pagesHerpetic StomatitisZulfahmi RizkiNo ratings yet