Download as pdf or txt
You might also like
- ICA International Diploma in Financial Crime Assignment 1Document20 pagesICA International Diploma in Financial Crime Assignment 1devonna100% (2)
- Cost AccountingDocument71 pagesCost AccountingEnis ErenözlüNo ratings yet
- Planning and Budgeting - PPT NotesDocument44 pagesPlanning and Budgeting - PPT NotesEmma WongNo ratings yet
- ICAB Lecture 1 & 2 On Chapter 1 Fundamentals of Costing - RCKDocument10 pagesICAB Lecture 1 & 2 On Chapter 1 Fundamentals of Costing - RCKrajeshaisdu009No ratings yet
- Then Do A Pictionary of The Jobs That You Can See in The PuzzleDocument7 pagesThen Do A Pictionary of The Jobs That You Can See in The PuzzleDayana VegaNo ratings yet
- Chapter 6 - AGGREGATE PLANNINGDocument9 pagesChapter 6 - AGGREGATE PLANNINGLong Đoàn PhiNo ratings yet
- Module 1 and 2 - Introduction To Management Accounting and Cost Classification and Behavior (Addtl) PDFDocument10 pagesModule 1 and 2 - Introduction To Management Accounting and Cost Classification and Behavior (Addtl) PDFAlliah ArrozaNo ratings yet
- Budgeting PDFDocument22 pagesBudgeting PDFBufan Ioana-Diana100% (1)
- Chapter 6 - AGGREGATE PLANNINGDocument9 pagesChapter 6 - AGGREGATE PLANNINGson15072003No ratings yet
- Topic 3: Operational Budgeting and Inventory ManagementDocument29 pagesTopic 3: Operational Budgeting and Inventory Managementsv03No ratings yet
- E Tivity2 Bsa 2d PastorjanmichaelsDocument7 pagesE Tivity2 Bsa 2d PastorjanmichaelsJan Michael PastorNo ratings yet
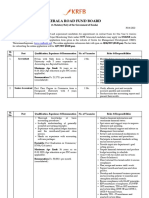
- Kerala Road Fund Board: (A Statutory Body of The Government of Kerala)Document5 pagesKerala Road Fund Board: (A Statutory Body of The Government of Kerala)vishnuprasad4292No ratings yet
- Accounting Short 2 PageDocument2 pagesAccounting Short 2 Pagemdanss1244No ratings yet
- Beyond The Balanced Scorecard WebDocument7 pagesBeyond The Balanced Scorecard Webthomas_pachecoNo ratings yet
- HSS MandE Framework Nov 2009 PDFDocument28 pagesHSS MandE Framework Nov 2009 PDFBahjaNo ratings yet
- Unit 5: Management AccountingDocument22 pagesUnit 5: Management AccountingArif KhanNo ratings yet
- Proposal Penelitian AspDocument11 pagesProposal Penelitian AspAndhiend Nagh TzanelNo ratings yet
- Background Reading Material: Elementary Basics ofDocument22 pagesBackground Reading Material: Elementary Basics ofSaloni MalhotraNo ratings yet
- 111 947 Epr Bso Call Annex C Logframe 220519Document3 pages111 947 Epr Bso Call Annex C Logframe 220519clairemilhietNo ratings yet
- Management Accounting - SBA1501: Unit - IDocument9 pagesManagement Accounting - SBA1501: Unit - ISubhasri RajaNo ratings yet
- BIB3204 IBM3203 Week12Document6 pagesBIB3204 IBM3203 Week12HITANSH KHANDELWALNo ratings yet
- Gateway Managerial Accounting MasterDocument48 pagesGateway Managerial Accounting Masterkhalid iqbalNo ratings yet
- Chapter 2. Business Motivations and Drivers For Big Data AdoptionDocument45 pagesChapter 2. Business Motivations and Drivers For Big Data AdoptionThư PhạmNo ratings yet
- BPM - 3 - HalaDocument12 pagesBPM - 3 - HalaAsadulla KhanNo ratings yet
- Good Governance, Performance Based Budgeting and SKPD Budget QualityDocument39 pagesGood Governance, Performance Based Budgeting and SKPD Budget QualityAnggreni Christine Carly SinagaNo ratings yet
- Service Delivery Model TemplateDocument3 pagesService Delivery Model Templatekholofelo letsoaloNo ratings yet
- Microsoft Dynamics AX Lean AccountingDocument26 pagesMicrosoft Dynamics AX Lean AccountingYaowalak Sriburadej100% (2)
- 2.0 Literature Review: 2.1 The Role of A Management AccountantDocument7 pages2.0 Literature Review: 2.1 The Role of A Management AccountantTeneswari RadhaNo ratings yet
- Integrated Report FinalDocument32 pagesIntegrated Report FinalVenkatesh VenkateshNo ratings yet
- Management Accounting NotesDocument80 pagesManagement Accounting Notesnuk.2021018028No ratings yet
- Projected Financial Statements Page 1Document16 pagesProjected Financial Statements Page 1ScribdTranslationsNo ratings yet
- Akbar MADocument21 pagesAkbar MAShah MuradNo ratings yet
- University of London (LSE)Document33 pagesUniversity of London (LSE)Dương DươngNo ratings yet
- Budgeting HandbookDocument1 pageBudgeting HandbookTamer ŞenerNo ratings yet
- Controlling Is A Primary Goal-Oriented Function of Management in AnDocument8 pagesControlling Is A Primary Goal-Oriented Function of Management in AnBrian Rey L. AbingNo ratings yet
- Comparative Chart HWDocument3 pagesComparative Chart HWXIMENA MORALES RIVERANo ratings yet
- Chapter 1 Introduction For 2009Document16 pagesChapter 1 Introduction For 2009filimonkinfe47No ratings yet
- TaskDocument5 pagesTaskwovefiv466No ratings yet
- Strategic Planning of Socio-Economic Development of Service EnterprisesDocument4 pagesStrategic Planning of Socio-Economic Development of Service EnterprisesCentral Asian StudiesNo ratings yet
- MBO AllDocument104 pagesMBO AllradhiaalfonceNo ratings yet
- CapstoneDocument16 pagesCapstoneKristine Kaye MercadoNo ratings yet
- Budget and Budgetary Control: A Study OnDocument10 pagesBudget and Budgetary Control: A Study Onferoz khanNo ratings yet
- Management Accounting (Unit 01)Document12 pagesManagement Accounting (Unit 01)md tabishNo ratings yet
- Advanced Management Accounting: Dr. Ronny Andesto, S.E., M.M Program Magister Akuntansi Universitas Mercu Buana 2018Document30 pagesAdvanced Management Accounting: Dr. Ronny Andesto, S.E., M.M Program Magister Akuntansi Universitas Mercu Buana 2018dhianNo ratings yet
- The Role of Budgeting in The Management Process: Planning and ControlDocument22 pagesThe Role of Budgeting in The Management Process: Planning and ControlBufan Ioana-Diana33% (3)
- Balanced ScoreCardDocument36 pagesBalanced ScoreCardProf. Lakshman Madurasinghe100% (17)
- Profit Planning (Budgeting) - Development of An Operational Plan To Achieve A Company's Goals and ObjectivesDocument2 pagesProfit Planning (Budgeting) - Development of An Operational Plan To Achieve A Company's Goals and ObjectivesSherilyn QuidolesNo ratings yet
- MM MM: By, Sant K. GuptaDocument23 pagesMM MM: By, Sant K. GuptasantNo ratings yet
- Effect of Financial Performance On Earnings Management in The Drug Distribution IndustryDocument4 pagesEffect of Financial Performance On Earnings Management in The Drug Distribution IndustrySalma ChakrounNo ratings yet
- Accounts: Critically Evaluate The Evolution in The Role of Management Accounting in Assisting Decision Makers in OrganisationsDocument7 pagesAccounts: Critically Evaluate The Evolution in The Role of Management Accounting in Assisting Decision Makers in OrganisationsPrabina PoudelNo ratings yet
- Business Process Document - Cost Centre AccountingDocument24 pagesBusiness Process Document - Cost Centre AccountingfharooksNo ratings yet
- Em 1 2017 08 PDFDocument18 pagesEm 1 2017 08 PDFDaria RotaruNo ratings yet
- Planning For Operating ExcellenceDocument11 pagesPlanning For Operating ExcellenceAlonso ValerianoNo ratings yet
- AFM Class NotesDocument33 pagesAFM Class NotesSamil MusthafaNo ratings yet
- The Balanced Scorecard (BSC) For Danish FarmDocument17 pagesThe Balanced Scorecard (BSC) For Danish FarmPrajanNo ratings yet
- Ch.2-Evaluating Operational PerformanceDocument21 pagesCh.2-Evaluating Operational PerformanceTiwi PangestiNo ratings yet
- AIS Lecture 9 Notes S1 2016 (V1) - CH 13 On GL Fin Report Cycle-StudentDocument20 pagesAIS Lecture 9 Notes S1 2016 (V1) - CH 13 On GL Fin Report Cycle-StudentfernandarvNo ratings yet
- Performance Measurement: Linking Balanced Scorecard to Business IntelligenceFrom EverandPerformance Measurement: Linking Balanced Scorecard to Business IntelligenceNo ratings yet
- Implementing Results-Based Budget Management Frameworks: An Assessment of Progress in Selected CountriesFrom EverandImplementing Results-Based Budget Management Frameworks: An Assessment of Progress in Selected CountriesNo ratings yet
- Extending Care Beyond Hospital Walls: Follow-Up Program Impacts Patients and Addresses Post-Discharge NeedsDocument3 pagesExtending Care Beyond Hospital Walls: Follow-Up Program Impacts Patients and Addresses Post-Discharge Needsacma2010No ratings yet
- Developing A Palliative Care Service: One Hospital's ExperienceDocument2 pagesDeveloping A Palliative Care Service: One Hospital's Experienceacma2010No ratings yet
- 2010 V 8 I 3 A 3Document3 pages2010 V 8 I 3 A 3acma2010No ratings yet
- The Critical Role of Clinical Social Work in Case ManagementDocument2 pagesThe Critical Role of Clinical Social Work in Case Managementacma2010No ratings yet
- A Management Engineering Approach To Improving Throughput and Shortening Overall LOS: An Unique Model For Efficiency and Time StudyDocument2 pagesA Management Engineering Approach To Improving Throughput and Shortening Overall LOS: An Unique Model For Efficiency and Time Studyacma2010No ratings yet
- Opening The Door To Timely and Informative DischargeDocument3 pagesOpening The Door To Timely and Informative Dischargeacma2010No ratings yet
- Getting The Most From Consultant Resources: by Martha J. Koen, ACM, MN, RNDocument2 pagesGetting The Most From Consultant Resources: by Martha J. Koen, ACM, MN, RNacma2010No ratings yet
- A Medical Director's PerspectiveDocument4 pagesA Medical Director's Perspectiveacma2010No ratings yet
- My Magnificent Seven' - How Case Management Assistants Turbo-Charge The Case Management FunctionDocument2 pagesMy Magnificent Seven' - How Case Management Assistants Turbo-Charge The Case Management Functionacma2010No ratings yet
- Case Manager Certification Offers Unique Practice-Specific ValidationDocument2 pagesCase Manager Certification Offers Unique Practice-Specific Validationacma2010No ratings yet
- Discharge Screening: Emergency Department Case Managers Help Improve Compliance With Discharge InstructionsDocument2 pagesDischarge Screening: Emergency Department Case Managers Help Improve Compliance With Discharge Instructionsacma2010No ratings yet
- Issues in Pediatric Case Management: by Rhonda Cofield, MSW, LCSWDocument2 pagesIssues in Pediatric Case Management: by Rhonda Cofield, MSW, LCSWacma2010No ratings yet
- Discharge Screening: Emergency Department Case Managers Help Improve Compliance With Discharge InstructionsDocument3 pagesDischarge Screening: Emergency Department Case Managers Help Improve Compliance With Discharge Instructionsacma2010No ratings yet
- Oncology Case Management Across The Continuum of Care: by Amelia Williams, MSWDocument2 pagesOncology Case Management Across The Continuum of Care: by Amelia Williams, MSWacma2010No ratings yet
- A View From The Field: Career Advancement Through Clinical LaddersDocument2 pagesA View From The Field: Career Advancement Through Clinical Laddersacma2010No ratings yet
- Supervision in Case Management: A Focus On Professional DevelopmentDocument3 pagesSupervision in Case Management: A Focus On Professional Developmentacma2010No ratings yet
- Emergency Department Gatekeepers - Interventions With Chronic Pain Patients and Identity FraudDocument3 pagesEmergency Department Gatekeepers - Interventions With Chronic Pain Patients and Identity Fraudacma2010No ratings yet
- A Medical Director's PerspectiveDocument2 pagesA Medical Director's Perspectiveacma2010No ratings yet
- "Life Changes in The Instant. The Ordinary Instant ": Dying Well: Case Management Leads A Process Redesign ProjectDocument3 pages"Life Changes in The Instant. The Ordinary Instant ": Dying Well: Case Management Leads A Process Redesign Projectacma2010No ratings yet
- A Medical Director's PerspectiveDocument2 pagesA Medical Director's Perspectiveacma2010No ratings yet
- A View From The Field: Emergency Department Case Managers Support Innovation That Improves Hospital RevenueDocument2 pagesA View From The Field: Emergency Department Case Managers Support Innovation That Improves Hospital Revenueacma2010No ratings yet
- British American Tobacco (BAT)Document24 pagesBritish American Tobacco (BAT)acidreign100% (2)
- ﺩﻭﺭ ﺍﻵﻟﻴﺎﺕ ﺍﻟﺩﺍﺨﻠﻴﺔ ﻟﻠﺤﻭﻜﻤﺔ ﻓﻲ ﺘﺤﺴﻴﻥ ﺍﻻﻓﺼﺎﺡ ﻭﺍﻟﺘﻘﺭﻴﺭ ﻋﻥ ﺍﻟﻤﺴﺅﻭﻟﻴﺔ ﺍﻻﺠﺘﻤﺎﻋﻴﺔ ﻟﻤﻨﺸﺂﺕ ﺍﻻﻋﻤﺎل ﺍﻟﺴﻌﻭﺩﻴﻪ PDFDocument49 pagesﺩﻭﺭ ﺍﻵﻟﻴﺎﺕ ﺍﻟﺩﺍﺨﻠﻴﺔ ﻟﻠﺤﻭﻜﻤﺔ ﻓﻲ ﺘﺤﺴﻴﻥ ﺍﻻﻓﺼﺎﺡ ﻭﺍﻟﺘﻘﺭﻴﺭ ﻋﻥ ﺍﻟﻤﺴﺅﻭﻟﻴﺔ ﺍﻻﺠﺘﻤﺎﻋﻴﺔ ﻟﻤﻨﺸﺂﺕ ﺍﻻﻋﻤﺎل ﺍﻟﺴﻌﻭﺩﻴﻪ PDFTareq Yousef Abualajeen100% (1)
- 6 Question: Suggest How Should RSWMDocument3 pages6 Question: Suggest How Should RSWMai_geethuNo ratings yet
- 15 BM Taxlawsconstrued 11 22 07 CPCDocument59 pages15 BM Taxlawsconstrued 11 22 07 CPCMerlina Cuare50% (2)
- CISADocument31 pagesCISAmadunixNo ratings yet
- Corrective and Preventative Action Systems: Standard Operating ProceduresDocument6 pagesCorrective and Preventative Action Systems: Standard Operating ProceduresNTAMBO KABEKENo ratings yet
- Workforce-Related Risks in Projects With A Contingent WorkforceDocument12 pagesWorkforce-Related Risks in Projects With A Contingent Workforceghassan riazNo ratings yet
- Piie QcpuDocument71 pagesPiie QcpuEunice Joy Romero BeranaNo ratings yet
- Memo - Development Review Pilot Program - ENDocument2 pagesMemo - Development Review Pilot Program - ENmpearson78No ratings yet
- Solving Retail Problems Using Lean Six SigmaDocument12 pagesSolving Retail Problems Using Lean Six SigmaYash VermaNo ratings yet
- Data Warehouse Project Management: Listen, Listen, Listen To The StakeholdersDocument9 pagesData Warehouse Project Management: Listen, Listen, Listen To The StakeholdersjanivarunNo ratings yet
- Job Description For Assistant Manager - HR OpsDocument2 pagesJob Description For Assistant Manager - HR OpsKompally Prachetan SharmaNo ratings yet
- Understanding Dimensions of Business ViabilityDocument9 pagesUnderstanding Dimensions of Business Viabilityfms162No ratings yet
- Stadium and Club Tours - Senior Tour GuideDocument4 pagesStadium and Club Tours - Senior Tour GuidebizmbuuNo ratings yet
- Lecture 4Document29 pagesLecture 4Chinong HowNo ratings yet
- A Comparative Analysis of Strategies and Business Models of Starbucks Corporation and Dunkin Donuts CompanyDocument10 pagesA Comparative Analysis of Strategies and Business Models of Starbucks Corporation and Dunkin Donuts CompanyBạch HàNo ratings yet
- Sap Fi Gen FinanceDocument7 pagesSap Fi Gen FinanceRavi Chandra LNo ratings yet
- Product Life Cycle Impact On Logistics and Distribution StrategyDocument7 pagesProduct Life Cycle Impact On Logistics and Distribution StrategyRiste Kelepurovski100% (2)
- HR Analytics UNIT 1Document7 pagesHR Analytics UNIT 1Tommy YadavNo ratings yet
- Shariah Governance Framework For Islamic Insurance or TakafulDocument19 pagesShariah Governance Framework For Islamic Insurance or TakafulRayhanNo ratings yet
- Risk-Isaca PDFDocument7 pagesRisk-Isaca PDFashwin2005No ratings yet
- Exercise B2C AnswerDocument5 pagesExercise B2C AnswerNabilah Musri98No ratings yet
- Ways To Increase Construction ProductivityDocument2 pagesWays To Increase Construction ProductivityLachu LaxNo ratings yet
- Cloud Migration Assessment Framework PDFDocument12 pagesCloud Migration Assessment Framework PDFtim.howell8050100% (1)
- Research Methodology: Chapter-1Document30 pagesResearch Methodology: Chapter-1Sulav SmsNo ratings yet
- Cobit INFOSECDocument36 pagesCobit INFOSECDavid LezcanoNo ratings yet
- PMLCDocument5 pagesPMLCiyappanaNo ratings yet
- English / Spanish Version Versión en Inglés y EspañolDocument21 pagesEnglish / Spanish Version Versión en Inglés y EspañolCristian David Cifuentes ParadaNo ratings yet
- Final Question Paper - Question Bank - Production and Operations Management - MBA 025Document5 pagesFinal Question Paper - Question Bank - Production and Operations Management - MBA 025Dr Rushen Singh80% (5)