
Anti Scabies
Anti Scabies
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fenton Growth Chart Boy v1Document2 pagesFenton Growth Chart Boy v1nurhapsari20100% (3)
- MRCPExamResult 2 PDFDocument2 pagesMRCPExamResult 2 PDFumair100% (1)
- ESO2 Emergency Ventilator Service Manual 5009585 BDocument100 pagesESO2 Emergency Ventilator Service Manual 5009585 Btech.consultantNo ratings yet
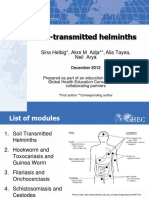
- Introduction To Soil-Transmitted Helminths Dec2012 FINAL - 1Document57 pagesIntroduction To Soil-Transmitted Helminths Dec2012 FINAL - 1Mike Serge RazafiNo ratings yet
- MCQ Calcium Hydroxide: Ca (OH) 2Document3 pagesMCQ Calcium Hydroxide: Ca (OH) 2Alexander LianNo ratings yet
- Answer The Following Questions Based On The Text!: Name: Class: Day/DateDocument2 pagesAnswer The Following Questions Based On The Text!: Name: Class: Day/DateSiti Aisyah SNo ratings yet
- RESEARCH Paper 10Document19 pagesRESEARCH Paper 10RAMEL OÑATENo ratings yet
- PseudochistDocument17 pagesPseudochistrazvanccNo ratings yet
- Anti Autoimmune ProtocolDocument39 pagesAnti Autoimmune Protocolanonyd100% (4)
- Sample Training DesignDocument3 pagesSample Training DesignSAMCH HEMSNo ratings yet
- Report On The Antimicrobial Activity of Graminex Nax 7 Paste 1Document13 pagesReport On The Antimicrobial Activity of Graminex Nax 7 Paste 1api-442513573No ratings yet
- Lawsuit Against PharmacyDocument21 pagesLawsuit Against PharmacyAnthony TalcottNo ratings yet
- 05.12 Anatomy of The Larynx & Physiology of PhonationDocument30 pages05.12 Anatomy of The Larynx & Physiology of PhonationReg LagartejaNo ratings yet
- PHD BrochureDocument28 pagesPHD BrochurealioshaNo ratings yet
- 03 Anaesthesia Machine PDFDocument0 pages03 Anaesthesia Machine PDFjuniorebindaNo ratings yet
- Lab ReportDocument5 pagesLab ReportsuniNo ratings yet
- Choosing A Specialty - ESDocument5 pagesChoosing A Specialty - ESece142No ratings yet
- Research LocaleDocument13 pagesResearch LocaleJovie DacoycoyNo ratings yet
- Documentary Critique Scie1458 4234137Document7 pagesDocumentary Critique Scie1458 4234137api-316134467No ratings yet
- Gnostica News 1974-03-21 Vol 3 Iss 8.editDocument35 pagesGnostica News 1974-03-21 Vol 3 Iss 8.edittempullyboneNo ratings yet
- Tattooing and MicropigmentationDocument2 pagesTattooing and MicropigmentationAlina PiscanuNo ratings yet
- Oxylog 2000 Manual EspañolDocument1 pageOxylog 2000 Manual EspañolDaniel FalconNo ratings yet
- Appendix: Proposed Guideline For The Rehabilitation of Acute Hamstring Strain Injuries Phase 1 (0-4 Weeks)Document6 pagesAppendix: Proposed Guideline For The Rehabilitation of Acute Hamstring Strain Injuries Phase 1 (0-4 Weeks)Yosie PutraNo ratings yet
- Kleptomania and HomoeopathyDocument7 pagesKleptomania and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Acute PsychosisDocument8 pagesAcute PsychosisAnonymous EtiONEG7No ratings yet
- RA Physician Davao Sept2019 PDFDocument10 pagesRA Physician Davao Sept2019 PDFPhilBoardResultsNo ratings yet
- Grinnell G.Document215 pagesGrinnell G.lancasterpdNo ratings yet
- TB AssessmentDocument2 pagesTB AssessmentVaishakh RaviNo ratings yet
- Target Product Profile: A Renaissance For Its Definition and UseDocument9 pagesTarget Product Profile: A Renaissance For Its Definition and UseKavya g nNo ratings yet
- Durian Jelly: An Undergraduate Practical ResearchDocument6 pagesDurian Jelly: An Undergraduate Practical ResearchDOLORFEY L. SUMILE100% (1)




































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fenton Growth Chart Boy v1Document2 pagesFenton Growth Chart Boy v1nurhapsari20100% (3)
- MRCPExamResult 2 PDFDocument2 pagesMRCPExamResult 2 PDFumair100% (1)
- ESO2 Emergency Ventilator Service Manual 5009585 BDocument100 pagesESO2 Emergency Ventilator Service Manual 5009585 Btech.consultantNo ratings yet
- Introduction To Soil-Transmitted Helminths Dec2012 FINAL - 1Document57 pagesIntroduction To Soil-Transmitted Helminths Dec2012 FINAL - 1Mike Serge RazafiNo ratings yet
- MCQ Calcium Hydroxide: Ca (OH) 2Document3 pagesMCQ Calcium Hydroxide: Ca (OH) 2Alexander LianNo ratings yet
- Answer The Following Questions Based On The Text!: Name: Class: Day/DateDocument2 pagesAnswer The Following Questions Based On The Text!: Name: Class: Day/DateSiti Aisyah SNo ratings yet
- RESEARCH Paper 10Document19 pagesRESEARCH Paper 10RAMEL OÑATENo ratings yet
- PseudochistDocument17 pagesPseudochistrazvanccNo ratings yet
- Anti Autoimmune ProtocolDocument39 pagesAnti Autoimmune Protocolanonyd100% (4)
- Sample Training DesignDocument3 pagesSample Training DesignSAMCH HEMSNo ratings yet
- Report On The Antimicrobial Activity of Graminex Nax 7 Paste 1Document13 pagesReport On The Antimicrobial Activity of Graminex Nax 7 Paste 1api-442513573No ratings yet
- Lawsuit Against PharmacyDocument21 pagesLawsuit Against PharmacyAnthony TalcottNo ratings yet
- 05.12 Anatomy of The Larynx & Physiology of PhonationDocument30 pages05.12 Anatomy of The Larynx & Physiology of PhonationReg LagartejaNo ratings yet
- PHD BrochureDocument28 pagesPHD BrochurealioshaNo ratings yet
- 03 Anaesthesia Machine PDFDocument0 pages03 Anaesthesia Machine PDFjuniorebindaNo ratings yet
- Lab ReportDocument5 pagesLab ReportsuniNo ratings yet
- Choosing A Specialty - ESDocument5 pagesChoosing A Specialty - ESece142No ratings yet
- Research LocaleDocument13 pagesResearch LocaleJovie DacoycoyNo ratings yet
- Documentary Critique Scie1458 4234137Document7 pagesDocumentary Critique Scie1458 4234137api-316134467No ratings yet
- Gnostica News 1974-03-21 Vol 3 Iss 8.editDocument35 pagesGnostica News 1974-03-21 Vol 3 Iss 8.edittempullyboneNo ratings yet
- Tattooing and MicropigmentationDocument2 pagesTattooing and MicropigmentationAlina PiscanuNo ratings yet
- Oxylog 2000 Manual EspañolDocument1 pageOxylog 2000 Manual EspañolDaniel FalconNo ratings yet
- Appendix: Proposed Guideline For The Rehabilitation of Acute Hamstring Strain Injuries Phase 1 (0-4 Weeks)Document6 pagesAppendix: Proposed Guideline For The Rehabilitation of Acute Hamstring Strain Injuries Phase 1 (0-4 Weeks)Yosie PutraNo ratings yet
- Kleptomania and HomoeopathyDocument7 pagesKleptomania and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Acute PsychosisDocument8 pagesAcute PsychosisAnonymous EtiONEG7No ratings yet
- RA Physician Davao Sept2019 PDFDocument10 pagesRA Physician Davao Sept2019 PDFPhilBoardResultsNo ratings yet
- Grinnell G.Document215 pagesGrinnell G.lancasterpdNo ratings yet
- TB AssessmentDocument2 pagesTB AssessmentVaishakh RaviNo ratings yet
- Target Product Profile: A Renaissance For Its Definition and UseDocument9 pagesTarget Product Profile: A Renaissance For Its Definition and UseKavya g nNo ratings yet
- Durian Jelly: An Undergraduate Practical ResearchDocument6 pagesDurian Jelly: An Undergraduate Practical ResearchDOLORFEY L. SUMILE100% (1)