
Direct Pulp Capping With Calcium Hydroxide, Mineral Trioxide Aggregate, and Biodentine in Permanent Young Teeth With Caries - A Randomized Clinical Trial
Direct Pulp Capping With Calcium Hydroxide, Mineral Trioxide Aggregate, and Biodentine in Permanent Young Teeth With Caries - A Randomized Clinical Trial
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
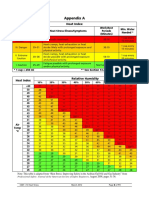
- Heat Index ChartDocument1 pageHeat Index ChartAnvarsha Sharafudheen100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Stamp Screening FormDocument3 pagesStamp Screening FormStefanie HonkkNo ratings yet
- 4d.effects of Two Fast-Setting Pulp-Capping Materials On Cell Viability andDocument6 pages4d.effects of Two Fast-Setting Pulp-Capping Materials On Cell Viability andAnisha AnilNo ratings yet
- 3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFDocument10 pages3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFAnisha AnilNo ratings yet
- Effect of Exposure Time and Pre-Heating On The Conversion Degree of Conventional, Bulk-Fill, Fiber Reinforced and Polyacid-Modified Resin CompositesDocument12 pagesEffect of Exposure Time and Pre-Heating On The Conversion Degree of Conventional, Bulk-Fill, Fiber Reinforced and Polyacid-Modified Resin CompositesAnisha AnilNo ratings yet
- CMPDocument122 pagesCMPAnisha Anil100% (1)
- Laser in OperativeDocument99 pagesLaser in OperativeAnisha AnilNo ratings yet
- Molecular Diagnostic AidsDocument90 pagesMolecular Diagnostic AidsAnisha Anil100% (1)
- Lecture Guide 2 in Engineering Data Analysis Engr. Theresa Lean Roma Tuliao-SumerDocument17 pagesLecture Guide 2 in Engineering Data Analysis Engr. Theresa Lean Roma Tuliao-SumerJustin Paul TumaliuanNo ratings yet
- SexualityDocument16 pagesSexualityGracia PattinasaranyNo ratings yet
- Earthquake Research ReportDocument4 pagesEarthquake Research ReportYaseen IsmailNo ratings yet
- Cardio Pulmonary Resuscitation and End of Life CareDocument21 pagesCardio Pulmonary Resuscitation and End of Life CareSundaraBharathi100% (1)
- Session 2 - Sufficient Causes ModelDocument51 pagesSession 2 - Sufficient Causes Modelfrank kipkoechNo ratings yet
- 1594862834TOCDocument2 pages1594862834TOCANS_MHDNo ratings yet
- Impact of Drug Abuse and Its Trafficking Its Trafficking in Society: An AppraisalDocument17 pagesImpact of Drug Abuse and Its Trafficking Its Trafficking in Society: An AppraisalTahaNo ratings yet
- Stress BustingDocument24 pagesStress BustingMarianne ChristieNo ratings yet
- Casediscussion Ludwig's Angina Review PDFDocument5 pagesCasediscussion Ludwig's Angina Review PDFBima BaskaraNo ratings yet
- Kalpa CleanseDocument21 pagesKalpa CleanseCristina Cobzaru100% (1)
- Minutes of The India-Bhutan Onsite Bilateral Meeting Guwahati, AssamDocument40 pagesMinutes of The India-Bhutan Onsite Bilateral Meeting Guwahati, AssamsidhuzNo ratings yet
- Awareness and Behavioural Outlook Towards Online PharmacyDocument6 pagesAwareness and Behavioural Outlook Towards Online PharmacyPRATIK VISHWAS SAWANT MBA 2019-21 (Delhi)No ratings yet
- Jaha 120 017275Document150 pagesJaha 120 017275Leonardo LiswojoNo ratings yet
- MAT Solved Paper 2012Document25 pagesMAT Solved Paper 2012solaris knightNo ratings yet
- Oncology Nursing Diploma Final Exam Blueprint 2022 - Final Approved 24 April 2022 PDFDocument4 pagesOncology Nursing Diploma Final Exam Blueprint 2022 - Final Approved 24 April 2022 PDFMarwa AlsataryNo ratings yet
- Moisture Guard Green Spray - GBDocument13 pagesMoisture Guard Green Spray - GBdiego albertonNo ratings yet
- Pedia Case PresDocument44 pagesPedia Case PresJharaNo ratings yet
- Instrument ProcessingDocument47 pagesInstrument ProcessingMarwa Temirek100% (1)
- Foot Reflexology: We Recommend That You Allocate at Least 30 Minutes To This WorksheetDocument5 pagesFoot Reflexology: We Recommend That You Allocate at Least 30 Minutes To This WorksheetAstro TriinityNo ratings yet
- Osha 300 FormsDocument2 pagesOsha 300 FormsLiliana PatiñoNo ratings yet
- Ambient Air Pollution Book PDFDocument232 pagesAmbient Air Pollution Book PDFmurli shahNo ratings yet
- Training PrinciplesDocument11 pagesTraining Principlesapi-249980013No ratings yet
- Section 3 - IMS Objectives and Functions - Incident Management System (IMS) Guidance - Version 2.0 - Ontario - Ca PDFDocument6 pagesSection 3 - IMS Objectives and Functions - Incident Management System (IMS) Guidance - Version 2.0 - Ontario - Ca PDFMagenta TrainingNo ratings yet
- Pharmacology SlidesDocument114 pagesPharmacology Slidesbrandon15000100% (9)
- S.S or AffidavitDocument9 pagesS.S or AffidavitAngelieNo ratings yet
- Four Major Gaps That Are Preventing Most Companies Worldwide From Achieving Excellent Process Safety PerformanceDocument25 pagesFour Major Gaps That Are Preventing Most Companies Worldwide From Achieving Excellent Process Safety PerformanceAsdika YdstrNo ratings yet
- HookwormDocument30 pagesHookwormGhea IrawanNo ratings yet
- Acyclovir Drug StudyDocument3 pagesAcyclovir Drug StudyJessie Cauilan Cain100% (1)











































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Heat Index ChartDocument1 pageHeat Index ChartAnvarsha Sharafudheen100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Stamp Screening FormDocument3 pagesStamp Screening FormStefanie HonkkNo ratings yet
- 4d.effects of Two Fast-Setting Pulp-Capping Materials On Cell Viability andDocument6 pages4d.effects of Two Fast-Setting Pulp-Capping Materials On Cell Viability andAnisha AnilNo ratings yet
- 3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFDocument10 pages3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFAnisha AnilNo ratings yet
- Effect of Exposure Time and Pre-Heating On The Conversion Degree of Conventional, Bulk-Fill, Fiber Reinforced and Polyacid-Modified Resin CompositesDocument12 pagesEffect of Exposure Time and Pre-Heating On The Conversion Degree of Conventional, Bulk-Fill, Fiber Reinforced and Polyacid-Modified Resin CompositesAnisha AnilNo ratings yet
- CMPDocument122 pagesCMPAnisha Anil100% (1)
- Laser in OperativeDocument99 pagesLaser in OperativeAnisha AnilNo ratings yet
- Molecular Diagnostic AidsDocument90 pagesMolecular Diagnostic AidsAnisha Anil100% (1)
- Lecture Guide 2 in Engineering Data Analysis Engr. Theresa Lean Roma Tuliao-SumerDocument17 pagesLecture Guide 2 in Engineering Data Analysis Engr. Theresa Lean Roma Tuliao-SumerJustin Paul TumaliuanNo ratings yet
- SexualityDocument16 pagesSexualityGracia PattinasaranyNo ratings yet
- Earthquake Research ReportDocument4 pagesEarthquake Research ReportYaseen IsmailNo ratings yet
- Cardio Pulmonary Resuscitation and End of Life CareDocument21 pagesCardio Pulmonary Resuscitation and End of Life CareSundaraBharathi100% (1)
- Session 2 - Sufficient Causes ModelDocument51 pagesSession 2 - Sufficient Causes Modelfrank kipkoechNo ratings yet
- 1594862834TOCDocument2 pages1594862834TOCANS_MHDNo ratings yet
- Impact of Drug Abuse and Its Trafficking Its Trafficking in Society: An AppraisalDocument17 pagesImpact of Drug Abuse and Its Trafficking Its Trafficking in Society: An AppraisalTahaNo ratings yet
- Stress BustingDocument24 pagesStress BustingMarianne ChristieNo ratings yet
- Casediscussion Ludwig's Angina Review PDFDocument5 pagesCasediscussion Ludwig's Angina Review PDFBima BaskaraNo ratings yet
- Kalpa CleanseDocument21 pagesKalpa CleanseCristina Cobzaru100% (1)
- Minutes of The India-Bhutan Onsite Bilateral Meeting Guwahati, AssamDocument40 pagesMinutes of The India-Bhutan Onsite Bilateral Meeting Guwahati, AssamsidhuzNo ratings yet
- Awareness and Behavioural Outlook Towards Online PharmacyDocument6 pagesAwareness and Behavioural Outlook Towards Online PharmacyPRATIK VISHWAS SAWANT MBA 2019-21 (Delhi)No ratings yet
- Jaha 120 017275Document150 pagesJaha 120 017275Leonardo LiswojoNo ratings yet
- MAT Solved Paper 2012Document25 pagesMAT Solved Paper 2012solaris knightNo ratings yet
- Oncology Nursing Diploma Final Exam Blueprint 2022 - Final Approved 24 April 2022 PDFDocument4 pagesOncology Nursing Diploma Final Exam Blueprint 2022 - Final Approved 24 April 2022 PDFMarwa AlsataryNo ratings yet
- Moisture Guard Green Spray - GBDocument13 pagesMoisture Guard Green Spray - GBdiego albertonNo ratings yet
- Pedia Case PresDocument44 pagesPedia Case PresJharaNo ratings yet
- Instrument ProcessingDocument47 pagesInstrument ProcessingMarwa Temirek100% (1)
- Foot Reflexology: We Recommend That You Allocate at Least 30 Minutes To This WorksheetDocument5 pagesFoot Reflexology: We Recommend That You Allocate at Least 30 Minutes To This WorksheetAstro TriinityNo ratings yet
- Osha 300 FormsDocument2 pagesOsha 300 FormsLiliana PatiñoNo ratings yet
- Ambient Air Pollution Book PDFDocument232 pagesAmbient Air Pollution Book PDFmurli shahNo ratings yet
- Training PrinciplesDocument11 pagesTraining Principlesapi-249980013No ratings yet
- Section 3 - IMS Objectives and Functions - Incident Management System (IMS) Guidance - Version 2.0 - Ontario - Ca PDFDocument6 pagesSection 3 - IMS Objectives and Functions - Incident Management System (IMS) Guidance - Version 2.0 - Ontario - Ca PDFMagenta TrainingNo ratings yet
- Pharmacology SlidesDocument114 pagesPharmacology Slidesbrandon15000100% (9)
- S.S or AffidavitDocument9 pagesS.S or AffidavitAngelieNo ratings yet
- Four Major Gaps That Are Preventing Most Companies Worldwide From Achieving Excellent Process Safety PerformanceDocument25 pagesFour Major Gaps That Are Preventing Most Companies Worldwide From Achieving Excellent Process Safety PerformanceAsdika YdstrNo ratings yet
- HookwormDocument30 pagesHookwormGhea IrawanNo ratings yet
- Acyclovir Drug StudyDocument3 pagesAcyclovir Drug StudyJessie Cauilan Cain100% (1)