Download as pdf or txt
You might also like
- Misoprostol For Induction of Labor With A Live FetusDocument4 pagesMisoprostol For Induction of Labor With A Live FetusUlfaa MutiaaNo ratings yet
- Comparison of Vaginal and Oral Doses of Misoprostol For Labour Induction in Post-Term PregnanciesDocument4 pagesComparison of Vaginal and Oral Doses of Misoprostol For Labour Induction in Post-Term Pregnanciesnur ulfahNo ratings yet
- Thesis PaperDocument5 pagesThesis PaperbhalNo ratings yet
- Facchinetti 2005Document5 pagesFacchinetti 2005Sri HariNo ratings yet
- Early Amniotomy After Vaginal Misoprostol For Induction of Labor: A Randomized Clinical TrialDocument5 pagesEarly Amniotomy After Vaginal Misoprostol For Induction of Labor: A Randomized Clinical Trialbidan22No ratings yet
- INDUKSIDocument17 pagesINDUKSIKukuh PrasetyoNo ratings yet
- Review: Expert Committee Member MISOPROSTOL (Low Dose For Labour Induction at Term) Author: Lenita WannmacherDocument13 pagesReview: Expert Committee Member MISOPROSTOL (Low Dose For Labour Induction at Term) Author: Lenita WannmacherTri YuliasihNo ratings yet
- Synopsis For Foley Plus Miso Vs Miso Alone in Induction of LabourDocument5 pagesSynopsis For Foley Plus Miso Vs Miso Alone in Induction of LabourAshish TomarNo ratings yet
- Jurnal 2 MisoprostolDocument17 pagesJurnal 2 MisoprostolaldoNo ratings yet
- Comparison Between Vaginal and Sublingual Misoprostol 50 UgDocument6 pagesComparison Between Vaginal and Sublingual Misoprostol 50 Ugidris setyadi lubisNo ratings yet
- A Study Comparing Vaginal Misoprostol Alone With VDocument4 pagesA Study Comparing Vaginal Misoprostol Alone With VKamal AnshariNo ratings yet
- 2 Kata Pengantar HiDocument5 pages2 Kata Pengantar Hiaryo aryoNo ratings yet
- Randomized Clinical Trial Between Hourly Titrated Oral Misoprostol and Vaginal Dinoprostone For Induction of LaborDocument6 pagesRandomized Clinical Trial Between Hourly Titrated Oral Misoprostol and Vaginal Dinoprostone For Induction of LabormerawatidyahsepitaNo ratings yet
- Safety and Efficacy of Misoprostol in Induction of Labour in Prelabour Rupture of Fetal Membrane in Nigerian Women: A Multicenter StudyDocument6 pagesSafety and Efficacy of Misoprostol in Induction of Labour in Prelabour Rupture of Fetal Membrane in Nigerian Women: A Multicenter StudyAnonymous GssdN5No ratings yet
- W 3 e WDDocument6 pagesW 3 e WDsupaidi97No ratings yet
- Comparison of Two DosesDocument7 pagesComparison of Two DosesFelix BoamahNo ratings yet
- Oral or Vaginal Misoprostol For Labor Induction and Cesarean Delivery Risk: A Cohort StudyDocument19 pagesOral or Vaginal Misoprostol For Labor Induction and Cesarean Delivery Risk: A Cohort StudyDoniNo ratings yet
- Ijpr 13 299Document6 pagesIjpr 13 299Iene Dhiitta PramudNo ratings yet
- ComparisonDocument7 pagesComparisonpurnoor abidNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument3 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyFahmi Nur SuwandiNo ratings yet
- MisoprostolDocument6 pagesMisoprostolMaría PradoNo ratings yet
- International Journal of Gynecology and ObstetricsDocument6 pagesInternational Journal of Gynecology and ObstetricsmerawatidyahsepitaNo ratings yet
- Deh 001Document4 pagesDeh 001syid rosyidNo ratings yet
- Cervical RipeningDocument7 pagesCervical RipeningBagus WicaksonoNo ratings yet
- Chen 2015Document9 pagesChen 2015noor hyNo ratings yet
- A Randomized Trial of Synthetic Osmotic Cervical D - 2022 - American Journal ofDocument20 pagesA Randomized Trial of Synthetic Osmotic Cervical D - 2022 - American Journal ofLuis GómezNo ratings yet
- The Windmill Technique Avoids Manual Removal of The RetainedDocument6 pagesThe Windmill Technique Avoids Manual Removal of The RetainedEndrianus Jaya PutraNo ratings yet
- 10.1111@jog.13193 2 PDFDocument5 pages10.1111@jog.13193 2 PDFgandongmiziNo ratings yet
- Profile of Induced Labour in Uncomplicated Pregnancies With Unfavourable Modifieds Bishop Score in A Tertiary Care CentreDocument8 pagesProfile of Induced Labour in Uncomplicated Pregnancies With Unfavourable Modifieds Bishop Score in A Tertiary Care CentreIJAR JOURNALNo ratings yet
- AsddsaDocument8 pagesAsddsaJody AndreanNo ratings yet
- Pi Is 0002937818302497Document8 pagesPi Is 0002937818302497Jody AndreanNo ratings yet
- Bishop Score and The Outcome of Labor Induction With MisoprostolDocument4 pagesBishop Score and The Outcome of Labor Induction With MisoprostolhasrikaNo ratings yet
- Treatment With Piroxicam Before Embryo Transfer Increases The Pregnancy Rate After in Vitro Fertilization and Embryo TransferDocument5 pagesTreatment With Piroxicam Before Embryo Transfer Increases The Pregnancy Rate After in Vitro Fertilization and Embryo TransferVasantham HospitalNo ratings yet
- Induction of Labor With Misoprostol For Premature Rupture of Membranes Beyond Thirty-Six Weeks' GestationDocument6 pagesInduction of Labor With Misoprostol For Premature Rupture of Membranes Beyond Thirty-Six Weeks' GestationFebrinata MahadikaNo ratings yet
- Comparison of Nifedipine and Bed Rest For Inhibiting Threatened Preterm Labour 2161 0932.1000131Document4 pagesComparison of Nifedipine and Bed Rest For Inhibiting Threatened Preterm Labour 2161 0932.1000131muhammad maadaNo ratings yet
- MisoprostolDocument6 pagesMisoprostolmichelle1945No ratings yet
- The Efficacy of Misoprostol Vaginal Insert Compared With Oral Misoprostol in The Induction of Labor of Nulliparous Women A Randomized National Multicenter TrialDocument15 pagesThe Efficacy of Misoprostol Vaginal Insert Compared With Oral Misoprostol in The Induction of Labor of Nulliparous Women A Randomized National Multicenter TrialdindacNo ratings yet
- Marconi 2008Document6 pagesMarconi 2008Sri HariNo ratings yet
- Ijrcog-10870 OraDocument7 pagesIjrcog-10870 OraDr Chitikala HarithaNo ratings yet
- Anatomic Outcomes After Pelvic Organ Prolapse Surgery Comparing Uterine Preservation With HysterectomyDocument4 pagesAnatomic Outcomes After Pelvic Organ Prolapse Surgery Comparing Uterine Preservation With HysterectomyResidentes GinecologíaNo ratings yet
- MisoprostolDocument6 pagesMisoprostolJuan Aarón Rodríguez CarbonellNo ratings yet
- Comparison of Misoprostol and Manual Vacuum Aspiration For The Treatment of Incomplete AbortionDocument5 pagesComparison of Misoprostol and Manual Vacuum Aspiration For The Treatment of Incomplete AbortionShofi Dhia AiniNo ratings yet
- Prom PDFDocument6 pagesProm PDFaninditautNo ratings yet
- Clinical Uses of Misoprostol in Obstetrics and Gynaecology: MedicalDocument4 pagesClinical Uses of Misoprostol in Obstetrics and Gynaecology: MedicalRobertus HajaiNo ratings yet
- Slide Teknik Inseminasi Intrauterine-Dr. Hilma-FinalDocument44 pagesSlide Teknik Inseminasi Intrauterine-Dr. Hilma-FinalHalim Fertility CenterNo ratings yet
- AmniosDocument15 pagesAmniosneko niNo ratings yet
- Supported By: None.: AbstractsDocument1 pageSupported By: None.: AbstractsFerry DimyatiNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument5 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyAndrea LiraNo ratings yet
- Ijgo 12998Document7 pagesIjgo 12998el_dani_ellNo ratings yet
- Ultrasound in Obstet Gyne - 2021 - Fernlund - Reproductive Outcome After Early Miscarriage Comparing Vaginal MisoprostolDocument7 pagesUltrasound in Obstet Gyne - 2021 - Fernlund - Reproductive Outcome After Early Miscarriage Comparing Vaginal MisoprostolPutu Gede WidyatamaNo ratings yet
- Acupuncture and Acupressure in LaborDocument5 pagesAcupuncture and Acupressure in LaborAstri YuliandiniNo ratings yet
- The Effect of Hyoscine Butylbromide On The First Stage of Labour in Term PregnanciesDocument5 pagesThe Effect of Hyoscine Butylbromide On The First Stage of Labour in Term PregnanciesnephylymNo ratings yet
- Made Ayu AsnggrainiDocument5 pagesMade Ayu AsnggrainiMoh RamliNo ratings yet
- FinleyDocument1 pageFinleyDedi SaputraNo ratings yet
- Mullin 2002Document6 pagesMullin 2002Khairun NisaNo ratings yet
- Vaginal Touch Versus Transvaginal Ultrasound in The Management of Threatened Preterm Labour at The University Hospital Center of Porto-Novo (Benin)Document9 pagesVaginal Touch Versus Transvaginal Ultrasound in The Management of Threatened Preterm Labour at The University Hospital Center of Porto-Novo (Benin)Bayu Diesfa PuteraNo ratings yet
- Misoprostol SL Vs VAGDocument5 pagesMisoprostol SL Vs VAGAgus WijayaNo ratings yet
- Treatment Strategy for Unexplained Infertility and Recurrent MiscarriageFrom EverandTreatment Strategy for Unexplained Infertility and Recurrent MiscarriageKeiji KurodaNo ratings yet
- Lower Genital Tract Precancer: Colposcopy, Pathology and TreatmentFrom EverandLower Genital Tract Precancer: Colposcopy, Pathology and TreatmentNo ratings yet
- Absolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationFrom EverandAbsolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationNo ratings yet
- Mca 1 Sem Mathematical Foundation of Computer Science Ca 102 2013 14Document4 pagesMca 1 Sem Mathematical Foundation of Computer Science Ca 102 2013 14manish agrawalNo ratings yet
- MH Board Class 10 Hindi Composite N 324 2020 PDFDocument8 pagesMH Board Class 10 Hindi Composite N 324 2020 PDFmanish agrawalNo ratings yet
- MH Board Class 10 Marathi Composite N 314 2020 PDFDocument15 pagesMH Board Class 10 Marathi Composite N 314 2020 PDFmanish agrawalNo ratings yet
- Sweety Pediatric PDFDocument4 pagesSweety Pediatric PDFmanish agrawalNo ratings yet
- Mca 2 Sem Data Structure Using C Nmca 213 2014 15Document6 pagesMca 2 Sem Data Structure Using C Nmca 213 2014 15manish agrawalNo ratings yet
- Barch 1 Sem Architectural Communication Skills 1 1015006 Summer 2016Document2 pagesBarch 1 Sem Architectural Communication Skills 1 1015006 Summer 2016manish agrawalNo ratings yet
- Case Report Article: A Rare Site For Primary Tuberculosis - TonsilsDocument3 pagesCase Report Article: A Rare Site For Primary Tuberculosis - Tonsilsmanish agrawalNo ratings yet
- Parita Patel - PSM PDFDocument6 pagesParita Patel - PSM PDFmanish agrawalNo ratings yet
- Comparative Study of Two Topical Therapies in Acne - Benzoyl Peroxide (2.5%) & Retinoic Acid (0.025%)Document4 pagesComparative Study of Two Topical Therapies in Acne - Benzoyl Peroxide (2.5%) & Retinoic Acid (0.025%)manish agrawalNo ratings yet
- Neha CR Patho PDFDocument3 pagesNeha CR Patho PDFmanish agrawalNo ratings yet
- Dr.R.M.L.S.College, MuzaffarpurDocument5 pagesDr.R.M.L.S.College, MuzaffarpurabhaybittuNo ratings yet
- QATAR: Major ChangesDocument11 pagesQATAR: Major ChangesVivekanandNo ratings yet
- Supreme Court Quarterly Digest - Constitution of India (Jan-Mar, 2024)Document17 pagesSupreme Court Quarterly Digest - Constitution of India (Jan-Mar, 2024)muhammed iqbalNo ratings yet
- Intertechnique: Within The Quality Aerospace EnvironmentDocument32 pagesIntertechnique: Within The Quality Aerospace EnvironmentwonchoiNo ratings yet
- Legal Terminology - Ders 1Document27 pagesLegal Terminology - Ders 1simberkis12No ratings yet
- Luke Gromen Slide Deck For Parts 3 and 4Document47 pagesLuke Gromen Slide Deck For Parts 3 and 4riazuddin1985No ratings yet
- Cloud Storage Limit Monitoring MeasuresDocument3 pagesCloud Storage Limit Monitoring MeasuresesatjournalsNo ratings yet
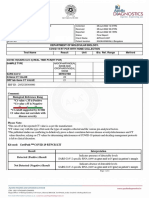
- Department of Molecular Biology. Covid 19 RT PCR With Home Collection Test Name Result Unit Bio. Ref. Range MethodDocument4 pagesDepartment of Molecular Biology. Covid 19 RT PCR With Home Collection Test Name Result Unit Bio. Ref. Range MethodnikhilaNo ratings yet
- Aspire Issue 6Document41 pagesAspire Issue 6HelenNo ratings yet
- Primary / Admin Entrance: Zone-B Zone-ADocument1 pagePrimary / Admin Entrance: Zone-B Zone-AMohammed AzharNo ratings yet
- Paul Andrew Mitchell Criminal ComplaiantDocument10 pagesPaul Andrew Mitchell Criminal Complaiantremenant2006No ratings yet
- Accreditaion of Hotel and Other - Related EstablishmentsDocument17 pagesAccreditaion of Hotel and Other - Related EstablishmentsAngelica Talandron100% (1)
- Vedant BaseDocument6 pagesVedant BasePanda ponnuNo ratings yet
- Disha 1000 Mcq-Pages EconomicsDocument76 pagesDisha 1000 Mcq-Pages EconomicsHarshit AroraNo ratings yet
- Curnon Bai Thuyet Trinh Giua KyDocument29 pagesCurnon Bai Thuyet Trinh Giua Ky22004079No ratings yet
- CVHimanshu MishraDocument8 pagesCVHimanshu Mishrak1969No ratings yet
- Wealth InequalityDocument35 pagesWealth Inequalityahmad100% (1)
- 08 - Chapter 2 PDFDocument21 pages08 - Chapter 2 PDFSaumya RanjanNo ratings yet
- Memo in Opposition To Defendants Motions For Attorneys FeesDocument4 pagesMemo in Opposition To Defendants Motions For Attorneys FeesJohn Carroll0% (1)
- Eng CH 1,2Document3 pagesEng CH 1,2hahirwar35No ratings yet
- Revised E-Tickets With Seat NumberDocument1 pageRevised E-Tickets With Seat NumberMohiminul KhanNo ratings yet
- 2022 - Year in ReviewDocument5 pages2022 - Year in ReviewRgvcfh HdggNo ratings yet
- MOL Pakistan - CORA DirectorateDocument18 pagesMOL Pakistan - CORA DirectorateAsad IrfanNo ratings yet
- A Political History of The Kingdom of Kazembe (Zambia) : Giacomo MacolaDocument256 pagesA Political History of The Kingdom of Kazembe (Zambia) : Giacomo Macolatemborhodah45No ratings yet
- This List Is For Officially Announced Partnerships, Collaberation, and Usage of Chainlink But It Is Not Maintained by The Team ItselfDocument3 pagesThis List Is For Officially Announced Partnerships, Collaberation, and Usage of Chainlink But It Is Not Maintained by The Team Itselfjustjack justjackNo ratings yet
- Cost and Management AccountingDocument296 pagesCost and Management Accountingatsamdam8781No ratings yet
- Lord Mcdonald by Eamonn SweeneyDocument6 pagesLord Mcdonald by Eamonn Sweeneyarrre weqweNo ratings yet
- PDFDocument6 pagesPDFHarshada AhirraoNo ratings yet
- Gregorio Araneta Vs RodasDocument2 pagesGregorio Araneta Vs RodasLeomar Despi LadongaNo ratings yet
- Mulund College of CommerceDocument20 pagesMulund College of CommerceAashay DagdeNo ratings yet