Professional Documents
Culture Documents
Pedersen 2001
Pedersen 2001
Uploaded by
anca_szaboCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Pedersen 2001
Pedersen 2001
Uploaded by
anca_szaboCopyright:
Available Formats
ORIGINAL ARTICLE
Evidence of a Dose-Response Relationship
Between Urbanicity During Upbringing
and Schizophrenia Risk
Carsten Bøcker Pedersen, MSc; Preben Bo Mortensen, DMSc
Background: Many studies have demonstrated that an Results: Individuals living in a higher degree of urbaniza-
urban birth or upbringing increases schizophrenia risk, tion than 5 years earlier had a 1.40-fold (95% confidence in-
but no studies have been able to distinguish between these terval, 1.28-1.51) increased risk, while individuals living in
effects. The objectives of this study were to discriminate a lower degree of urbanization than 5 years earlier had a 0.82-
the effect of urbanicity at birth from an effect of urban- fold (95% confidence interval, 0.77-0.88) decreased risk of
icity during upbringing, and to identify particularly vul- schizophrenia. For fixed urbanicity at the 15th birthday, risk
nerable age periods and a possible dose-response rela- increased with increasing degree of urbanization at birth.
tionship between urbanicity during upbringing and Furthermore, the more years lived in the higher the degree
schizophrenia risk. of urbanization, the greater the risk. Individuals who lived
their first 15 years in the highest category of the 5-level ur-
Methods: Using data from the Danish Civil Registra- banicityhada2.75-fold(95%confidenceinterval,2.31-3.28)
tion System, we established a population-based cohort increased risk of schizophrenia.
of 1.89 million people, which included information on
place of birth, place of residence during upbringing, and Conclusion: Continuous, or repeated, exposures dur-
the accumulated number of years lived in each category ing upbringing that occur more frequently in urbanized
of the 5-level degree of urbanization during upbringing. areas may be responsible for the association between ur-
Schizophrenia in cohort members and mental illness in banization and schizophrenia risk.
a parent or sibling were identified by linkage with the
Danish Psychiatric Central Register. Arch Gen Psychiatry. 2001;58:1039-1046
A
LTHOUGH A family history banicity at birth and urbanicity during up-
of schizophrenia is the best bringing are strongly associated, a large
established risk factor for study population, including information
the disease, 1 it may ac- on place of birth and upbringing, is needed
count for only a small pro- to discriminate the effect of urbanicity at
portion of the population occurrence of birth from an effect of urbanicity during
schizophrenia.2,3 Other factors, such as ur- upbringing, and vice versa.7 To our knowl-
banicity at birth and upbringing, are as- edge, studies based on such data have not
sociated with an increased risk also,2-4 and been published previously. This study uses
causal factors underlying this association a large population-based sample of the
may account for a much higher propor- Danish population, including complete in-
tion of the population occurrence of the formation on all permanent addresses at
disease. Although the causes of these ur- which cohort members had lived since
ban-rural differences are unknown, they 1971, to investigate the relative impact of
have been hypothesized to include, eg, ob- urbanicity at birth and during upbring-
stetric complications, infections, diet, toxic ing. Furthermore, the hypothesis that there
exposures, household crowding, breast- is a dose-response relationship between
From the Department of feeding, social class, and an artifact due to urbanicity during upbringing and schizo-
Psychiatric Demography, migration.5,6 phrenia risk is investigated.
Institute for Basic Psychiatric
To reduce the number of possible
Research, Aarhus University
Hospital, Risskov, and the candidates responsible for this associa- RESULTS
National Centre for tion, the objective of this study was to in-
Register-Based Research, vestigate at what age during upbringing A total of 8235 persons developed schizo-
Aarhus University, Aarhus C, (including birth) children were most vul- phrenia during the 27.1 million person-
Denmark. nerable to urbanicity. However, since ur- years of follow-up (Table 1). Urbanicity
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, NOV 2001 WWW.ARCHGENPSYCHIATRY.COM
1039
©2001 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a University of St. Andrews Library User on 05/19/2015
PARTICIPANTS AND METHODS million admissions. From 1995 onward, information on
outpatient visits to psychiatric departments was included
STUDY POPULATION in the register. There are no private psychiatric depart-
ments in Denmark. From April 1, 1969, to December 31,
We used data from the Danish Civil Registration System8 1993, the diagnostic system used was the International
to obtain a large and representative set of data on Danish Classification of Diseases, 8th Revision (ICD-8),10 and from
persons, which for all persons included current and his- January 1, 1994, the diagnostic system used was the Inter-
torical information on address in Denmark and Greenland national Classification of Diseases, 10th Revision (ICD-10).11
and emigrations and immigrations to and from other Cohort members were classified as having schizophrenia if
countries, together with exact dates for changes of resi- they had been admitted to a psychiatric hospital or had
dence. All citizens in Denmark are obliged to inform the been in outpatient care with a diagnosis of the disorder
authorities about any change of permanent address within (ICD-8 code 295 or ICD-10 code F20). The date of onset
5 days. Failure to supply this information will result in was defined as the first day of the first contact (inpatient or
the inability to receive a supplementary benefit (eg, outpatient) with a diagnosis of schizophrenia. Parents and
unemployment, sickness or disablement benefits, and siblings were categorized hierarchically with a history of
educational aid from public funds), to go to a day nurs- schizophrenia (ICD-8 code 295 or ICD-10 code F20),
ery, to go to nursery school, to attend primary and lower schizophrenialike psychoses (ICD-8 code 297, 298.39, or
secondary school, to obtain free national health care, and 301.83 or ICD-10 codes F21-F29), or other mental disor-
to obtain a tax deduction card (required to have paid ders (any ICD-8 or ICD-10 diagnosis) if they had been
work). Therefore, it is unlikely that this mandatory infor- admitted to a psychiatric hospital or had been in outpa-
mation is not reported. This information is complete from tient care with one of these diagnoses.
January 1, 1971. Our study cohort consists of all persons
with known maternal identity who were born in Denmark ASSESSMENT OF DEGREE OF URBANIZATION
between January 1, 1956, and December 31, 1983, and
who were alive at the 15th birthday (1.89 million The 276 municipalities in Denmark were classified accord-
persons). ing to the degree of urbanization12: capital, capital suburb,
provincial city with more than 100000 inhabitants, pro-
ASSESSMENT OF SCHIZOPHRENIA AND vincial town with more than 10000 inhabitants, or rural
MENTAL ILLNESS IN A PARENT OR SIBLING areas. Denmark is a small homogeneous country with a
population of 5.3 million people and a total area of 43000
The study population and their mothers, fathers, and sib- km2. The capital, capital suburb, provincial city, provin-
lings were linked with the Danish Psychiatric Central Reg- cial town, and rural area hold 5220, 845, 470, 180, and 55
ister,9 which has been computerized since April 1, 1969. people per square kilometer, respectively.13 Distances are
The Danish Psychiatric Central Register contains data on small in Denmark; most people live within 25 km of a city
all admissions to Danish psychiatric inpatient facilities and with more than 30000 inhabitants, and are even closer to
includes data on approximately 450000 persons and 1.6 a psychiatric hospital.
at birth is known for all persons, whereas information increasing age and increasing number of changes. Over-
on urbanicity at a given age depends on the year of birth, all, these 4 variables had a significant effect (P⬍.001),
as information on place of residence was accessible only and the model with these 4 variables had a significantly
from 1971 onward. better fit than the model in which the change of munici-
pality was described in 1-year bands (Figure 1).
CHANGE OF RESIDENCE
URBANICITY IN 1-YEAR AGE POINTS
The relative risk of schizophrenia increases with increas-
ing age at change of the address or the municipality Individuals who at birth lived in the capital, the capital
(Figure 1). However, change of address within the same suburb, the provincial city, or the provincial town had a
municipality had no influence on schizophrenia risk. Fur- relative risk of schizophrenia of 2.24 (95% confidence
thermore, the effect of changes of the municipality within interval [CI], 1.92-2.61), 1.71 (95% CI, 1.46-2.00), 1.62
the same degree of urbanization increased with increas- (95% CI, 1.36-1.92), and 1.27 (95% CI, 1.10-1.47), re-
ing age (data not shown). Therefore, the confounding spectively, compared with individuals who lived in the
effect of change of residence can be described by changes rural area (Figure 2). This difference remained almost
of the municipality. constant for ages from birth to the 15th birthday.
We classified change of municipality by 4 vari-
ables, counting the number of changes of the munici- RELATIVE URBANICITY AT SUCCESSIVE AGES
pality from birth to the 5th birthday, from the 5th to the
10th birthday, from the 10th to the 13th birthday, and Among those who were born in the capital suburb, those
from the 13th to the 15th birthday (Table 2). Com- who at the 5th birthday lived in a higher, the same, or a
pared with persons with no changes of the municipality lower degree of urbanization than at birth had a relative
from the 5th to the 10th birthday, those with one change risk of schizophrenia of 2.01, 1.82, or 1.55, respectively
of the municipality had a relative risk of 1.18. The effect (Table 3, first adjustment), compared with those who
of the number of changes of municipality increased with at birth and at the 5th birthday lived in the rural area. In
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, NOV 2001 WWW.ARCHGENPSYCHIATRY.COM
1040
©2001 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a University of St. Andrews Library User on 05/19/2015
STUDY DESIGN mental illness in a parent was treated as a variable that was in-
dependent of time. Age was categorized using the following
Using data from the Danish Civil Registration System, for each cut points: 15, 16, 17, 18, 19, 20, 22, 24, 26, 28, 30, 35, and
person in the cohort we obtained information on (1) the de- 40 years. Calendar year was categorized using the following
gree of urbanization in 1-year age points from birth to the cut points: 1971, 1976, 1979, 1982, 1985, 1988, 1991, 1993,
15th birthday; (2) the number of changes of the address, the 1994, 1995, 1996, 1997, and 1998. P values were based on find-
municipality, and the degree of urbanization in 1-year age ings from the likelihood ratio tests, and 95% confidence lim-
bands from birth to the 15th birthday; and (3) the accumu- its were calculated by the Wald test.16 The adjusted-score test17
lated number of years each person born in 1971 or later had suggested that the regression models were not subject to over-
been living in each degree of urbanization from birth to the dispersion. Apart from the reduction in the size of the study
5th birthday, from the 5th to the 10th birthday, and from the population, omission of adjustment for seasonality, maternal
10th to the 15th birthday. The reason we considered change and paternal age, and the inclusion of information on perma-
of residence was that initial analyses suggested that to inves- nent address for all cohort members since 1971, the material
tigate the association between schizophrenia and urbaniza- described is identical to that used in our previous study,3 where
tion we had to control for an increased risk associated with we found that the effects of urbanicity at birth and mental ill-
change of residence. Furthermore, to avoid the potential im- ness in a family member were invariant to the diagnostic sys-
pact of selective migration to cities in the prodromal phase tem and the inclusion of outpatient information.
of schizophrenia, only residence during upbringing was con- To evaluate the hypothesis that there is a dose-response
sidered. By upbringing, we are referring to the period from relationship between urbanicity during upbringing and
birth to the 15th birthday. Information on urbanicity at birth, schizophrenia risk, we used a statistical model for the accu-
urbanicity during upbringing, and change of residence is in- mulated number of years each person had been living in the
dependent of the disease status. A total of 1.89 million per- capital, the capital suburb, the provincial city, and the pro-
sons were followed up from their 15th birthday or from April vincial town. It implies that those who always lived in the
1, 1970, whichever came later, until the date of onset of schizo- rural area during upbringing were chosen as the reference
phrenia, the date of death, the date of emigration, or Decem- category, and that the effect of these 4 variables measures
ber 31, 1998, whichever came first. the effect of exchanging upbringing in the rural area with up-
bringing in the corresponding degree of urbanization.
STATISTICAL ANALYSES By urbanicity at some age point, we refer only to the
degree of urbanization at the given age point, whereas by
The relative risk of schizophrenia was estimated by log- urbanicity during upbringing, we refer to the full se-
linear Poisson regression14 with the GENMOD procedure, us- quence of degrees of urbanization of places of residence from
ing SAS statistical software, version 6.12.15 All relative risks birth to the 15th birthday. Furthermore, by a model for ur-
were adjusted for age and its interaction with sex, calendar banicity during upbringing, we refer to a model for the ac-
year, and history of mental illness in a parent or sibling. Age, cumulated number of years each person has lived in the
calendar year, and history of mental illness in siblings were capital, the capital suburb, the provincial city, and the pro-
treated as time-dependent variables,16 whereas history of vincial town during upbringing.
general, living in a higher degree of urbanization at the banicity at the 15th birthday, risk increases with increas-
5th birthday than at birth increased risk, while living in ing degree of urbanization at place of birth (data not
a lower degree of urbanization at the 5th birthday than shown).
at birth decreased risk. This tendency was not modified
by adjustment for change of the municipality (Table 3, URBANICITY DURING UPBRINGING
second adjustment).
Living in a higher or lower degree of urbanization at A total of 807 000 people in the cohort were born in
the 10th birthday than at the 5th birthday increased risk, 1971 or later and, therefore, these people had accessible
but risk was increased more if living in a higher than in a information on urbanicity during upbringing. Among
lower degree of urbanization (Table 3, first adjustment). them, 1553 persons developed schizophrenia during
When these estimates were adjusted for the number of the 5.6 million person-years at risk (Table 4). Com-
changes of the municipality, living in a higher degree of pared with those who had always been living in the ru-
urbanization at the 10th birthday than at the 5th birth- ral area, those who had always been living in the capital
day increased risk, while living in a lower degree of ur- had a relative risk of 2.62. In general, the more years
banization at the 10th birthday than at the 5th birthday lived in the higher the degree of urbanization, the
decreased risk (Table 3, second adjustment). The same greater the risk of schizophrenia.
tendency was found when comparing place of residence Estimates in the second column of Table 5 mea-
at the 10th birthday with place of residence at the 15th sure the risk per year associated with exchanging resi-
birthday. Overall, living in a higher degree of urbaniza- dence in the rural area with residence in each degree of
tion than 5 years earlier increased risk 1.40-fold (95% urbanization, and estimates in the third column mea-
CI, 1.28-1.51), while living in a lower degree of urban- sure the risk associated with exchanging all residence (15
ization than 5 years earlier decreased risk 0.82-fold (95% years) in the rural area with residence in each degree of
CI, 0.77-0.88). Furthermore, for fixed urbanicity at birth, urbanization. The relative risk per 15 years is calculated
risk increases with increasing degree of urbanization at by raising the relative risk per year to the 15th power,
place of residence at the 15th birthday, and for fixed ur- eg, 1.069715 = 2.75. Compared with those who had al-
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, NOV 2001 WWW.ARCHGENPSYCHIATRY.COM
1041
©2001 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a University of St. Andrews Library User on 05/19/2015
1.75
Table 1. Distribution of 8235 Cases of Schizophrenia and A
27.1 Million Person-years at Risk in a Population-Based
Cohort of 1.89 Million Danish People
Relative Risk of Schizophrenia
1.50
No. of
Variable Cases Person-years
1.25
Total 8235 27 115 224
Sex
Male 5462 14 150 781
1.00
Female 2773 12 964 444
History
Maternal
Schizophrenia 234 86 524 0.75
Schizophrenialike psychoses 257 196 298
Other mental disorders 1323 2 067 383 1.50
B
Mother not affected 6421 24 765 019
Paternal
Relative Risk of Schizophrenia
Schizophrenia 98 45 980
Schizophrenialike psychoses 106 96 483 1.25
Other mental disorders 888 1 573 112
Unknown father 640 990 119
Father not affected 6503 24 409 531
Siblings
1.00
Schizophrenia 284 105 515
Schizophrenialike psychoses 115 80 535
Other mental disorders 546 705 134
No affected siblings 7290 26 224 040
Urbanicity 0.75
At birth
Capital 2594 5 008 126 1.50
C
Capital suburb 793 2 328 013
Provincial city 1073 3 451 055
Relative Risk of Schizophrenia
Provincial town 2375 9 405 666
Rural area 1400 6 922 365 1.25
At the 5th birthday
Capital 559 940 862
Capital suburb 635 1 720 492
Provincial city 449 1 239 834
1.00
Provincial town 836 3 220 339
Rural area 822 4 114 556
Other countries 29 80 010
Unknown 6 7909
Unaccessible information 4893 15 775 738 0.75
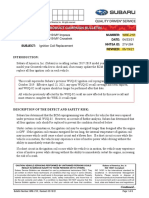
At the 10th birthday 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Capital 913 1 427 445 Age, y
Capital suburb 1139 2 915 199
Provincial city 660 1 988 951 Figure 1. Relative risk of schizophrenia associated with age and change of
the municipality (A), the address within the same municipality (B), and the
Provincial town 1416 5 369 404
address (C). Those without change of the municipality, the address within
Rural area 1602 7 224 640 the same municipality, or the address are used as the baseline category
Other countries 47 131 801 (relative risk = 1.00). Vertical lines indicate 95% confidence intervals. Age 0
Unknown 10 18 555 indicates the age period from birth to the first birthday, etc. Estimates of
Unaccessible information 2448 8 039 228 relative risks were adjusted for age and its interaction with sex, calendar
At the 15th birthday year, and mental illness in a parent or sibling.
Capital 1240 2 011 689
Capital suburb 1559 4 017 883
Provincial city 896 2 760 442 pared with a person who had always been living in the
Provincial town 2020 7 629 875
rural area (not accounting for the increased risk associ-
Rural area 2453 10 547 958
Other countries 57 126 824 ated with change of residence). In general, risk in-
Unknown 10 20 553 creases with increasing degree of urbanization, and in-
herent in the log-linear model is that risk increases with
increasing number of years lived in each degree of ur-
banization. The categorical model (Table 4) could be sim-
ways been living in the rural area during upbringing, those plified to the log-linear model (Table 5) for urbanicity
who had always been living in the capital during up- during upbringing (P =.63). In the rest of this article, we
bringing had a relative risk of 2.75. According to this use the log-linear model to describe the association be-
model, a person who had been living 7 years in the capi- tween schizophrenia and urbanization. Furthermore, this
tal and 8 years in the capital suburb during upbringing model had a significantly better fit than any of the mod-
had a relative risk of 2.12 (1.06977 ⫻ 1.03558) com- els for the modifying effects of urbanicity between the
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, NOV 2001 WWW.ARCHGENPSYCHIATRY.COM
1042
©2001 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a University of St. Andrews Library User on 05/19/2015
Table 2. Adjusted Relative Risks According to Number of Changes of Municipality in a Population-Based Cohort
of 1.89 Million Danish People*
Relative Risk
No. of Changes of Municipality No. of Cases Person-years (95% Confidence Interval)†
From birth to the 5th birthday (P = .34)
0 1004 3 890 119 1.00‡
1 328 1 123 412 0.92 (0.82-1.05)
2 131 376 364 0.97 (0.80-1.16)
ⱖ3 90 217 165 0.91 (0.73-1.13)
From the 5th to the 10th birthday (P⬍.001)
0 2390 9 119 282 1.00‡
1 601 1 570 244 1.18 (1.07-1.29)
2 216 433 266 1.29 (1.12-1.49)
ⱖ3 135 216 693 1.28 (1.07-1.54)
From the 10th to the 13th birthday (P⬍.001)
0 4845 17 244 968 1.00‡
1 665 1 455 258 1.16 (1.07-1.26)
2 199 283 956 1.40 (1.21-1.62)
ⱖ3 78 91 815 1.36 (1.08-1.70)
From the 13th to the 15th birthday (P⬍.001)
0 6324 22 485 003 1.00‡
1 696 1 240 162 1.45 (1.34-1.57)
2 184 217 825 1.79 (1.54-2.08)
ⱖ3 76 55 656 2.49 (1.97-3.13)
*Categories with unaccessible information are not shown.
†Estimates of relative risk were adjusted for age and its interaction with sex, calendar year, urbanicity at birth, mental illness in a parent or sibling, and change
of the municipality.
‡Referent.
successive age points of birth, 5th, 10th, and 15th birth-
Capital Provincial City Rural Area
day (Table 3).
Capital Suburb Provincial Town
When urbanicity at birth and urbanicity during
upbringing were adjusted mutually, the effect of urban- 2.75
icity at birth vanished (P = .80), while the effect of ur-
banicity during upbringing was not modified and re- 2.50
Realative Risk of Schizophrenia
mained strongly significant (P⬍.001). This means that
2.00
urbanicity during upbringing explains the effect of ur-
banicity at birth, ie, urbanicity at birth is a proxy for 1.75
urbanicity during upbringing. The effect of urbanicity dur-
ing upbringing did not differ significantly by age at resi- 1.50
dence (P=.08) or sex (P= .79) (data not shown), mean-
1.25
ing that there was no evidence of age at residence or sex
differences in the vulnerability to upbringing in urban- 1.00
ized areas. Furthermore, there were no urban-rural dif-
ferences in age of onset (P = .21). 0.75
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
In any of the models presented herein, the effect of Age, y
change of municipality remained constant.
Figure 2. Relative risk of schizophrenia according to urbanicity and age at
residence. Urbanicity from birth to the 15th birthday enters separately in
COMMENT these 16 models. Age 0 indicates the time at birth, etc. Vertical lines indicate
95% confidence intervals. To avoid the confidence intervals from overlapping
graphically, the age scale for the capital suburb was moved slightly to the left
Places of residence at nearby ages are strongly associ- and the age scale for the provincial city was moved slightly to the right.
ated, meaning that for most people, place of residence Estimates of relative risks were adjusted for age and its interaction with sex,
at the fifth birthday was identical to place of residence calendar year of diagnosis, and mental illness in a parent or sibling. Further
adjustment for change of the municipality would reduce the effect of
at the fourth and sixth birthday. This correlation im- urbanicity only slightly.
pedes the interpretation of the finding of the constant effect
of urbanicity according to age (Figure 2). However, sup-
pose children were only vulnerable to urbanicity at the birthday. Furthermore, because of attenuation caused by
fifth birthday and not to urbanicity at birth or urbanic- misclassification,18 the effect of this proxy variable would
ity at any other age, then the reason many studies (eg, be lower than the effect of urbanicity at the fifth birth-
Mortensen and others2,3,6) have found an association be- day. Therefore, if children were most fragile to urban-
tween urbanicity at birth and schizophrenia risk is that icity at some single age point during upbringing, then
urbanicity at birth is a proxy for urbanicity at the fifth urbanicity would have a higher effect for this age point
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, NOV 2001 WWW.ARCHGENPSYCHIATRY.COM
1043
©2001 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a University of St. Andrews Library User on 05/19/2015
Table 3. Adjusted Relative Risk of Schizophrenia According to Urbanicity in a Population-Based Cohort of 1.89 Million Danish People
Relative Degree of Urbanization at Place of Residence 5 y Later*
Relative Risk (95% Confidence Interval)
No. of Cases First Adjustment† Second Adjustment‡
Urbanicity Higher Same Lower Higher Same Lower Higher Same Lower
At birth
Capital ... 503 430 ... 2.75 (2.39-3.17) 2.08 (1.80-2.41) ... 2.53 (2.19-2.92) 1.94 (1.68-2.25)
Capital suburb 22 268 56 2.01 (1.30-3.10) 1.82 (1.55-2.15) 1.55 (1.16-2.06) 1.82 (1.18-2.81) 1.74 (1.48-2.05) 1.44 (1.08-1.92)
Provincial city 9 367 124 1.63 (0.84-3.16) 1.94 (1.67-2.25) 1.46 (1.19-1.80) 1.44 (0.74-2.79) 1.92 (1.65-2.24) 1.41 (1.14-1.73)
Provincial town 117 658 332 2.21 (1.79-2.74) 1.37 (1.20-1.57) 1.20 (1.03-1.40) 2.02 (1.63-2.51) 1.35 (1.18-1.55) 1.17 (1.00-1.37)
Rural area 100 315 ... 1.95 (1.56-2.45) 1.00§ ... 1.83 (1.46-2.30) 1.00§ ...
At the fifth birthday
Capital ... 434 117 ... 2.70 (2.39-3.04) 2.04 (1.67-2.48) ... 2.63 (2.33-2.96) 1.53 (1.22-1.90)
Capital suburb 32 514 84 2.74 (1.92-3.90) 1.72 (1.54-1.93) 2.17 (1.73-2.72) 2.04 (1.41-2.95) 1.67 (1.49-1.87) 1.62 (1.26-2.07)
Provincial city 9 375 62 3.01 (1.56-5.82) 1.79 (1.58-2.03) 2.01 (1.55-2.61) 2.16 (1.11-4.21) 1.84 (1.63-2.09) 1.53 (1.16-2.02)
Provincial town 43 707 85 2.41 (1.77-3.27) 1.28 (1.16-1.42) 1.54 (1.23-1.92) 1.78 (1.29-2.46) 1.30 (1.17-1.45) 1.16 (0.90-1.48)
Rural area 116 704 ... 1.92 (1.58-2.34) 1.00§ ... 1.45 (1.16-1.81) 1.00§ ...
At the 10th birthday
Capital ... 725 179 ... 2.38 (2.17-2.60) 2.61 (2.23-3.05) ... 2.41 (2.20-2.64) 1.93 (1.63-2.28)
Capital suburb 58 955 114 3.14 (2.42-4.09) 1.61 (1.49-1.75) 1.99 (1.64-2.41) 2.26 (1.73-2.96) 1.60 (1.47-1.73) 1.41 (1.16-1.73)
Provincial city 7 582 70 2.40 (1.14-5.04) 1.47 (1.34-1.62) 1.96 (1.54-2.50) 1.70 (0.81-3.59) 1.53 (1.39-1.69) 1.45 (1.13-1.86)
Provincial town 53 1242 115 2.14 (1.63-2.82) 1.16 (1.07-1.25) 1.59 (1.31-1.92) 1.52 (1.14-2.01) 1.18 (1.10-1.28) 1.15 (0.94-1.40)
Rural area 180 1417 ... 1.94 (1.66-2.27) 1.00§ ... 1.37 (1.16-1.62) 1.00§ ...
*Ellipses indicate data not applicable.
†Estimates of relative risk were adjusted for sex and its interaction with age, calendar year, and mental illness in a parent or sibling.
‡Estimates of relative risk were adjusted for all variables in the first adjustment and for change of the municipality.
§Referent.
than for the nearby age points. However, since the effect dren at or around birth to factors influencing children
of urbanicity (Figure 2) does not depend on age at resi- continuously, or repeatedly, throughout upbringing. Fac-
dence, these data show no indication of any ages par- tors such as obstetric complications, prenatal infec-
ticularly vulnerable to residence in urbanized areas dur- tions, and breastfeeding are, therefore, less likely expla-
ing upbringing. nations for these urban-rural differences, although they
The risk associated with 15 years of residence in any may well affect risk independently of urbanicity. Also,
urbanicity was greater than the risk associated with liv- studies have suggested that household crowding,19 ob-
ing in the same urbanicity as 5 years earlier (Table 3, sec- stetric complications,20 parental social class,21 and pre-
ond adjustment, and Table 5), which in turn was greater natal exposure to influenza22 do not explain the urban-
than the effect of urbanicity at birth or at some age point rural differences in schizophrenia risk.
(Figure 2). This indicates that the greater the refine- When Danish children move from one municipal-
ment of the modeling of urbanicity, the greater the risk, ity to another, they usually change school. Therefore, it
and that not only urbanicity at birth or at some age point is interesting that change of municipality had a greater
but also the effect of living in the same urbanicity as 5 effect on schizophrenia risk than change of address, while
years earlier are proxies for urbanicity during upbring- change of address within the same municipality had no
ing. In conclusion, the log-linear model for the accumu- effect (Figure 1). We can only speculate regarding the
lated number of years lived in each degree of urbaniza- underlying causes of these findings; however, they may
tion during upbringing is the best model describing the be related to social maladjustment in preschizophrenic
association between urbanization and schizophrenia risk. children, the stress of making new friends, and the fact
Furthermore, it provides evidence of a dose-response re- that preschizophrenic children are more anxious in new
lationship between urbanicity during upbringing and environments.23,24 Life events, such as parental death, pa-
schizophrenia risk. rental divorce, or change in social class, are possible but
The possible etiological factors that might explain less likely explanations as they are not related to change
our findings remain unknown. However, the finding of of the municipality only.
a dose-response relationship between schizophrenia risk It is extremely unlikely that selective migration or
and urbanicity during upbringing lends support to a causal urban-rural differences in the availability of psychiatric
association. Our findings may suggest that constant, cu- services explain the effect of urbanicity at birth; for
mulative, or repeated exposures during upbringing oc- fixed urbanicity at the 15th birthday, risk increases
curring more frequently in urbanized areas are respon- with increasing degree of urbanization at place of birth,
sible for the association between urbanization and and there was no evidence that age at onset was modi-
schizophrenia risk. The potential explanations for the ur- fied by urbanicity during upbringing, ie, there were no
ban-rural differences shift from factors influencing chil- urban-rural differences in the threshold for a psychiat-
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, NOV 2001 WWW.ARCHGENPSYCHIATRY.COM
1044
©2001 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a University of St. Andrews Library User on 05/19/2015
Table 4. Distribution of the Number of Cases, the Person-years at Risk, and the Adjusted Relative Risk According
to a Categorical Model for the Accumulated Number of Years Lived in Each Degree of Urbanization During Upbringing*
Urbanicity According to the No. of Relative Risk
Accumulated Number of Years Cases Person-years (95% Confidence Interval)† P Value
Capital
⬎0 to ⬍5 y 136 314 844 1.34 (1.07-1.68)
ⱖ5 to ⬍10 y 55 113 206 1.46 (1.07-2.00)
ⱖ10 to ⬍15 y 89 102 480 2.95 (2.28-3.82)
Always (15 y) 120 233 972 2.62 (2.12-3.23)
Capital suburb
⬎0 to ⬍5 y 120 275 161 0.97 (0.77-1.21)
ⱖ5 to ⬍10 y 71 168 721 1.14 (0.86-1.51)
ⱖ10 to ⬍15 y 107 244 843 1.51 (1.18-1.94)
Always (15 y) 147 489 353 1.71 (1.40-2.08)
Provincial city
⬎0 to ⬍5 y 70 220 259 1.12 (0.87-1.44) ⬍.001
ⱖ5 to ⬍10 y 32 102 010 1.08 (0.75-1.55)
ⱖ10 to ⬍15 y 54 122 771 1.77 (1.33-2.37)
Always (15 y) 118 415 550 1.69 (1.36-2.09)
Provincial town
⬎0 to ⬍5 y 176 476 356 1.14 (0.95-1.37)
ⱖ5 to ⬍10 y 91 262 643 1.23 (0.97-1.56)
ⱖ10 to ⬍15 y 104 339 907 1.32 (1.05-1.65)
Always (15 y) 239 1 099 021 1.30 (1.09-1.54)
Rural area
Always (15 y) 224 1 493 521 1.00‡
Total 1553 5 607 060 ... ...
*Categories indicating residence less than 15 years are not mutually exclusive. For example a person who lives 7 years in the capital and 8 in the capital suburb
belong to 2 categories (capital: ⱖ5 to ⬍10 years and capital suburb ⱖ5 to ⬍10 years). Ellipses indicate data not applicable.
†Estimates of relative risk were adjusted for age and its interaction with sex, calendar year, mental illness in a parent or sibling, and change of the municipality.
‡Referent.
Table 5. Adjusted Relative Risk According to a Log-Linear Model for the Accumulated Number
of Years Lived in Each Degree of Urbanization During Upbringing
Relative Risk (95% Confidence Interval)*
Urbanicity From Birth
to the 15th Birthday Per Year Per 15 y† P Value
Capital 1.0697 (1.0572-1.0824) 2.75 (2.31-3.28)
Capital suburb 1.0355 (1.0242-1.0469) 1.69 (1.43-1.99)
Provincial city 1.0363 (1.0232-1.0496) 1.71 (1.41-2.06) ⬍.001
Provincial town 1.0187 (1.0081-1.0293) 1.32 (1.13-1.54)
Rural area 1.0000‡ 1.00‡
*Estimates of relative risk were adjusted for age and its interaction with sex, calendar year, mental illness in a parent or sibling, and change of the municipality.
†The relative risk per 15 years is calculated by raising the relative risk per year to the 15th power, eg, 1.069715 = 2.75.
‡Referent.
ric admission with schizophrenia. Furthermore, ser- will be much larger than the association with urbanicity
vices are free and distances are small in Denmark. during upbringing we demonstrated.
The results of the study are based on patients with To our knowledge, this is the first study to directly
schizophrenia admitted to a psychiatric hospital or those assess the relative importance of urbanicity at birth and
in outpatient care diagnosed as having schizophrenia. Al- during upbringing. Lewis et al4 have shown an associa-
though not all patients with schizophrenia are admitted tion between being brought up in urban areas and hav-
to a psychiatric hospital or are in outpatient care during ing schizophrenia later in life, but they did not distin-
the first episode, many will eventually be admitted or come guish this effect from an effect of urban birth. Marcelis
in for outpatient care and, thus, subsequently will be- et al25 showed that urban residence at onset did not
come registered. Furthermore, the classification of de- affect schizophrenia risk when controlling for urban
gree of urbanization is based on the number of inhabi- birth. However, their results may be biased by the mi-
tants in the largest city in the municipality, and is almost gration of preschizophrenic people before their first
certainly a crude proxy variable for the unidentified un- hospitalization with schizophrenia. Although our find-
derlying risk factors and mechanism. If the underlying ings must be replicated, they warrant direct tests of the
risk-increasing mechanisms explaining the urban-rural hypothesis that continuous, or repeated, exposures
difference can be identified, it is likely that their effects during upbringing that occur more frequently in urban-
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, NOV 2001 WWW.ARCHGENPSYCHIATRY.COM
1045
©2001 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a University of St. Andrews Library User on 05/19/2015
ized areas are responsible for the association between 9. Munk-Jørgensen P, Mortensen PB. The Danish Psychiatric Central Register. Dan
Med Bull. 1997;44:82-84.
urbanization and schizophrenia risk. Candidate risk
10. World Health Organization. Manual of the International Classification of Diseases,
factors would include infections, diet, and exposure to 8th Revision (ICD-8). Geneva, Switzerland: World Health Organization; 1967.
pollution. 11. World Health Organization. International Classification of Diseases, 10th Revi-
sion (ICD-10). Geneva, Switzerland: World Health Organization; 1992.
Accepted for publication May 1, 2001. 12. Statistics Denmark. Befolkningen i Kommunerne 1. Januar 1997. Copenhagen,
Denmark: Statistics Denmark; 1997.
This study was supported by the Theodore and Vada
13. Statistics Denmark. Statistisk Årbog 1997. Copenhagen, Denmark: Statistics Den-
Stanley Foundation, Bethesda, Md. The National Centre for mark; 1997.
Register-Based Research is funded by the Danish National 14. Breslow NE, Day NE. Statistical Methods in Cancer Research Volume II: The De-
Research Foundation, Copenhagen. sign and Analysis of Cohort Studies. Oxford, England: Oxford University Press;
Corresponding author and reprints: Carsten Bøcker 1987. IARC scientific publication 82.
15. SAS Institute Inc. The GENMOD procedure. In: SAS/STAT Software: Changes and
Pedersen, MSc, National Centre for Register-Based Re-
Enhancements Through Release 6.12. Cary, NC: SAS Institute Inc; 1997:247-348.
search, Aarhus University, Taasingegade 1, 8000 Aarhus 16. Clayton D, Hills M. Statistical Models in Epidemiology. New York, NY: Oxford
C, Denmark (e-mail: cbp@ncrr.au.dk). University Press Inc; 1993.
17. Breslow NE. Generalized linear models: checking assumptions and strengthen-
ing conclusions. Statistica Applicata. 1996;8:23-41.
REFERENCES 18. Fuller WA. Measurement Error Models. New York, NY: John Wiley & Sons Inc;
1987.
1. Gottesman II. Schizophrenia Genesis: The Origins of Madness. New York, NY: 19. Agerbo E, Torrey EF, Mortensen PB. Household crowding and schizophrenia are
WH Freeman & Co; 1991. unrelated in Denmark. Schizophr Res. 2001;47:243-246.
2. Mortensen PB, Pedersen CB, Westergaard T, Wohlfahrt J, Ewald H, Mors O, 20. Eaton WW, Mortensen PB, Frydenberg M. Obstetric factors, urbanization and psy-
Andersen PK, Melbye M. Effects of family history and place and season of birth chosis. Schizophr Res. 2000;43:117-123.
on the risk of schizophrenia. N Engl J Med. 1999;340:603-608. 21. Mortensen PB, Agerbo E, Eriksson T, Westergaard-Nielsen N. Parental educa-
3. Pedersen CB, Mortensen PB. Family history, place and season of birth as risk tion and socioeconomic variables as predictors of schizophrenia in the off-
factors for schizophrenia in Denmark: a replication and reanalysis. Br J Psychia- spring [abstract]. Schizophr Res. 2000;41(special issue):73.
try. 2001;179:46-52. 22. Westergaard T, Mortensen PB, Pedersen CB, Wohlfahrt J, Melbye M. Exposure
4. Lewis G, David A, Andreasson S, Allebeck P. Schizophrenia and city life. Lancet. to prenatal and childhood infections and the risk of schizophreina: suggestions
1992;340:137-140. from a study of sibship characteristics and influenza prevalence. Arch Gen Psy-
5. Mortensen PB. Urban-rural differences in the risk for schizophrenia. Int J Ment chiatry. 1999;56:993-998.
Health. 2000;29:101-110. 23. Jones P, Rodgers B, Murray R, Marmot M. Child development risk factors for adult
6. Freeman H. Schizophrenia and city residence. Br J Psychiatry Suppl. 1994;164 schizophrenia in the British 1946 birth cohort. Lancet. 1994;344:1398-1402.
(suppl 23):39-50. 24. Done DJ, Crow TJ, Johnstone EC, Sacker A. Childhood antecedents of schizo-
7. Marcelis M, Navarro-Mateu F, Murray R, Selten JP, Van Os J. Urbanization and phrenia and affective illness: social adjustment at ages 7 and 11. BMJ. 1994;
psychosis: a study of 1942-1978 birth cohorts in the Netherlands. Psychol Med. 309:699-703.
1998;28:871-879. 25. Marcelis M, Takei N, van Os J. Urbanization and risk for schizophrenia: does the
8. Malig C. The civil registration system in Denmark. Tech Pap Int Inst Vital Registr effect operate before or around the time of illness onset? Psychol Med. 1999;
Stat. 1996;66:1-6. 29:1197-1203.
(REPRINTED) ARCH GEN PSYCHIATRY/ VOL 58, NOV 2001 WWW.ARCHGENPSYCHIATRY.COM
1046
©2001 American Medical Association. All rights reserved.
Downloaded From: http://archpsyc.jamanetwork.com/ by a University of St. Andrews Library User on 05/19/2015
You might also like
- Olympus CLV s190 ManualDocument40 pagesOlympus CLV s190 ManualPolo RaztecaNo ratings yet
- Do You Agree or Disagree With McCarthyDocument3 pagesDo You Agree or Disagree With McCarthyBinu Kumar100% (3)
- Two Year Old Preschool Lesson Plan PDFDocument13 pagesTwo Year Old Preschool Lesson Plan PDFsally rahan100% (2)
- 1951 New York State Building CodeDocument292 pages1951 New York State Building Codekip2001No ratings yet
- Lab 2 - Report - FO1Document23 pagesLab 2 - Report - FO1V TH100% (1)
- Strategic Management ProjectDocument84 pagesStrategic Management ProjectTalha Abdul Rauf57% (7)
- Raising Power Practices OccultDocument5 pagesRaising Power Practices OccultRaúl Antonio Morales DomínguezNo ratings yet
- Effects of Family History and Place and Season of Birth On The Risk of SchizophreniaDocument6 pagesEffects of Family History and Place and Season of Birth On The Risk of SchizophreniaAnastasia FebriantiNo ratings yet
- Schizophrenia Review of Molecular GeneticsDocument18 pagesSchizophrenia Review of Molecular Geneticsmustafa566512345No ratings yet
- kww009 PDFDocument10 pageskww009 PDFsaniya ashilahNo ratings yet
- Risk Factors For Autism. Perinatal Factors Parental Psychiatric History and Socioeconomic StatusDocument10 pagesRisk Factors For Autism. Perinatal Factors Parental Psychiatric History and Socioeconomic StatusJulio CesarNo ratings yet
- MacGinty Et Al-2018-Pediatric PulmonologyDocument14 pagesMacGinty Et Al-2018-Pediatric Pulmonologywawa chenNo ratings yet
- Urban Birth and Risk of Schizophrenia: A Worrying Example of Epidemiology Where The Data Are Stronger Than The HypothesesDocument4 pagesUrban Birth and Risk of Schizophrenia: A Worrying Example of Epidemiology Where The Data Are Stronger Than The HypothesesvitaNo ratings yet
- DEPRESIADocument9 pagesDEPRESIACojocaru Cristina IoanaNo ratings yet
- 7 NatDocument6 pages7 NatLidwina ApyakaNo ratings yet
- J9 How Little We Know Herpes ZosterDocument4 pagesJ9 How Little We Know Herpes ZosterNur Adha AtjoNo ratings yet
- Trend and Outcome of Sepsis in ChildrenDocument8 pagesTrend and Outcome of Sepsis in ChildrenGunduz AgaNo ratings yet
- Epilepsi Dari Ortu PDFDocument10 pagesEpilepsi Dari Ortu PDFCONSTANTIUS AUGUSTONo ratings yet
- Ethnic Minotrity StatusDocument11 pagesEthnic Minotrity StatusFabiana H. ShimabukuroNo ratings yet
- Adverse Childhood ExperiencesDocument8 pagesAdverse Childhood ExperiencesMa. Alicia Jimenez MartinezNo ratings yet
- Eclinicalmedicine: Victoria Peer, Naama Schwartz, Manfred S. GreenDocument10 pagesEclinicalmedicine: Victoria Peer, Naama Schwartz, Manfred S. GreenBryam Arango HuamanNo ratings yet
- Prevalence and CharacteristicsDocument8 pagesPrevalence and CharacteristicsЯковлев АлександрNo ratings yet
- NEonatal Sepsis PDFDocument11 pagesNEonatal Sepsis PDFMarielaTessyGonzalesParedesNo ratings yet
- Special Article SchizophreniaDocument10 pagesSpecial Article SchizophreniaCitra KristiNo ratings yet
- Autismo EgiptoDocument8 pagesAutismo EgiptoOvsd Vfsg SDNo ratings yet
- Ni Hms 804361Document11 pagesNi Hms 804361Makhda Nurfatmala LubisNo ratings yet
- Neonatal SepsisDocument11 pagesNeonatal SepsisrezkadehaNo ratings yet
- 2010 - Epidemioloy of Ulcerative Keratitis in Northern CaliforniaDocument7 pages2010 - Epidemioloy of Ulcerative Keratitis in Northern CaliforniaPrasetya AnugrahNo ratings yet
- 2013 - Epidemiology of Stuttering - 21st Century AdvancesDocument22 pages2013 - Epidemiology of Stuttering - 21st Century AdvancesMagdalena Cuevas ArguataNo ratings yet
- Fazel 2014 CORRECTE PDFDocument11 pagesFazel 2014 CORRECTE PDFMargaNo ratings yet
- Medicine 2021: Specific Health Problems: Genetic DisordersDocument7 pagesMedicine 2021: Specific Health Problems: Genetic DisordersKita kitaNo ratings yet
- InfekcijaasdDocument8 pagesInfekcijaasdЈевремПоповићNo ratings yet
- Journal Pone 0207095Document16 pagesJournal Pone 0207095Vivi SinulinggaNo ratings yet
- Síndromes de Anomalías en Cromosomas SexualesDocument9 pagesSíndromes de Anomalías en Cromosomas SexualesIscoMoragaNo ratings yet
- Gender 22Document4 pagesGender 22andi tzamrah istiqani syamNo ratings yet
- EpidemioDocument6 pagesEpidemioFlavian Costin NacladNo ratings yet
- Pone 0206340 PDFDocument17 pagesPone 0206340 PDFSelfa YunitaNo ratings yet
- The Prevention of SchizophreniaDocument5 pagesThe Prevention of Schizophreniasaurav.das2030No ratings yet
- Noncommunicable Diseases, Risk Factors, and Protective FactorsDocument12 pagesNoncommunicable Diseases, Risk Factors, and Protective Factorsnanardim1No ratings yet
- Smoking and CHDDocument19 pagesSmoking and CHDAnonymous NeRC5JYiSNo ratings yet
- Captura de Pantalla 2024-01-23 A La(s) 11.26.43Document9 pagesCaptura de Pantalla 2024-01-23 A La(s) 11.26.43Dany MorBenNo ratings yet
- Perinatalni I Prenatalni Uzroci AutizmaDocument8 pagesPerinatalni I Prenatalni Uzroci AutizmaJohn SmithNo ratings yet
- Risk of Oral Clefts in TwinsDocument7 pagesRisk of Oral Clefts in Twinsedward iskandarNo ratings yet
- Genetic Liability To Schizophrenia Is Associated With Exposure To Traumatic Events in ChildhoodDocument8 pagesGenetic Liability To Schizophrenia Is Associated With Exposure To Traumatic Events in Childhoodsamira6alvarado6zebaNo ratings yet
- 11th R.LDocument24 pages11th R.LWilliam Tac anNo ratings yet
- Sociodemographic and Environmental FactoDocument17 pagesSociodemographic and Environmental FactoLigiaNo ratings yet
- Consangenious MarriagesDocument17 pagesConsangenious MarriagesskylertNo ratings yet
- Bahan Jurding Kulit 1Document16 pagesBahan Jurding Kulit 1Baim TmvnNo ratings yet
- Plos One 2021Document20 pagesPlos One 2021cdsaludNo ratings yet
- Esclerosis ArtDocument13 pagesEsclerosis ArtKelly GómezNo ratings yet
- The Complex Aetiology of Cerebral PalsyDocument16 pagesThe Complex Aetiology of Cerebral PalsyAileen MéndezNo ratings yet
- Ensefalitis 9Document4 pagesEnsefalitis 9Asri RachmawatiNo ratings yet
- Hollander Et Al (2016) Refugee Migration and Risk of SchizophreniaDocument8 pagesHollander Et Al (2016) Refugee Migration and Risk of SchizophreniaMaria Mendez RodriguezNo ratings yet
- Riesgos en VSRDocument11 pagesRiesgos en VSRlorena mirielisNo ratings yet
- Artigo JAMADocument7 pagesArtigo JAMAVanessa LealNo ratings yet
- Writing A Research ProposalDocument6 pagesWriting A Research ProposalLoc NguyenNo ratings yet
- Writing A Research ProposalDocument6 pagesWriting A Research ProposalLoc NguyenNo ratings yet
- Frailty Syndrome and Risk of Sepsis in The REasons ForDocument18 pagesFrailty Syndrome and Risk of Sepsis in The REasons ForIkhsan Amadea9969No ratings yet
- Variations in The Incidence of Schizophrenia: Data Versus DogmaDocument3 pagesVariations in The Incidence of Schizophrenia: Data Versus DogmaMarisca JohnNo ratings yet
- The Contribution of Social Factors To The Development of Schizophrenia: A Review of Recent FindingsDocument10 pagesThe Contribution of Social Factors To The Development of Schizophrenia: A Review of Recent FindingsJEREMY RANo ratings yet
- Himmelmann2011 PDFDocument12 pagesHimmelmann2011 PDFRaditNo ratings yet
- Antecedents of CPDocument8 pagesAntecedents of CPЯковлев АлександрNo ratings yet
- Jansen2016 PDFDocument15 pagesJansen2016 PDFRahmad SyamsulNo ratings yet
- Neurodevelopmental Assessment in Kindergarten in Children Exposed To General Anesthesia Before The Age of 4 YearsDocument11 pagesNeurodevelopmental Assessment in Kindergarten in Children Exposed To General Anesthesia Before The Age of 4 YearsJenivia LulileloNo ratings yet
- BMC Public Health: Down Syndrome, Paternal Age and Education: Comparison of California and The Czech RepublicDocument10 pagesBMC Public Health: Down Syndrome, Paternal Age and Education: Comparison of California and The Czech RepublicHalimatus Sa'diyahhNo ratings yet
- Psychiatry of Pandemics: A Mental Health Response to Infection OutbreakFrom EverandPsychiatry of Pandemics: A Mental Health Response to Infection OutbreakDamir HuremovićNo ratings yet
- The Maternal Imprint: The Contested Science of Maternal-Fetal EffectsFrom EverandThe Maternal Imprint: The Contested Science of Maternal-Fetal EffectsNo ratings yet
- JSA SC Area KariangauDocument20 pagesJSA SC Area KariangauSiti AminahNo ratings yet
- The Spirit Controlled Life Ebook PDF 1Document184 pagesThe Spirit Controlled Life Ebook PDF 1Okesola AbayomiNo ratings yet
- Axialflow SeriesDocument40 pagesAxialflow SerieswachemilNo ratings yet
- About PolyethyleneDocument4 pagesAbout PolyethyleneMifzal IzzaniNo ratings yet
- Valency and Formulae-HandoutDocument3 pagesValency and Formulae-HandoutABHAVYA RAJNo ratings yet
- Finger Sprain: Active Finger Flexion ExercisesDocument7 pagesFinger Sprain: Active Finger Flexion ExercisesTJPlayzNo ratings yet
- VFD-E - Manual Vfd022e43aDocument395 pagesVFD-E - Manual Vfd022e43aJuan LopezNo ratings yet
- Blackrock PeriodicDocument2 pagesBlackrock Periodicsameer1987kazi4405No ratings yet
- Filipendula Ulmaria BrochureDocument3 pagesFilipendula Ulmaria BrochureMamta maheshwariNo ratings yet
- Earth and Life Science11 - Q1 - Module 2Document18 pagesEarth and Life Science11 - Q1 - Module 2Gab PlayzNo ratings yet
- RPD Daily Incident Report 1/5/23Document5 pagesRPD Daily Incident Report 1/5/23inforumdocsNo ratings yet
- Commissioning Tests For HV Underground Cables (Up To 33Kv) SWPDocument13 pagesCommissioning Tests For HV Underground Cables (Up To 33Kv) SWPCharles Robiansyah100% (1)
- Bullying Survey StudentDocument3 pagesBullying Survey Studentrizalina bronosoNo ratings yet
- CoilDocument8 pagesCoilJosé Luis Martinez GodoyNo ratings yet
- Journal Multivariate Mita2016Document36 pagesJournal Multivariate Mita2016Mange Sumange GffrNo ratings yet
- Impalutao Integrated School: Briging Program Report Grade 9 CurriculumDocument3 pagesImpalutao Integrated School: Briging Program Report Grade 9 CurriculumIVy PearlNo ratings yet
- Filling The Gaps: COMMUTE and The Fight For Transit Equity in New York CityDocument20 pagesFilling The Gaps: COMMUTE and The Fight For Transit Equity in New York CityApplied Research CenterNo ratings yet
- Establish A LawnDocument4 pagesEstablish A LawnStain MasterGNo ratings yet
- Neurotransmitters in Schizophrenia: Dr. Adel El SheshaiDocument47 pagesNeurotransmitters in Schizophrenia: Dr. Adel El SheshaielvinegunawanNo ratings yet
- Consumer Perception About Herbal and Non Herbal Products"Document48 pagesConsumer Perception About Herbal and Non Herbal Products"Diksha Prajapati100% (1)
- Approach To Coagulation DisordersDocument20 pagesApproach To Coagulation DisordersTri P BukerNo ratings yet
- Roderico R. Bioco: BGB ChairmanDocument28 pagesRoderico R. Bioco: BGB ChairmanjeorgiaNo ratings yet
- Year 9 Biology InvestigationDocument2 pagesYear 9 Biology Investigationapi-222503660No ratings yet