Professional Documents
Culture Documents
Treatment Options For Refractoryrelapsed Multiple
Treatment Options For Refractoryrelapsed Multiple
Uploaded by
iman knOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Treatment Options For Refractoryrelapsed Multiple
Treatment Options For Refractoryrelapsed Multiple
Uploaded by
iman knCopyright:
Available Formats
Cancer Management and Research Dovepress
open access to scientific and medical research
Open Access Full Text Article ORIGINAL RESEARCH
Treatment options for refractory/relapsed
multiple myeloma: an updated evidence
Cancer Management and Research downloaded from https://www.dovepress.com/ by 191.101.19.106 on 21-Aug-2018
synthesis by network meta-analysis
This article was published in the following Dove Press journal:
Cancer Management and Research
Xian-Wu Luo 1 Background: The refractory/relapsed multiple myeloma (RRMM) remains a big clinical
Xue-Qing Du 2 challenge, due to its biological and clinical complexity. Leading hematologists have performed
Jie-Li Li 2 many randomized controlled trials (RCTs) worldwide, and their findings were summarized in
Xiao-Ping Liu 3,4 a recently published network meta-analysis (NMA) but with certain limitations.
For personal use only.
Materials and methods: We performed an updated NMA of RCTs related to RRMM treat-
Xiang-Yu Meng 3,4
ment, focusing on efficacy measures including the nonresponse rate (NRR), time to progression
1
Department of Health Management,
(TTP), progression-free survival (PFS), and overall survival (OS). The PubMed database was
School of Health Sciences, Wuhan
University, 2Department of searched. We extended the literature search strategy of a previous NMA to June 30, 2017 and
Hematology, Zhongnan Hospital of included additional primary RCTs. The surface under the cumulative ranking curve (SUCRA)
Wuhan University, 3Department
of Evidence-Based Medicine and was calculated to rank the regimens. A weighted-average method was used to rank the regimens
Clinical Epidemiology, Second Clinical by summarizing SUCRAs across different outcome measures.
School, Wuhan University, 4Center Results: Finally, a total of 24 RCTs were included in this updated NMA. According to the
for Evidence-based and Translational
Medicine, Zhongnan Hospital of result, the combination of daratumumab, lenalidomide, and dexamethasone showed better
Wuhan University, Wuhan, China efficacy than other regimens in terms of NRR, TTP, and PFS (NRR: odds ratio [OR] =0.046,
95% credible interval [CrI] =[0.024, 0.085]; TTP: hazard ratio [HR] =0.14, 95% CrI =[0.092,
0.2]; PFS: HR =0.12, 95% CrI =[0.077, 0.18], compared with dexamethasone singlet). The
combination of ixazomib, lenalidomide, and dexamethasone showed better efficacy than other
regimens in terms of OS (HR =0.30, 95% CrI =[0.17, 0.54], compared with dexamethasone).
The combination of daratumumab, lenalidomide, and dexamethasone ranked first in terms of
overall efficacy (weighted average of SUCRAs =0.920).
Conclusion: The combination of daratumumab, lenalidomide, and dexamethasone may cur-
rently be the most effective regimen in the population of RRMM patients. Triplet regimens
containing daratumumab, ixazomib, carfilzomib, or elotumumab plus lenalidomide and dexa-
methasone can be recommended as first-line therapies for RRMM patients.
Keywords: multiple myeloma, refractory/relapsed, treatment regimens, efficacy, network
meta-analysis
Introduction
Since the early 2000s, the introduction of newly developed agents has dramatically
improved the outcome of patients with multiple myeloma. However, the refractory/
Correspondence: Xiang-Yu Meng relapsed multiple myeloma (RRMM) remains a big challenge, due to its biological
Department of Evidence-Based Medicine
and Clinical Epidemiology, Second Clinical and clinical complexity. In an attempt to find ways to conquer RRMM, world’s leading
School, Wuhan University, 169 Donghu hematologists have performed many randomized controlled trials (RCTs) worldwide.
Road, Wuhan 430071, China
Tel/Fax +86 27 6781 2817
Recently, two research groups have tried to synthesize the results of these trials by
Email mengxy_whu@163.com network meta-analysis (NMA), a statistical analysis method by which a thorough
submit your manuscript | www.dovepress.com Cancer Management and Research 2018:10 2817–2823 2817
Dovepress © 2018 Luo et al. This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.
http://dx.doi.org/10.2147/CMAR.S166640
php and incorporate the Creative Commons Attribution – Non Commercial (unported, v3.0) License (http://creativecommons.org/licenses/by-nc/3.0/). By accessing the work
you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For
permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms (https://www.dovepress.com/terms.php).
Powered by TCPDF (www.tcpdf.org)
Luo et al Dovepress
c omparison and ranking of all included treatment options is Data extraction and statistical analysis
made possible.1,2 However, the two previous NMAs have cer- Two authors (X.W.L. and X.Q.D) independently reviewed
tain limitations. To name a few, in the NMA by van Beurden- the reports. Supplementary materials of the RCTs were
Tan et al,1 important outcomes such as overall survival (OS) included, and the following information was extracted from
were left uninvestigated and the ranking information was not each study report: name of the first author, year of publica-
provided; and in the other NMA by Botta et al,2 regimens tion, trial identifications, treatment regimens used for the
were grouped into categories before comparison, some of
Cancer Management and Research downloaded from https://www.dovepress.com/ by 191.101.19.106 on 21-Aug-2018
experimental and control arms, total number of patients,
which seem inappropriate and may cause bias and confusion. outcome measures investigated, and data for the calculation
Besides, we found that several new RCTs and updated trial of effect size for each outcome.
reports are available for a new NMA. Considering the above, Before NMA, the logarithmic odds ratio (OR) and its
we performed the present study to update the evidence and standard error were calculated for NRR, and the logarithmic
improve its quality using traditional NMA and a self-designed hazard ratio (HR) and its standard error for time-to-event
weighted average method to rank the regimens by summariz- outcomes were original data inputs. Fixed effects Bayesian
ing results across various efficacy outcome measures. NMAs were conducted, and forest plots were generated
with results shown as the HR and corresponding 95% cred-
Materials and methods ible interval (95%CrI). To include all treatments within one
Outcome measures network, bortezomib with or without dexamethasone was
This updated NMA focuses on early and long-term efficacy considered identical and labeled as “bortezomib ± dexa-
For personal use only.
outcomes, including the nonresponse rate (NRR), time to methasone” and thalidomide with or without dexametha-
progression (TTP), progression-free survival (PFS) and OS. sone was considered identical and labeled as “thalidomide
Response rate was considered instead of NRR because its ± dexamethasone” as described in van Beurden-Tan et al.1
outcome event, that is, the absence of objective response The dexamethasone monotherapy was set as the common
to treatment, a negative indicator of treatment efficacy and reference regimen. To rank all regimens, the surface under
prognosis, is similar to events of other outcome measures, the cumulative ranking curve (SUCRA) was calculated
which allows ranking by summarizing results across all these for each outcome as described in Salanti et al 3 for a given
outcome measures. regimen. A larger SUCRA score indicated better efficacy in
terms of a specific outcome measure. For the final ranking
Literature search and study selection regarding the overall efficacy, an arithmetic weighted average
The PubMed database was searched. We adopted the lit- of SUCRA scores across NRR, PFS, and OS was calculated.
erature search strategy described by Botta et al.2 In brief, A 20%, 35%, and 45% weight was given to the NRR, PFS,
all possible combinations of the following search terms and OS, respectively. These weights were given in accordance
were used for searching RCTs concerning RRMM patients: with the importance of the outcome measures. We consid-
“multiple myeloma,” “relapse,” “refractory,” “randomized,” ered the OS the most important, PFS as the surrogate of OS
“management,” “regimen,” and “therapy.” No specific filters the second most important, and NRR that reflects the early
were used during the search. The time range of the search was efficacy the least important. There was only one exception,
between the January 1, 2000 and June 30, 2017. oblimersen plus dexamethasone, for which data on PFS and
The following predefined eligibility criteria were used OS were not available, thus an 80% weight was attributed
for the study selection: 1) the study should be an RCT; 2) to TTP. A larger weighted average of SUCRAs indicated a
the subjects should be RRMM patients; 3) at least two dif- higher rank in terms of overall efficacy. The R software ver-
ferent regimens were compared in the study, except for those sion 3.1.2 and the gemtc package were used to perform all
comparing different dosing schemes or modes of administra- the statistical analyses.
tions; 4) data for at least one of the outcome measures were
available. Studies that did not match any of the above criteria Results
were excluded. Basic information of included RCTs
Two authors (X.W.L. and X.Q.D.) independently per- After literature search and study selection, a total of 29
formed the literature search and study selection and discussed trial reports published between 2005 and 2017 were con-
with the third author (X.M.) to resolve any discrepancies. sidered eligible to be included in the NMA. As a result, 24
2818 submit your manuscript | www.dovepress.com Cancer Management and Research 2018:10
Dovepress
Powered by TCPDF (www.tcpdf.org)
Dovepress Treatment options for refractory/relapsed multiple myeloma
independent studies, with a total of 10,853 subjects and 21 Ranking of regimens by SUCRA
different regimens were included in the present study. Com- As shown in Table 2, the ranking by SUCRA scores for each
pared with the inclusion results by Botta et al,2 an additional efficacy outcome was generally consistent with NMA find-
seven references4–10 were included, among which four were ings. The combination of daratumumab, lenalidomide, and
newly identified studies4,5,9,10 and three were updated study dexamethasone ranked first for NRR (SUCRA =0.984), TTP
results.6–8 The basic information of the included references (SUCRA =0.988), and PFS (SUCRA =0.999). The combina-
has been summarized in Table 1.
Cancer Management and Research downloaded from https://www.dovepress.com/ by 191.101.19.106 on 21-Aug-2018
tion of ixazomib, lenalidomide, and dexamethasone ranked
first for OS (SUCRA =0.972).
NMA results In terms of overall efficacy measured by the weighted
According to the results of NMAs, the combination of dara- average of SUCRAs, the combination of daratumumab,
tumumab, lenalidomide, and dexamethasone was the most lenalidomide, and dexamethasone ranked on top (weighted
effective therapy in terms of NRR, TTP, and PFS (NRR: average =0.920), followed by the combination of ixazomib,
OR =0.046, 95% CrI =[0.024, 0.085]; TTP: HR =0.14, 95% lenalidomide, and dexamethasone (weighted average =0.907).
CrI =[0.092, 0.2]; PFS: HR =0.12, 95% CrI =[0.077, 0.18],
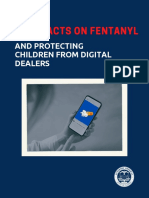
compared with dexamethasone singlet; Figure 1A–C), and the Discussion
combination of ixazomib, lenalidomide, and dexamethasone Regardless of recent progress in management, RRMM is still
is the most effective one in terms of OS (HR =0.12, 95%CrI an incurable disease, which has been attracting substantial
=[0.17, 0.54]; Figure 1D). research attention. In the past decades, a large number of
For personal use only.
Table 1 Basic information of included RCT reports
Authors Year Trial Identification Arm 1 Arm 2 N Outcome
Richardson et al 11
2005 APEX BOR DEX 627 NRR, TTP, OS
Richardson et al12 2007 APEX BOR DEX 627 NRR, TTP, OS
Dimopoulos et al13 2007 MM-010 LEN + DEX DEX 351 NRR, TTP, OS
Orlowski et al14 2007 DOXIL-MMY-3001 BOR + plDOX BOR + DEX 646 NRR, TTP, PFS, OS
Weber et al15 2007 MM-009 LEN + DEX DEX 353 NRR, TTP, OS
Chanan-Khan et al16 2009 GMY302 OBL + DEX DEX 224 NRR, TTP
Dimopoulos et al17 2009 MM-009 & MM-010 LEN + DEX DEX 704 PFS, OS
Garderet et al18 2012 MMVAR/IFM 2005-04 BOR + THA + DEX THA + DEX 244 NRR, TTP, PFS, OS
Hjorth et al19 2012 NCT00602511 THA + DEX BOR + DEX 131 NRR, PFS, OS
Kropff et al20 2012 OPTIMUM THA DEX 499 NRR, TTP, PFS, OS
Dimopoulos et al21 2013 VANTAGE 088 VOR + BOR BOR 635 NRR, TTP, PFS, OS
San-Miguel et al4 2013 MM-003 POM + DEX DEX 455 NRR, TTP, PFS, OS
White et al.22 2013 AMBER BEV + BOR BOR 102 NRR, PFS, OS
Morgan et al6 2014 MM-003 POM + DEX DEX 455 OS
Richardson et al5 2014 MM-002 POM + DEX POM 221 NRR, PFS, OS
San-Miguel et al23 2014 PANORAMA1 PAN + BOR + DEX BOR + DEX 768 NRR, TTP, PFS, OS
Lonial et al24 2015 ELOQUENT-2 ELO + LEN + DEX LEN + DEX 646 NRR, PFS
Orlowski et al25 2015 NCT00401843 SIL + BOR BOR 268 NRR, TTP, PFS, OS
Stewart et al26 2015 ASPIRE CAR + LEN + DEX LEN + DEX 792 NRR, PFS, OS
Dimopoulos et al27 2016 POLLUX DAR + LEN + DEX LEN + DEX 557 NRR, TTP, PFS, OS
Dimopoulos et al28 2016 ENDEAVOR CAR + DEX BOR + DEX 929 NRR, PFS, OS
Jakubowiak et al29 2016 NCT01478048 ELO + BOR + DEX BOR + DEX 152 NRR, PFS, OS
Moreau et al30 2016 TOURMALINE-MM1 IXA + LEN + DEX LEN + DEX 722 NRR, TTP, PFS
Orlowski et al31 2016 DOXIL-MMY-3001 BOR + plDOX BOR + DEX 646 OS
Palumbo et al32 2016 CASTOR DAR + BOR + DEX BOR + DEX 474 NRR, TTP, PFS, OS
San-Miguel et al7 2016 PANORAMA 1 PAN + BOR + DEX BOR + DEX 768 OS
Dimopoulos et al8 2017 ELOQUENT-2 ELO + LEN + DEX LEN + DEX 646 PFS, OS
Hou et al10 2017 NCT01564537 IXA + LEN + DEX LEN + DEX 115 NRR, TTP, PFS, OS
Hajek et al9 2017 FOCUS CAR DEX 315 NRR, PFS, OS
Abbreviations: BOR, bortezomib; BEV, bevacizumab; CAR, carfilzomib; DAR, daratumumab; DEX, dexamethasone; plDOX, Pegylated liposomal doxorubicin;
ELO, elotumumab; IXA, ixazomib; LEN, lenalidomide; OBL, oblimersen; POM, pomalidomide; SIL, siltuximab; THA, thalidomide; NRR, non-response rate; PAN, panobinostat;
PFS, progression-free survival; TTP, time to progression; OS, overall survival; N, number of patients; VOR, vorinostat.
Cancer Management and Research 2018:10 submit your manuscript | www.dovepress.com
2819
Dovepress
Powered by TCPDF (www.tcpdf.org)
Luo et al Dovepress
A Regimens OR (95% Crl) B Regimens HR (95% Crl)
Daratumumab+Lenalidomide+Dexamethasone 0.46 (0.024–0.085) Daratumumab+Lenalidomide+Dexamethasone 0.14 (0.092–0.2)
Carfilzombib+Lenalidomide+Dexamethasone 0.054 (0.033– 0.088) Carfilzombib+Lenalidomide+Dexamethasone 0.26 (0.19–0.34)
Elotuzumab+Lenalidomide+Dexamethasone 0.095 (0.059– 0.15) Ixazomib+Lenalidomide+Dexamethasone 0.26 (0.20–0.35)
Elotuzumab+Lenalidomide+Dexamethasone 0.27 (0.20–0.35)
Ixazomib+Lenalidomide+Dexamethasone 0.11 (0.072–0.18)
Daratumumab+Bortezomib+Dexamethasone 0.31 (0.18–0.52)
Daratumumab+Bortezomib+Dexamethasone 0.12 (0.072– 0.21)
Lenalidomide+Dexamethasone 0.37 (0.30–0.45)
Carfilzombib+Dexamethasone 0.18 (0.11–0.28)
Carfilzombib+Dexamethasone 0.41 (0.26–0.67)
Lenalidomide+Dexamethasone 0.18 (0.13– 0.25) Bortezomib+Thalidomide+Dexamethasone 0.44 (0.29–0.67)
Vorinostat+Bortezomib 0.19 (0.12–0.30) Panobinostat+Bortezomib+Dexamethasone 0.45 (0.28–0.73)
Pomalidomide+Dexamethasone 0.24 (0.13–0.42) Pegylated liposomal doxorubicin+Bortezomib 0.46 (0.28–0.76)
Siltuximab+Bortezomib
Cancer Management and Research downloaded from https://www.dovepress.com/ by 191.101.19.106 on 21-Aug-2018
0.25 (0.14–0.45) Pomalidomide+Dexamethasone 0.48 (0.39–0.59)
Bevacizumab+Bortezomib 0.26 (0.11–0.60) Bevacizumab+Bortezomib 0.58 (0.29–1.20)
Panobinostat+Bortezomib+Dexamethasone 0.27 (0.17–0.42) Elotuzumab+Bortezomib+Dexamethasone 0.59 (0.34–1.00)
Elotuzumab+Bortezomib+Dexamethasone 0.30 (0.14–0.63) Vorinostat+Bortezomib 0.61 (0.38–0.98)
Pegylated liposomal doxorubicin+Bortezomib 0.31 (0.19–0.48) Siltuximab+Bortezomib 0.68 (0.40–1.10)
Bortezomib+/-Dexamethason 0.35 (0.25–0.49) Pomalidomide 0.71 (0.50–1.00)
Pomalidomide Thalidomide+/-Dexamethasone 0.72 (0.53–0.98)
0.49 (0.21–1.20)
Bortezomib+/-Dexamethason 0.78 (0.51–1.20)
Carfilzombib 0.54 (0.29–1.00)
Dexamethasone 1
Bortezomib+Thalidomide+Dexamethasone 0.58 (0.29–1.10) Carfilzombib 1. 1 (0.84–1.40)
Thalidomide+/-Dexamethasone 0.90 (0.58–1.40)
Dexamethasone 1 0.08 0.32 1.28
Oblimersen+Dexamethasone 1.20 ( 0.57– 2.40)
0.01 0.04 0.16 0.64 2.56
C D Regimens HR (95% Crl)
0.30 (0.17–0.54)
For personal use only.
Ixazomib+Lenalidomide+Dexamethasone
Daratumumab+Lenalidomide+Dexamethasone 0.46 (0.28–0.75)
Regimens HR (95% Crl) Pomalidomide+Dexamethasone 0.52 (0.39–0.69)
Daratumumab+Lenalidomide+Dexamethasone 0.12 (0.077–0.18) Bevacizumab+Bortezomib 0.54 (0.22–1.40)
Daratumumab+Bortezomib+Dexamethasone 0.17 (0.10–0.26) Elotuzumab+Lenalidomide+Dexamethasone 0.55 (0.41–0.74)
Ixazomib+Lenalidomide+Dexamethasone 0.24 (0.18–0.32) Pomalidomide 0.55 (0.37–0.83)
Pegylated liposomal doxorubicin+Bortezomib 0.30 (0.21–0.44) Bortezomib+Thalidomide+Dexamethasone 0.56 (0.35–0.89)
Panobinostat+Bortezomib+Dexamethasone 0 32 (0.22–0.45) Carfilzombib+Lenalidomide+Dexamethasone 0.56 (0.42–0.76)
Lenalidomide+Dexamethasone Elotuzumab+Bortezomib+Dexamethasone 0.64 (0.37–1.10)
0.35 (0.29–0.42)
Bortezomib+Thalidomide+Dexamethasone Daratumumab+Bortezomib+Dexamethasone 0.66 (0.38–1.10)
0.39 (0.24–0.61)
Vorinostat+Bortezomib Carfilzombib+Dexamethasone 0.67 (0.46–0.98)
0.43 (0.30–0.62)
Lenalidomide+Dexamethasone 0.71 (0.59–0.87)
Pomalidomide+Dexamethasone 0.46 (0.36–0.59)
Vorinostat+Bortezomib 0.73 (0.50–1.10)
Siltuximab+Bortezomib 0.47 (0.31– 0.71)
Panobinostat+Bortezomib+Dexamethasone 0.80 (0.61–1.10)
Bortezomib+/-Dexamethason 0.55 (0.41–0.74) Thalidomide+/-Dexamethasone 0.80 (0.64–1.00)
Thalidomide+/-Dexamethasone 0.82 (0.68–0.99)
Pegylated liposomal doxorubicin+Bortezomib 0.81 (0.62–1.10)
Dexamethasone 1 Bortezomib+/-Dexamethason 0.85 (0.69–1.00)
Oblimersen+Dexamethasone 1.10 (0.95–1.20) Carfilzombib 0.97 (0.76–1.20)
Dexamethasone 1
0.05 0.1 0.2 0.4 0.8 1.6 Siltuximab+Bortezomib 1.20 (0.76–1.80)
0.1 0.4 1.6
Figure 1 Forest plots presenting results of network meta-analysis: (A) nonresponse rate, (B) progression-free survival, (C) time to progression, (D) overall survival.
Abbreviations: OR, odds ratio; CrI, credible interval; HR, hazard ratio.
RCTs concerning RRMM treatment were published, in According to our results, the combination of daratu-
which dozens of novel therapeutic regimens were tested and mumab, lenalidomide, and dexamethasone was most effec-
examined. Efforts were made to quantitatively summarize the tive in terms of NRR, TTP, and PFS. However, in terms of
evidence from RCTs by performing NMA, in order to provide OS, it was less effective compared with the combination of
useful and important information for clinical decision-mak- ixazomib, lenalidomide, and dexamethasone. Ranking by
ing at minimal cost. However, flawed analyses may result in overall efficacy showed that the daratumumab, lenalidomide,
misleading conclusions. On the other hand, updates of NMAs and dexamethasone triplet regimen had better performance
on a timely basis are the key to keep the evidence “alive.” The than other regimens. Interestingly, we noted that the 21
present study included the most recently published trials and regimens investigated in this NMA can be categorized into
updates of previous trial reports, thoroughly investigated the three subgroups based on the weighted average of SUCRA
efficacy profiles of 21 treatment options, and avoided certain scores. The first subgroup includes four regimens (19.0%,
limitations of previous NMAs mentioned above. weighted average from ~0.8 to ~0.9), which are the most
2820 submit your manuscript | www.dovepress.com Cancer Management and Research 2018:10
Dovepress
Powered by TCPDF (www.tcpdf.org)
Dovepress Treatment options for refractory/relapsed multiple myeloma
Table 2 Included regimens, SUCRAs, weighted averages of SUCRAs across NRR, TTP, and OS, and ranks in terms of overall efficacy
Regimens NRR TTP PFS OS Weighted Rank
average
Daratumumab + lenalidomide + dexamethasone 0.984 0.988 0.999 0.829 0.920 1
Ixazomib + lenalidomide + dexamethasone 0.828 0.828 0.869 0.972 0.907 2
Carfilzomib + lenalidomide + dexamethasone 0.964 NA 0.887 0.697 0.817 3
Elotuzumab + lenalidomide + dexamethasone 0.873 NA 0.855 0.72 0.798 4
Cancer Management and Research downloaded from https://www.dovepress.com/ by 191.101.19.106 on 21-Aug-2018
Daratumumab + bortezomib + dexamethasone 0.813 0.927 0.812 0.539 0.689 5
Pomalidomide + dexamethasone 0.539 0.393 0.512 0.771 0.634 6
Carfilzomib + dexamethasone 0.683 NA 0.638 0.527 0.597 7
Lenalidomide + dexamethasone 0.66 0.609 0.685 0.447 0.572 8
Bortezomib + thalidomide + dexamethasone 0.202 0.531 0.581 0.689 0.554 9
Bevacizumab + bortezomib 0.5 NA 0.38 0.656 0.528 10
Elotuzumab + bortezomib + dexamethasone 0.429 NA 0.358 0.564 0.465 11
Pomalidomide monotherapy 0.252 NA 0.25 0.698 0.452 12
Vorinostat + bortezomib 0.661 0.446 0.342 0.433 0.447 13
Panobinostat + bortezomib + dexamethasone 0.472 0.678 0.566 0.327 0.43965 14
Pegylated liposomal doxorubicin + bortezomib 0.406 0.715 0.55 0.305 0.41095 15
Thalidomide ± dexamethasone 0.083 0.153 0.221 0.325 0.2402 16
Bortezomib ± dexamethason 0.329 0.263 0.149 0.235 0.2237 17
Siltuximab + bortezomib 0.511 0.391 0.259 0.048 0.21445 18
For personal use only.
Carfilzomib monotherapy 0.214 NA 0.029 0.132 0.11235 19
Dexamethasone monotherapy 0.057 0.068 0.059 0.089 0.0721 20
Oblimersen + dexamethasone* 0.041 0.011 NA NA 0.017 21
Notes: A 20%, 35%, and 45% weight was given to the NRR, PFS, and OS, respectively. *Since data on PFS and OS were not available, a 20% and 80% weight was assigned
to NRR and TTP, respectively.
Abbreviations: NA, not available; NRR, non-response rate; TTP, time-to-progression; PFS, progression-free survival; OS, overall survival.
effective ones, with lenalidomide and dexamethasone as the OS, respectively. We did not take safety into account, because
backbone plus one of the four latest agents (daratumumab, to date no adequate data were available to include all treatment
ixazomib, carfilzomib, or elotumumab). The second subgroup options in one network for any single adverse event outcome.
includes 11 regimens (52.4%, weighted average from ~0.4 to A systematic review less quantitatively intense may be a good
~0.7), which show moderate efficacy in RRMM patients and choice for further investigation on safety profiles. We do not
are mostly doublet or triplet regimens. The third subgroup recommend any ranking based on a combined quantitative
includes six regimens (28.6%, weighted average from 0.0 to analysis of efficacy and safety, because they are two facets
0.25), which are mostly singlet or doublet regimens having distinct from one another, and it is very difficult to assign a
limited efficacy. rational and appropriate weight to each outcome.
An important advantage of NMA over traditional meta- The present study, similar to its preceding works, also
analysis is the possibility of ranking multiple treatment options. has some limitations. First, although the relative impor-
The SUCRA score, derived from the probability that a given tance of different outcome measures was considered, the
treatment has a certain rank and calculated from the posterior appropriateness of the arbitrary assignment of weights
distributions of all treatments, is widely used for ranking needs further verification. Besides, it should acknowledge
treatments in Bayesian NMAs. In this study, we applied a the limitations of the NMA fully when comparing benefits
weighted averaging strategy to rank the regimens for overall from the experimental treatments in patient populations that
efficacy. We assigned weights to different outcome measures differ in previous treatments, cytogenetic risks, subsequent
in accordance with their importance. The OS is the “gold stem-cell transplantation, maintenance therapy, and so on.
standard” outcome measure for the evaluation of long-term Although it could be possible to make adjustment by using
anticancer efficacy, the PFS and TTP are widely acknowledged approaches such as network meta-regression, the immatu-
surrogates of OS, and the treatment response associated with rity of methodology, limited number of included trials and
early efficacy may differ from long-term outcomes. Therefore, frequent missingness in certain study-level variables make
we gave a 20%, 35%, and 45% weight to NRR, PFS/TTP, and it difficult and less reliable.
Cancer Management and Research 2018:10 submit your manuscript | www.dovepress.com
2821
Dovepress
Powered by TCPDF (www.tcpdf.org)
Luo et al Dovepress
Conclusion 15. Weber DM, Chen C, Niesvizky R, et al. Lenalidomide plus dexametha-
sone for relapsed multiple myeloma in North America. N Engl J Med.
In conclusion, the combination of daratumumab, lenalido- 2007;357(21):2133–2142.
mide, and dexamethasone may currently be the most effec- 16. Chanan-Khan AA, Niesvizky R, Hohl RJ, et al. Phase III randomised
study of dexamethasone with or without oblimersen sodium for patients
tive regimen in the population of RRMM patients. Triplet with advanced multiple myeloma. Leuk Lymphoma. 2009;50(4):
regimens containing daratumumab, ixazomib, carfilzomib, 559–565.
or elotumumab plus lenalidomide and dexamethasone can be 17. Dimopoulos MA, Chen C, Spencer A, et al. Long-term follow-up on
overall survival from the MM-009 and MM-010 phase III trials of
Cancer Management and Research downloaded from https://www.dovepress.com/ by 191.101.19.106 on 21-Aug-2018
recommended as the first-line therapies for RRMM patients. lenalidomide plus dexamethasone in patients with relapsed or refractory
multiple myeloma. Leukemia. 2009;23(11):2147–2152.
Disclosure 18. Garderet L, Iacobelli S, Moreau P, et al. Superiority of the triple
combination of bortezomib-thalidomide-dexamethasone over the dual
The authors report no conflicts of interest in this work. combination of thalidomide-dexamethasone in patients with multiple
myeloma progressing or relapsing after autologous transplantation: the
MMVAR/IFM 2005-04 Randomized Phase III Trial from the Chronic
References Leukemia Working Party of the European Group for Blood and Marrow
1. van Beurden-Tan CHY, Franken MG, Blommestein HM, Uyl-de Groot Transplantation. J Clin Oncol. 2012;30(20):2475–2482.
CA, Sonneveld P. Systematic literature review and network meta- 19. Hjorth M, Hjertner O, Knudsen LM, et al. Thalidomide and dexa-
analysis of treatment outcomes in relapsed and/or refractory multiple methasone vs. bortezomib and dexamethasone for melphalan refractory
myeloma. J Clin Oncol. 2017;35(12):1312–1319. myeloma: a randomized study. Eur J Haematol. 2012;88(6):485–496.
2. Botta DCC, Ciliberto D, Rossi M, et al. Network meta-analysis of 20. Kropff M, Baylon HG, Hillengass J, et al. Thalidomide versus dexa-
randomized trials in multiple myeloma: efficacy and safety in relapsed/ methasone for the treatment of relapsed and/or refractory multiple
refractory patients. Blood Adv. 2017;1(7):455–466. myeloma: results from OPTIMUM, a randomized trial. Haematologica.
3. Salanti G, Ades AE, Ioannidis JP. Graphical methods and numerical 2012;97(5):784–791.
For personal use only.
summaries for presenting results from multiple-treatment meta-analysis: 21. Dimopoulos M, Siegel DS, Lonial S, et al. Vorinostat or placebo in
an overview and tutorial. J Clin Epidemiol. 2011;64(2):163–171. combination with bortezomib in patients with multiple myeloma
4. San Miguel J, Weisel K, Moreau P, et al. Pomalidomide plus low-dose (VANTAGE 088): a multicentre, randomised, double-blind study. Lancet
dexamethasone versus high-dose dexamethasone alone for patients with Oncol. 2013;14(11):1129–1140.
relapsed and refractory multiple myeloma (MM-003): a randomised, 22. White D, Kassim A, Bhaskar B, Yi J, Wamstad K, Paton VE. Results from
open-label, phase 3 trial. Lancet Oncol. 2013;14(11):1055–1066. AMBER, a randomized phase 2 study of bevacizumab and bortezomib
5. Richardson PG, Siegel DS, Vij R, et al. Pomalidomide alone or in combi- versus bortezomib in relapsed or refractory multiple myeloma. Cancer.
nation with low-dose dexamethasone in relapsed and refractory multiple 2013;119(2):339–347.
myeloma: a randomized phase 2 study. Blood. 2014;123(12):1826–1832. 23. San-Miguel JF, Hungria VT, Yoon SS, et al. Panobinostat plus bort-
6. Morgan G, Palumbo A, Dhanasiri S, et al. Overall survival of relapsed ezomib and dexamethasone versus placebo plus bortezomib and dexa-
and refractory multiple myeloma patients after adjusting for crossover methasone in patients with relapsed or relapsed and refractory multiple
in the MM-003 trial for pomalidomide plus low-dose dexamethasone. myeloma: a multicentre, randomised, double-blind phase 3 trial. Lancet
Br J Haematol. 2015;168(6):820–823. Oncol. 2014;15(11):1195–1206.
7. San-Miguel JF, Hungria VT, Yoon SS, et al. Overall survival of patients 24. Lonial S, Dimopoulos M, Palumbo A, et al. Elotuzumab therapy for
with relapsed multiple myeloma treated with panobinostat or placebo plus relapsed or refractory multiple myeloma. N Engl J Med. 2015;373(7):
bortezomib and dexamethasone (the PANORAMA 1 trial): a randomised, 621–631.
placebo-controlled, phase 3 trial. Lancet Haematol. 2016;3(11):e506–e515. 25. Orlowski RZ, Gercheva L, Williams C, et al. A phase 2, randomized,
8. Dimopoulos MA, Lonial S, White D, et al. Elotuzumab plus lenalido- double-blind, placebo-controlled study of siltuximab (anti-IL-6 mAb)
mide/dexamethasone for relapsed or refractory multiple myeloma: and bortezomib versus bortezomib alone in patients with relapsed or
ELOQUENT-2 follow-up and post-hoc analyses on progression-free refractory multiple myeloma. Am J Heamtol. 2015;90(1):42–49.
survival and tumour growth. Br J Haematol. 2017;178(6):896–905. 26. Stewart AK, Rajkumar SV, Dimopoulos MA, et al. Carfilzomib,
9. Hajek R, Masszi T, Petrucci MT, et al. A randomized phase III study of lenalidomide, and dexamethasone for relapsed multiple myeloma. N
carfilzomib vs low-dose corticosteroids with optional cyclophosphamide Engl J Med. 2015;372(2):142–152.
in relapsed and refractory multiple myeloma (FOCUS). Leukemia. 27. Dimopoulos MA, Oriol A, Nahi H, et al. Daratumumab, lenalidomide,
2017;31(1):107–114. and dexamethasone for multiple myeloma. N Engl J Med. 2016;375(14):
10. Hou J, Jin J, Xu Y, et al. Randomized, double-blind, placebo-controlled 1319–1331.
phase III study of ixazomib plus lenalidomide-dexamethasone in 28. Dimopoulos MA, Moreau P, Palumbo A, et al. Carfilzomib and dexa-
patients with relapsed/refractory multiple myeloma: China Continuation methasone versus bortezomib and dexamethasone for patients with
study. J Hematol Oncol. 2017;10(1):137. relapsed or refractory multiple myeloma (ENDEAVOR): a randomised,
11. Richardson PG, Sonneveld P, Schuster MW, et al. Bortezomib or high- phase 3, open-label, multicentre study. Lancet Oncol. 2016;17(1):27–38.
dose dexamethasone for relapsed multiple myeloma. N Engl J Med. 29. Jakubowiak A, Offidani M, Pegourie B, et al. Randomized phase 2 study:
2005;352(24):2487–2498. elotuzumab plus bortezomib/dexamethasone vs bortezomib/dexametha-
12. Richardson PG, Sonneveld P, Schuster M, et al. Extended follow-up of sone for relapsed/refractory MM. Blood. 2016;127(23):2833–2840.
a phase 3 trial in relapsed multiple myeloma: final time-to-event results 30. Moreau P, Masszi T, Grzasko N, et al. Oral ixazomib, lenalido-
of the APEX trial. Blood. 2007;110(10):3557–3560. mide, and dexamethasone for multiple myeloma. N Engl J Med.
13. Dimopoulos M, Spencer A, Attal M, et al. Lenalidomide plus dexa- 2016;374(17):1621–1634.
methasone for relapsed or refractory multiple myeloma. N Engl J Med. 31. Orlowski RZ, Nagler A, Sonneveld P, et al. Final overall survival results
2007;357(21):2123–2132. of a randomized trial comparing bortezomib plus pegylated liposomal
14. Orlowski RZ, Nagler A, Sonneveld P, et al. Randomized phase III doxorubicin with bortezomib alone in patients with relapsed or refrac-
study of pegylated liposomal doxorubicin plus bortezomib compared tory multiple myeloma. Cancer. 2016;122(13):2050–2056.
with bortezomib alone in relapsed or refractory multiple myeloma: 32. Palumbo A, Chanan-Khan A, Weisel K, et al. Daratumumab, bort-
combination therapy improves time to progression. J Clin Oncol. ezomib, and dexamethasone for multiple myeloma. N Engl J Med.
2007;25(25):3892–3901. 2016;375(8):754–766.
2822 submit your manuscript | www.dovepress.com Cancer Management and Research 2018:10
Dovepress
Powered by TCPDF (www.tcpdf.org)
Dovepress Treatment options for refractory/relapsed multiple myeloma
Cancer Management and Research downloaded from https://www.dovepress.com/ by 191.101.19.106 on 21-Aug-2018
For personal use only.
Cancer Management and Research Dovepress
Publish your work in this journal
Cancer Management and Research is an international, peer-reviewed a very quick and fair peer-review system, which is all easy to use. Visit
open access journal focusing on cancer research and the optimal use of http://www.dovepress.com/testimonials.php to read real quotes from
preventative and integrated treatment interventions to achieve improved published authors.
outcomes, enhanced survival and quality of life for the cancer patient.
The manuscript management system is completely online and includes
Submit your manuscript here: https://www.dovepress.com/cancer-management-and-research-journal
Cancer Management and Research 2018:10 submit your manuscript | www.dovepress.com
2823
Dovepress
Powered by TCPDF (www.tcpdf.org)
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- DDS ReviewDocument30 pagesDDS ReviewIvymae TrillesNo ratings yet
- Diss Method DevDocument17 pagesDiss Method DevAnnisaIndahPNo ratings yet
- Drug Profile ChlorphenramineDocument16 pagesDrug Profile ChlorphenramineMuhammad Ali RizviNo ratings yet
- Antiparkinsons DrugsDocument19 pagesAntiparkinsons Drugs39 Nayan BhagatNo ratings yet
- GP Drug List Full-130505Document14 pagesGP Drug List Full-130505zilott90No ratings yet
- Fentanyl Patch NHSDocument2 pagesFentanyl Patch NHSkhangsiean89No ratings yet
- Postoperative CareDocument4 pagesPostoperative CareacqueNo ratings yet
- General Information Fast Facts On FentanylDocument8 pagesGeneral Information Fast Facts On FentanylAnthony TalcottNo ratings yet
- 8-Drugs Used in Anxiety and Panic Disprder (Edited)Document11 pages8-Drugs Used in Anxiety and Panic Disprder (Edited)ana01210761809No ratings yet
- EPIDocument2 pagesEPIJoseph MandigmaNo ratings yet
- Form Gdoc Febuari 2024Document84 pagesForm Gdoc Febuari 2024apotekcahayapakalNo ratings yet
- Opiods MorphineDocument4 pagesOpiods MorphinevysakhmohanannairNo ratings yet
- Komplikasi Pain ManagementDocument60 pagesKomplikasi Pain ManagementSigit SutantoNo ratings yet
- March, To It Now Being The Vast Majority of Our Sequenced CasesDocument6 pagesMarch, To It Now Being The Vast Majority of Our Sequenced Cases01 LudviaNo ratings yet
- K Etorolac Tormethamine PDFDocument19 pagesK Etorolac Tormethamine PDFMuhammad Khairun NNo ratings yet
- Cardiovascular PharmacologyDocument61 pagesCardiovascular PharmacologyTeeOne920% (1)
- Anti GlaucomadrugsDocument31 pagesAnti GlaucomadrugsAshu KhanNo ratings yet
- Drug StudyDocument2 pagesDrug StudyNURSETOPNOTCHER100% (3)
- Nursing Record: Student Name: Student IDDocument5 pagesNursing Record: Student Name: Student IDHaneenNo ratings yet
- Internship Mercury DrugDocument4 pagesInternship Mercury DrugjadeNo ratings yet
- Tapazole (Methimazole)Document2 pagesTapazole (Methimazole)CassieNo ratings yet
- Kerala - Floods - List of Medicines Required at Each District in KeralaDocument5 pagesKerala - Floods - List of Medicines Required at Each District in KeralaDhiru bhaiNo ratings yet
- Astrazeneca India Private Limited: Advantage KarnatakaDocument3 pagesAstrazeneca India Private Limited: Advantage KarnatakaPrasath GNo ratings yet
- EntroDocument23 pagesEntroSS RUTVIJ REDDYNo ratings yet
- Perspectives in PharmacyDocument7 pagesPerspectives in Pharmacyjonette carataoNo ratings yet
- SOP VerifikasoDocument85 pagesSOP Verifikasofransiska labuNo ratings yet
- Anupam AntifungalDocument32 pagesAnupam AntifungalShreeharsh SharmaNo ratings yet
- Azilsartan Medoxomil (Edarbi)Document15 pagesAzilsartan Medoxomil (Edarbi)nicasioaquinoNo ratings yet
- Produk Knowledge ZenithDocument1 pageProduk Knowledge ZenithFungky Firdi Lastuti AziliaNo ratings yet
- Anti ParkinsonsDocument4 pagesAnti ParkinsonsMichaela BernadasNo ratings yet