Download as pdf or txt
You might also like
- Respiratory Infections 1Document62 pagesRespiratory Infections 1Eduardo Valdez RodríguezNo ratings yet
- Pneumonia: Neonates To AdolescentsDocument32 pagesPneumonia: Neonates To AdolescentsAthenaTudino100% (2)
- Health and Hygiene in IndiaDocument25 pagesHealth and Hygiene in IndiaSOHEL BANGINo ratings yet
- Bronchiolitis: Ms AnamDocument56 pagesBronchiolitis: Ms AnamdmaulidaNo ratings yet
- Pneumonia Seminar HKNDocument66 pagesPneumonia Seminar HKNMahendra Yogi SemaraNo ratings yet
- Bro NK Ho PneumoniaDocument35 pagesBro NK Ho PneumoniaDewi AgustiniNo ratings yet
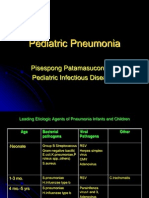
- Pediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesDocument39 pagesPediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesSi PuputNo ratings yet
- Presenter: clerk 2 蘇雋淋 Date: 2022/03/11Document39 pagesPresenter: clerk 2 蘇雋淋 Date: 2022/03/11s0501120醫學系No ratings yet
- Pneumonia - Dr. IonescuDocument51 pagesPneumonia - Dr. IonescuArleen MatincaNo ratings yet
- Neumonías 2008Document62 pagesNeumonías 2008Lucero BautistaNo ratings yet
- Patho Lect - An Overview of Bacterial and Viral Infections 3-03-2015Document36 pagesPatho Lect - An Overview of Bacterial and Viral Infections 3-03-2015Taimoor Ul HassanNo ratings yet
- Espiratory Infections BitseatDocument90 pagesEspiratory Infections BitseatAhmed KitawNo ratings yet
- Hand-Foot-And - Mouth DiseaseDocument27 pagesHand-Foot-And - Mouth DiseaseNur IzzahNo ratings yet
- Infeksi Saluran Pernafasan AtasDocument51 pagesInfeksi Saluran Pernafasan AtasreshaNo ratings yet
- Blok 27 PertussisDocument36 pagesBlok 27 PertussisNiaaAprilita100% (1)
- Pediatric NotesDocument61 pagesPediatric NotesMatusala BafaNo ratings yet
- IDAI Online Nov2021-FinalDocument46 pagesIDAI Online Nov2021-FinalEny HardiyantiNo ratings yet
- Acute Respiratory Infections: Dr. Ms Anam, Msi - Med, SpaDocument43 pagesAcute Respiratory Infections: Dr. Ms Anam, Msi - Med, SpaAgiana PratamaNo ratings yet
- Acute Respiratory Infections: Pneumonia Bronkiolitis Bronkitis AkutDocument60 pagesAcute Respiratory Infections: Pneumonia Bronkiolitis Bronkitis AkutIrfanNo ratings yet
- Upper Respıratory Tract InfectıonsDocument68 pagesUpper Respıratory Tract InfectıonsMekdes ZewdeNo ratings yet
- Topic 2. Dyspnea. Complecated Pneumonia in Children. - ShortDocument69 pagesTopic 2. Dyspnea. Complecated Pneumonia in Children. - ShortIbtissame BadadNo ratings yet
- PediatricsDocument312 pagesPediatricsمحمد ابو مناضل الافينش100% (1)
- Pedi Respir... DR - BrukDocument81 pagesPedi Respir... DR - BrukMatusala BafaNo ratings yet
- ASOMDocument41 pagesASOMArunkumar S KumarNo ratings yet
- ParamyxoviridaeDocument27 pagesParamyxoviridaeFarrah BenoitNo ratings yet
- Pneumonia 1Document40 pagesPneumonia 1Ahsan AuliyaNo ratings yet
- Viral Infection of The Respiratory TractDocument29 pagesViral Infection of The Respiratory TractPritha BhuwapaksophonNo ratings yet
- ParamyxovirusesDocument36 pagesParamyxovirusesRandy BerryNo ratings yet
- PneumoniaDocument66 pagesPneumoniaumanantini06100% (1)
- Fiebre Sin Foco Aparente 3 A 36 Meses DynaMedDocument41 pagesFiebre Sin Foco Aparente 3 A 36 Meses DynaMedAna Maria Guerron CabreraNo ratings yet
- PneumoniaDocument86 pagesPneumoniakhushisinghal.cse22No ratings yet
- Pneumococcal Disease and Pneumococcal VaccinesDocument31 pagesPneumococcal Disease and Pneumococcal VaccinesKartika RezkyNo ratings yet
- Pneumonia DR M ManiDocument69 pagesPneumonia DR M ManimaniNo ratings yet
- L - 2 - GR (-) CocciDocument82 pagesL - 2 - GR (-) CocciFahim NadvyNo ratings yet
- 3 Infeksi Saluran Pernafasan Akut (ISPA) PediatricsDocument35 pages3 Infeksi Saluran Pernafasan Akut (ISPA) PediatricsCharisma Tiara RessyaNo ratings yet
- The Child With Problems Related To The Transfer of Oxygen and NutrientsDocument200 pagesThe Child With Problems Related To The Transfer of Oxygen and NutrientsKarolien Faye DongaNo ratings yet
- PI Virus (Enterovirus and Rhinovirus Groups)Document34 pagesPI Virus (Enterovirus and Rhinovirus Groups)Lovryan Tadena AmilingNo ratings yet
- Common Childhood Infections For CIDocument89 pagesCommon Childhood Infections For CIBeamlak Getachew WoldeselassieNo ratings yet
- The Child With Problems Related To The Transfer of Oxygen and NutrientsDocument200 pagesThe Child With Problems Related To The Transfer of Oxygen and NutrientsKarolien Faye DongaNo ratings yet
- Pneumonia: H. Ridwan M. Daulay Wisman Dalimunthe Rini S. DaulayDocument49 pagesPneumonia: H. Ridwan M. Daulay Wisman Dalimunthe Rini S. DaulayKhairani PutriNo ratings yet
- Pneumonia and BronchiolitisDocument48 pagesPneumonia and Bronchiolitisshashank panwarNo ratings yet
- 3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualDocument28 pages3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualjimmyneumologiaNo ratings yet
- Ari P - Streptococcus Pneumoniae (Pneumococcal) Infection - 23 Nov 2023 - EnglishDocument27 pagesAri P - Streptococcus Pneumoniae (Pneumococcal) Infection - 23 Nov 2023 - Englishrosmadamanik2904No ratings yet
- CROUPDocument26 pagesCROUPRahul MehtaNo ratings yet
- Acute Respiratory Infections: PneumoniaDocument31 pagesAcute Respiratory Infections: PneumoniaAndy KumaraNo ratings yet
- LimfadenitisDocument24 pagesLimfadenitisrahmah ningsihNo ratings yet
- Respiratory Tract Infections 2022Document36 pagesRespiratory Tract Infections 2022m-9904772No ratings yet
- Pneumonia Pada Kasus PediatrikDocument41 pagesPneumonia Pada Kasus PediatrikasriNo ratings yet
- K.3 Pediatri-Virologi 3 2018-2019 PDFDocument76 pagesK.3 Pediatri-Virologi 3 2018-2019 PDFandi firdha restuwatiNo ratings yet
- Neonatal Sepsis-1Document35 pagesNeonatal Sepsis-1Mutai KiprotichNo ratings yet
- Pneumonia Pada Anak Di Era Pandemi COVID-19Document34 pagesPneumonia Pada Anak Di Era Pandemi COVID-19Hudania AddinaNo ratings yet
- Lec No (4) - Viral Respiratory Tract InfectionsDocument60 pagesLec No (4) - Viral Respiratory Tract InfectionsMohammedu IhthishamNo ratings yet
- Seminar On MumpsDocument40 pagesSeminar On Mumpssushmitabiswas052No ratings yet
- MENINGITIS DR Syad Akram Ali 01-12-2014Document95 pagesMENINGITIS DR Syad Akram Ali 01-12-2014Gopireddy Sivakarthik ReddyNo ratings yet
- Malarial Parasitaemia in Febrile Children With Sickle Cell AnaemiaDocument3 pagesMalarial Parasitaemia in Febrile Children With Sickle Cell AnaemiaAnn Irene DomnicNo ratings yet
- Pneumonii Acute Si Cronice La CopilDocument123 pagesPneumonii Acute Si Cronice La CopilAlexandra CristeaNo ratings yet
- Common Cold: Milan Karki 4062Document20 pagesCommon Cold: Milan Karki 4062BinayaNo ratings yet
- Surgical Pathology Unknown Case Conference 3/26/07Document22 pagesSurgical Pathology Unknown Case Conference 3/26/07Asmara SyedNo ratings yet
- Clinically Relevant Mycoses: A Practical ApproachFrom EverandClinically Relevant Mycoses: A Practical ApproachElisabeth PresterlNo ratings yet
- Water MetabolismDocument13 pagesWater MetabolismarmyNo ratings yet
- IATA Guidance On Managing Medical EventsDocument36 pagesIATA Guidance On Managing Medical EventsShinta Frennand100% (1)
- Narrative TextDocument19 pagesNarrative Textnafa nabillaNo ratings yet
- Grade VIII Biology Synopsis Theme 4: Unit 1 Name of The Chapter: Human Body-Endocrine System Date: 20-10-2021 No. of Pages: 6Document6 pagesGrade VIII Biology Synopsis Theme 4: Unit 1 Name of The Chapter: Human Body-Endocrine System Date: 20-10-2021 No. of Pages: 6shashwatthegamerytNo ratings yet
- Mudra Yoga Tips - SaiDocument8 pagesMudra Yoga Tips - SaidwhraghavNo ratings yet
- Research Articles ListDocument135 pagesResearch Articles Listnaga chaitanyaNo ratings yet
- Fibromyalgia and Chronic Fatigue Syndrome - Seven Proven Steps To Less Pain and More EnergyDocument196 pagesFibromyalgia and Chronic Fatigue Syndrome - Seven Proven Steps To Less Pain and More EnergyLyssa Jada-Marie CarterNo ratings yet
- Method of Triangles PreviewDocument30 pagesMethod of Triangles PreviewNidheesh RadhakrishnanNo ratings yet
- Obesity and Overweight: Key FactsDocument4 pagesObesity and Overweight: Key FactsAmandaNo ratings yet
- Holy Basil: Cabangbang, Mathews H. BSHM 2BDocument3 pagesHoly Basil: Cabangbang, Mathews H. BSHM 2BAlexis A. AguilarNo ratings yet
- Soal Persiapan Ulangan Bersama Semester 2 Kelas Xi 2021Document7 pagesSoal Persiapan Ulangan Bersama Semester 2 Kelas Xi 2021Fauzan NaufalNo ratings yet
- Yoga Asana With Benefits and Condtraidiction PDFDocument9 pagesYoga Asana With Benefits and Condtraidiction PDFAanchal SinghNo ratings yet
- Lesson Plan On Croups DiseaseDocument6 pagesLesson Plan On Croups DiseasechinchuNo ratings yet
- Textbook of Critical Care 7Th Edition Jean Louis Vincent Full ChapterDocument67 pagesTextbook of Critical Care 7Th Edition Jean Louis Vincent Full Chapterlorraine.thomason463100% (11)
- Weekly TipsDocument69 pagesWeekly TipsSharynn Kew Moore100% (1)
- Analytical ExpositionDocument16 pagesAnalytical ExpositionHuru JatiNo ratings yet
- TCM DiagnosisDocument7 pagesTCM DiagnosisravenadlerNo ratings yet
- CP 4Document79 pagesCP 4Kalichandren ArumugamNo ratings yet
- Billiary SystemDocument60 pagesBilliary SystemDONALD UNASHENo ratings yet
- RabipurDocument3 pagesRabipurDon DavidNo ratings yet
- Skill Lab Ebm TaryDocument15 pagesSkill Lab Ebm TarykemastasrifNo ratings yet
- Kode Icd 10 Tersering Di Poliklinik Obstetri Dan Ginekologi - EditDocument5 pagesKode Icd 10 Tersering Di Poliklinik Obstetri Dan Ginekologi - EditNur Rohmah Arsyad100% (1)
- KNGF Guideline For Physical Therapy Cardiac Rehabilitation FlowchartDocument3 pagesKNGF Guideline For Physical Therapy Cardiac Rehabilitation FlowchartXulkanain ZENo ratings yet
- PRE MS N2016 Ans KeyDocument33 pagesPRE MS N2016 Ans Keyaaron tabernaNo ratings yet
- The Concept of Powerlessness in Patient Treatment Nursing EssayDocument38 pagesThe Concept of Powerlessness in Patient Treatment Nursing EssayreginesulibNo ratings yet
- (DERMA) Therapeutic Conference - Antifungal 07-07-20Document89 pages(DERMA) Therapeutic Conference - Antifungal 07-07-20Jolaine ValloNo ratings yet
- Glipizide Patient HandoutDocument3 pagesGlipizide Patient HandoutsilvanaanggraeniNo ratings yet
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDocument37 pagesPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralNo ratings yet
- What Is Sport InjuryDocument6 pagesWhat Is Sport Injuryjuanito1979No ratings yet