Download as docx, pdf, or txt
You might also like
- Expense Claim Form NEW - 2 PagDocument2 pagesExpense Claim Form NEW - 2 PagGabriel Vasile MarinescuNo ratings yet
- PROPOSAL SHIP MANAGEMENT - OdtDocument7 pagesPROPOSAL SHIP MANAGEMENT - Odtloyal setiaNo ratings yet
- Logistics Company ProfileDocument12 pagesLogistics Company ProfilemydeanzNo ratings yet
- Step Vendor Register Johor PortDocument1 pageStep Vendor Register Johor Portاحمد اليفف اكملNo ratings yet
- APPIA - FIX EngineDocument2 pagesAPPIA - FIX EngineNYSE TechnologiesNo ratings yet
- WAHL - Paper Comparing Series MV Device Driver TopologiesDocument13 pagesWAHL - Paper Comparing Series MV Device Driver TopologiesRicky SwinedickNo ratings yet
- Contoh Form Claim Expenses, Form LeaveDocument5 pagesContoh Form Claim Expenses, Form LeaveRenovhie TasariNo ratings yet
- Daily Allowance Claim Form: Only For Use of EngineersDocument10 pagesDaily Allowance Claim Form: Only For Use of EngineersAltafNo ratings yet
- New Outstation Travel Claim Form (Single Page)Document1 pageNew Outstation Travel Claim Form (Single Page)Pradeep JhaNo ratings yet
- Travel Order FormDocument1 pageTravel Order FormJack SprwNo ratings yet
- Expenses Claim Form: QF/FIN/005/01/00Document2 pagesExpenses Claim Form: QF/FIN/005/01/00rahmanNo ratings yet
- Claim Form For Interview, Travel & Subsistence Expenses For 2013 Specialty Recruitment ProcessDocument2 pagesClaim Form For Interview, Travel & Subsistence Expenses For 2013 Specialty Recruitment ProcessblebeacristinaNo ratings yet
- RFQ Quotation LetterDocument1 pageRFQ Quotation LetterMd. Alomgir HossainNo ratings yet
- Veritas Logistics Company ProfileDocument15 pagesVeritas Logistics Company ProfilePhillip Plat TsanguNo ratings yet
- HR - Forms & ProceduresDocument26 pagesHR - Forms & ProceduresAsk EVANo ratings yet
- Letter of Intent Sample FormatsDocument7 pagesLetter of Intent Sample FormatsMariangel EmbusNo ratings yet
- Expense Report: From: To: Purpose: Statement #: Name: Employee ID: Department: ManagerDocument4 pagesExpense Report: From: To: Purpose: Statement #: Name: Employee ID: Department: Managerprajapatiprashant40No ratings yet
- 2Document30 pages2ASM LikhonNo ratings yet
- Expenses Claim Form (Car)Document1 pageExpenses Claim Form (Car)AsriSaffuanNo ratings yet
- Updated - Salary Sheet With Auto Salary Tax Calculator For FY 2075-2076 (Nepali Talim)Document13 pagesUpdated - Salary Sheet With Auto Salary Tax Calculator For FY 2075-2076 (Nepali Talim)samNo ratings yet
- Company Property ReceiptDocument1 pageCompany Property ReceiptRanjith KumarNo ratings yet
- Accounts Clerk Position JD Kpi KraDocument3 pagesAccounts Clerk Position JD Kpi KraCA AMIT JAINNo ratings yet
- MISA - Service Manual (10 Edition) en V1 - UpDocument149 pagesMISA - Service Manual (10 Edition) en V1 - UpquickpassNo ratings yet
- Using A Retention BondDocument2 pagesUsing A Retention Bondvivekjn100% (1)
- Vendor Registration Form PDFDocument2 pagesVendor Registration Form PDFHINANo ratings yet
- Grantt Chart Template 08Document12 pagesGrantt Chart Template 08wahyuNo ratings yet
- Hindustan Construction CompanyDocument18 pagesHindustan Construction CompanySudipta BoseNo ratings yet
- Bank Guarantee-I (Bg-I) / Counter Guarantee-I (Cg-I) ApplicationDocument2 pagesBank Guarantee-I (Bg-I) / Counter Guarantee-I (Cg-I) ApplicationAzref MhdNo ratings yet
- Transfer PricingDocument53 pagesTransfer PricingkannnamreddyeswarNo ratings yet
- Debtor-Creditor Cicularization FormateDocument1 pageDebtor-Creditor Cicularization FormateChristopher TateNo ratings yet
- Tenancy ManagementDocument34 pagesTenancy ManagementPraba Karan67% (3)
- Draft D2Document12 pagesDraft D2Choirul AnwarNo ratings yet
- Heavy Equipment Sales ProposalDocument5 pagesHeavy Equipment Sales Proposalyummy playlist mineNo ratings yet
- Expression of InterestDocument8 pagesExpression of InterestgajanandperiwalNo ratings yet
- Adco Company Application Form.Document2 pagesAdco Company Application Form.shobhit mohta67% (3)
- Tax Q&A - Income From Investment and Other SourcesDocument3 pagesTax Q&A - Income From Investment and Other SourcesHadifliNo ratings yet
- NSN Ksa Overtime Policy Version 1 2009Document4 pagesNSN Ksa Overtime Policy Version 1 2009Amr ElsheshtawyNo ratings yet
- MM Quarterly Report Q2 2021Document36 pagesMM Quarterly Report Q2 2021PaulNo ratings yet
- Mobilization Advance Guarantee / Retenation BondDocument4 pagesMobilization Advance Guarantee / Retenation Bondaliengineer953No ratings yet
- Invoices DaburDocument1 pageInvoices Daburaamir aliNo ratings yet
- End of Probation Perio1Document24 pagesEnd of Probation Perio1Ravi RathnayakaNo ratings yet
- Dec 2014Document2 pagesDec 2014Zahiratul QamarinaNo ratings yet
- Application Form: 1. Personal DetailsDocument6 pagesApplication Form: 1. Personal DetailsGareth Cotter100% (1)
- Kurunegala - Site Expenses: in HandDocument22 pagesKurunegala - Site Expenses: in HandKrishan RodrigoNo ratings yet
- Job Description For The Post of Business Development ExecutiveDocument2 pagesJob Description For The Post of Business Development ExecutivePriya SinghNo ratings yet
- External Audit DepartmentDocument3 pagesExternal Audit DepartmentCristine TanggoyocNo ratings yet
- (Your Company Name) (Your State or Jurisdiction)Document7 pages(Your Company Name) (Your State or Jurisdiction)Perimenopause Symptoms100% (1)
- Sample Credit Control PolicyDocument21 pagesSample Credit Control PolicyMozitomNo ratings yet
- Staff Expenses Claim For The Month of Department: NameDocument2 pagesStaff Expenses Claim For The Month of Department: NameDioNo ratings yet
- Solution Test 1Document3 pagesSolution Test 1anis izzatiNo ratings yet
- QuotationDocument2 pagesQuotationAjeet Kumar PandeyNo ratings yet
- Accounting Services Proposal Template (New)Document4 pagesAccounting Services Proposal Template (New)marvbeats1555No ratings yet
- Employment Application FormDocument3 pagesEmployment Application FormamirrulasyrafNo ratings yet
- Charge Sheet - IRLL - Dipesh - ShawDocument2 pagesCharge Sheet - IRLL - Dipesh - ShawDIPESH KUMAR SHAWNo ratings yet
- Corporate Budget Memo No. 39Document95 pagesCorporate Budget Memo No. 39mcla28No ratings yet
- CTG FormDocument1 pageCTG FormSanjeevMishra100% (1)
- Delta Fuels Company ProfileDocument12 pagesDelta Fuels Company ProfileAnonymous 5z7ZOpNo ratings yet
- Integral University, Lucknow: This Is Computer Generated Receipt, No Signature RequiredDocument1 pageIntegral University, Lucknow: This Is Computer Generated Receipt, No Signature RequiredHassan KhanNo ratings yet
- Dcoffee IdeaDocument7 pagesDcoffee IdeaDhananjay DubeyNo ratings yet
- Assessment of Working Capital Requirement: Sheet 1Document13 pagesAssessment of Working Capital Requirement: Sheet 1Arjun YemulNo ratings yet
- Vidyamandir Classes LTD.: Reimbursement SheetDocument3 pagesVidyamandir Classes LTD.: Reimbursement Sheetsudhir_kumar_33No ratings yet
- TERRAGEN DOFTutorialDocument14 pagesTERRAGEN DOFTutorialCresencio TurpoNo ratings yet
- Homework By:: Pratik Pranav - 2018CS10368 Sarthak Behera - 2018CS10384 Shreyans Nagori - 2018CS10390Document4 pagesHomework By:: Pratik Pranav - 2018CS10368 Sarthak Behera - 2018CS10384 Shreyans Nagori - 2018CS10390pratik pranav100% (1)
- Saurabh ResumeDocument1 pageSaurabh Resumesaurabh kashyapNo ratings yet
- Airlines ProjectDocument25 pagesAirlines Projectjyotisinghal1976No ratings yet
- Software Development Processes and Software Quality AssuranceDocument137 pagesSoftware Development Processes and Software Quality AssuranceDoanh DoanhNo ratings yet
- Support Vector MachineDocument22 pagesSupport Vector MachineZakky DayatNo ratings yet
- Amphenol ARINC 600: Rack and Panel ConnectorsDocument18 pagesAmphenol ARINC 600: Rack and Panel ConnectorsCopperAustraliaNo ratings yet
- Quantum Internet: Networking Challenges in Distributed Quantum ComputingDocument9 pagesQuantum Internet: Networking Challenges in Distributed Quantum ComputinghdjskhdkjsNo ratings yet
- Expert SystemsDocument60 pagesExpert SystemsSai Venkat GudlaNo ratings yet
- Mikroprog Suite Pic Dspic Pic32 Manual V100aDocument24 pagesMikroprog Suite Pic Dspic Pic32 Manual V100astranger72_28No ratings yet
- Automobile Tracking System Using Gps and GSM: Jaya Ram Khatri ChhetriDocument49 pagesAutomobile Tracking System Using Gps and GSM: Jaya Ram Khatri Chhetrioluwakayode olabanjiNo ratings yet
- Internet of Things (Iot)Document35 pagesInternet of Things (Iot)zapNo ratings yet
- Soniclear Installation GuideDocument75 pagesSoniclear Installation GuideYetunde AgbetolaNo ratings yet
- BootstrapDocument11 pagesBootstrapKidus DawitNo ratings yet
- National Institute of Technology, Raipur: Smart Irrigation System Using LoraDocument22 pagesNational Institute of Technology, Raipur: Smart Irrigation System Using LoraHimanshu VermaNo ratings yet
- Saurab Gurung 20MC204001 Research MethodologyDocument36 pagesSaurab Gurung 20MC204001 Research Methodologyyogendra sharmaNo ratings yet
- Block DiagramDocument3 pagesBlock DiagramttatontokevinNo ratings yet
- JWeb ServicesDocument52 pagesJWeb ServicesUday KumarNo ratings yet
- UCBrowser User Agent enDocument23 pagesUCBrowser User Agent enGennaro Scala0% (1)
- Ensayo Sobre La CortesíaDocument4 pagesEnsayo Sobre La Cortesíah6867qp4100% (1)
- DS-2CD3123G0E-I (W) (S) Datasheet V5.5.3 20180706Document5 pagesDS-2CD3123G0E-I (W) (S) Datasheet V5.5.3 20180706Sandeep KamatNo ratings yet
- Data Mangement OTMDMDocument98 pagesData Mangement OTMDMChithra SNo ratings yet
- Case Study 5Document1 pageCase Study 5prisweetieNo ratings yet
- Modulation and Frequency Synthesis X Digital Wireless RadioDocument233 pagesModulation and Frequency Synthesis X Digital Wireless Radiolcnblzr3877No ratings yet
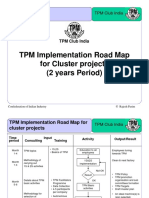
- TPM Road MapDocument4 pagesTPM Road Mapsanjeev singhNo ratings yet
- Practice 1: Introduction To Matlab. Control Toolbox: ObjectiveDocument5 pagesPractice 1: Introduction To Matlab. Control Toolbox: ObjectiveLeonardo PalaciosNo ratings yet
- Fluency With Information Technology 6th Edition Lawrence Snyder Solutions ManualDocument3 pagesFluency With Information Technology 6th Edition Lawrence Snyder Solutions ManualPeggie Edwards100% (34)
- (1c) Linear Programming - Graphical MethodDocument37 pages(1c) Linear Programming - Graphical MethodDennis NavaNo ratings yet