Download as docx, pdf, or txt
You might also like
- Personal Development Module 7Document51 pagesPersonal Development Module 7Allinatsoc Reverof Nylia75% (4)
- Teaching Students With AdhdDocument60 pagesTeaching Students With AdhdDelia Popa100% (1)
- Edn449 Assignment 2Document12 pagesEdn449 Assignment 2api-294965415No ratings yet
- 2022-2023 MFA in Screenwriting Read All Instructions Carefully Before Completing The ApplicationDocument8 pages2022-2023 MFA in Screenwriting Read All Instructions Carefully Before Completing The ApplicationISABELLANo ratings yet
- Cara Weber PLPDocument4 pagesCara Weber PLPapi-721974344No ratings yet
- Flores Huaman ElenaDocument92 pagesFlores Huaman Elenamarikita89674No ratings yet
- Team Leaders Master ListDocument2 pagesTeam Leaders Master ListininzisNo ratings yet
- Salome Mwashiuya ProposalDocument39 pagesSalome Mwashiuya ProposalHerryNo ratings yet
- Revision III PortionDocument3 pagesRevision III Portionraghupredator2No ratings yet
- RM 1Document2 pagesRM 1SuriNo ratings yet
- OcoyDocument8 pagesOcoyTeni MariamNo ratings yet
- Worldbuilding Workbook (Form Fillable)Document14 pagesWorldbuilding Workbook (Form Fillable)Peter LührsNo ratings yet
- 2024 Triton High School PLP 3Document4 pages2024 Triton High School PLP 3api-723092404No ratings yet
- Soalan Kuiz - Bab 3 t2Document15 pagesSoalan Kuiz - Bab 3 t2emmylineNo ratings yet
- The Surrepetious Story of Young Breastfeeding Mother Some Stoy To Tell.Document79 pagesThe Surrepetious Story of Young Breastfeeding Mother Some Stoy To Tell.Andro Cabatuan InesNo ratings yet
- ClassXIICOMMERCE SepHYDocument3 pagesClassXIICOMMERCE SepHYParth BeriNo ratings yet
- 1Document22 pages1musaweraghani25No ratings yet
- Asuncion, Dennis M. Copy 1Document4 pagesAsuncion, Dennis M. Copy 1Allan IgbuhayNo ratings yet
- Chem 0293 SyllabusDocument3 pagesChem 0293 Syllabusabens01No ratings yet
- Thesis - Differential Predictors of Subjective Well-Being in A Latino Clinical SampleDocument209 pagesThesis - Differential Predictors of Subjective Well-Being in A Latino Clinical SampleGeorges El NajjarNo ratings yet
- Case Study On C Section Placenta Previa. B2 A 2Document46 pagesCase Study On C Section Placenta Previa. B2 A 2Hanna CarsanoNo ratings yet
- Startrek Character AntonaDocument1 pageStartrek Character AntonaNope ThanksNo ratings yet
- First BookDocument209 pagesFirst BookshekharavacNo ratings yet
- My PLPDocument4 pagesMy PLPapi-721686634No ratings yet
- Rita MMSEDocument20 pagesRita MMSEMostafa ShabanNo ratings yet
- Fundamentals of NursingDocument4 pagesFundamentals of NursingMaricel DuposNo ratings yet
- Student Scorecard Personal Learning Plan: Goals + InterestsDocument4 pagesStudent Scorecard Personal Learning Plan: Goals + Interestsapi-722202233No ratings yet
- Theories of Personality The Board Exam MonitoringDocument6 pagesTheories of Personality The Board Exam MonitoringRhalfNo ratings yet
- Godavari College of Nursing, Jalgaon.: Second Year Basic B.SC., NursingDocument1 pageGodavari College of Nursing, Jalgaon.: Second Year Basic B.SC., NursingshivaNo ratings yet
- Generic Clinical Checklist Area - Labour & DeliveryDocument4 pagesGeneric Clinical Checklist Area - Labour & DeliveryStanley SelvanathanNo ratings yet
- Dr. Amrita Aggarwal 1Document93 pagesDr. Amrita Aggarwal 1Pujal NayakNo ratings yet
- Final Grid Bsn-Curriculum Credit 050120Document1 pageFinal Grid Bsn-Curriculum Credit 050120dperezmorgado1No ratings yet
- Revision Ii PortionDocument2 pagesRevision Ii Portionraghupredator2No ratings yet
- Philosophy of Hospita L 2003Document26 pagesPhilosophy of Hospita L 2003Tanu GulatiNo ratings yet
- HASNAIN Preliminary PagesDocument8 pagesHASNAIN Preliminary PagesAgha HasnainNo ratings yet
- Awareness On The Effects of Cellphone Utilization To Students of Pangasinan State University San Carlos CampusDocument5 pagesAwareness On The Effects of Cellphone Utilization To Students of Pangasinan State University San Carlos CampusSteaven Claude Mendoza Cansino-RovilosNo ratings yet
- 2016 Annual ReportDocument36 pages2016 Annual ReportCCHSNo ratings yet
- Type 2 Diabetes Mellitus IcsDocument35 pagesType 2 Diabetes Mellitus IcsAriane Gay DuranNo ratings yet
- Chapter 5 Microbial GrowthDocument18 pagesChapter 5 Microbial GrowthMohamidin MamalapatNo ratings yet
- Microbiology 18 Anaerobes Cultivationa and Identification 556-597Document42 pagesMicrobiology 18 Anaerobes Cultivationa and Identification 556-597JenNo ratings yet
- Phychology Cbcs Draft Syllabus PDFDocument50 pagesPhychology Cbcs Draft Syllabus PDFTithi PaulNo ratings yet
- Elyssa Robinson Triton High School PLP 1Document4 pagesElyssa Robinson Triton High School PLP 1api-721727120No ratings yet
- Gabriella Molina 2024 Triton High School PLP 1Document4 pagesGabriella Molina 2024 Triton High School PLP 1api-722202629No ratings yet
- Stroke Awareness Because It Matters - BI PRESENTATIONDocument7 pagesStroke Awareness Because It Matters - BI PRESENTATIONHabibNo ratings yet
- Communication Tool To Promote Antenatal Care, Skilled Delivery and Postnatal CareDocument32 pagesCommunication Tool To Promote Antenatal Care, Skilled Delivery and Postnatal CareNICHOLE MOJELLONo ratings yet
- ResearchDocument80 pagesResearchRamesh RamuNo ratings yet
- Diagnosis and Diagnostic Aids - Case History and Clinical ExaminationDocument203 pagesDiagnosis and Diagnostic Aids - Case History and Clinical ExaminationhaleenaNo ratings yet
- S2 Exam 4 MicrobioDocument6 pagesS2 Exam 4 MicrobioYosr FarzaNo ratings yet
- ThesisDocument67 pagesThesisAnas hussein BarafNo ratings yet
- Tenants' Level of Satisfaction Towards The Fire Safety Engineer of Mall of AsiaDocument45 pagesTenants' Level of Satisfaction Towards The Fire Safety Engineer of Mall of AsiaHenesy ValenciaNo ratings yet
- Ilovepdf MergedDocument77 pagesIlovepdf Mergedsyed NihalNo ratings yet
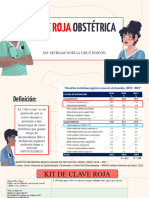
- Clave Roja - Im Myriam Noelia Cruz PoicónDocument29 pagesClave Roja - Im Myriam Noelia Cruz PoicónAle tcNo ratings yet
- Creation of A Flexible Class: Distance Offline Remote ModalityDocument3 pagesCreation of A Flexible Class: Distance Offline Remote ModalityEM BINo ratings yet
- Esgd 3Document279 pagesEsgd 3JOSHUA MEDRANONo ratings yet
- Revista 1Document262 pagesRevista 1Domenica ToalaNo ratings yet
- NauliDocument5 pagesNaulidorkasisimfukwe29No ratings yet
- Underground Drill ProfilingDocument21 pagesUnderground Drill ProfilingKennethSampaguitaDeLaRosaNo ratings yet
- Monograph of PsychometryDocument4 pagesMonograph of PsychometryLuis EsbaNo ratings yet
- Adult Emergency PDFDocument2 pagesAdult Emergency PDFVon HippoNo ratings yet
- FM TosDocument2 pagesFM TosAnees RahmanNo ratings yet
- On The Origins and Diagnosis of Asperger's Syndrome: A Clinical Neuroimaging and Genetic StudyDocument95 pagesOn The Origins and Diagnosis of Asperger's Syndrome: A Clinical Neuroimaging and Genetic StudydesbestNo ratings yet
- Non-Food Item Post-Distribution Monitoring ReportDocument14 pagesNon-Food Item Post-Distribution Monitoring ReportLGNo ratings yet
- Psychological Statistics and Research MethodsDocument198 pagesPsychological Statistics and Research MethodsNireesh Gopalakrishnan100% (3)
- Advanced Social Psychology PDFDocument238 pagesAdvanced Social Psychology PDFNireesh GopalakrishnanNo ratings yet
- ValmikiRamayanam Malayalam BalaKandam PDFDocument589 pagesValmikiRamayanam Malayalam BalaKandam PDFNireesh Gopalakrishnan100% (1)
- Cognitive Beahavioural TherapyDocument10 pagesCognitive Beahavioural TherapyNireesh GopalakrishnanNo ratings yet
- ValmikiRamayanam Malayalam BalaKandamDocument589 pagesValmikiRamayanam Malayalam BalaKandamNireesh Gopalakrishnan100% (2)
- Downloaded From PirateBB - Org - Business Materials & E-Learning Video Tutorials DownloadDocument1 pageDownloaded From PirateBB - Org - Business Materials & E-Learning Video Tutorials DownloadNireesh GopalakrishnanNo ratings yet
- Intermediate Iridology Course TranscriptionDocument52 pagesIntermediate Iridology Course TranscriptionNireesh Gopalakrishnan100% (1)
- Somatoform Disorder PDFDocument18 pagesSomatoform Disorder PDFAmit Tamboli100% (1)
- Iep Ben SDocument47 pagesIep Ben Sapi-269881639No ratings yet
- (Download PDF) Child and Adolescent Psychopathology For School Psychology 1St Edition Terry Diamanduros Full Chapter PDFDocument69 pages(Download PDF) Child and Adolescent Psychopathology For School Psychology 1St Edition Terry Diamanduros Full Chapter PDFdydtnszani100% (9)
- Typology of Learners With Special NeedsDocument10 pagesTypology of Learners With Special NeedsKaiden GaizerNo ratings yet
- 2004 - Hart - Opening The Contemplative Mind in The ClassroomDocument12 pages2004 - Hart - Opening The Contemplative Mind in The Classroometherealflames5228No ratings yet
- Rennie TerryJames PHD 2002Document408 pagesRennie TerryJames PHD 2002sumairaNo ratings yet
- 1 s2.0 S2451902222001471 MainDocument11 pages1 s2.0 S2451902222001471 MainAlejandro CabaNo ratings yet
- Attention-Deficit Hyperactivity Disorder Systematic Reviews Impulsivity AdhdDocument3 pagesAttention-Deficit Hyperactivity Disorder Systematic Reviews Impulsivity AdhdJhoo AngelNo ratings yet
- Seventh Grade Abiotic & Biotic FactorsDocument6 pagesSeventh Grade Abiotic & Biotic Factorsapi-285033858No ratings yet
- Dev Ped July Exam CorrectedDocument7 pagesDev Ped July Exam CorrectedbookwormMDNo ratings yet
- Factor Analysis of The CBQDocument4 pagesFactor Analysis of The CBQMamalikou MariaNo ratings yet
- AdhdDocument20 pagesAdhdAlexis FajardoNo ratings yet
- STANDocument62 pagesSTANErick HidayatNo ratings yet
- EXCELLEROLYMPICSDocument53 pagesEXCELLEROLYMPICSJoya Jimenea GenzolaNo ratings yet
- Adhd HandoutDocument2 pagesAdhd Handoutapi-294390786No ratings yet
- StoryboardDocument8 pagesStoryboardapi-291436352No ratings yet
- Early-Life Language Stimulation, Skills May Prevent Childhood Depression - Children With Language Deficits Are Significantly More Likely To Experience Depression by Third Grade - ScienceDailyDocument5 pagesEarly-Life Language Stimulation, Skills May Prevent Childhood Depression - Children With Language Deficits Are Significantly More Likely To Experience Depression by Third Grade - ScienceDailyPietro De SantisNo ratings yet
- Systematic Review and Meta-Analysis: The Science of Early-Life Precursors and Interventions For Attention-De Ficit/hyperactivity DisorderDocument40 pagesSystematic Review and Meta-Analysis: The Science of Early-Life Precursors and Interventions For Attention-De Ficit/hyperactivity DisorderAndana TrisaviNo ratings yet
- Diagnosis and Management of Learning Disabilities An Interdisciplinary Lifespan ApproachDocument244 pagesDiagnosis and Management of Learning Disabilities An Interdisciplinary Lifespan ApproachLilithNo ratings yet
- OPDocument15 pagesOPFernanda ClaudinoNo ratings yet
- Psychological Disorders Class 12 PDFDocument11 pagesPsychological Disorders Class 12 PDFsushil_bugalia7293No ratings yet
- EBD The Etiological Factors or Causes of EbdDocument1 pageEBD The Etiological Factors or Causes of EbdmootchabaaaNo ratings yet
- Hand Outs For Special EducationDocument27 pagesHand Outs For Special EducationArjay JacobNo ratings yet
- Understanding Conduct Disorder and Oppositional-Defiant Disorder: A Guide To Symptoms, Management and TreatmentDocument46 pagesUnderstanding Conduct Disorder and Oppositional-Defiant Disorder: A Guide To Symptoms, Management and TreatmentjojdoNo ratings yet
- Mutism SelectivDocument30 pagesMutism SelectivAurelia BartaNo ratings yet
- Apnea KidsDocument5 pagesApnea KidsVeenu KhubnaniNo ratings yet
- You Are The Perfect Parent: 9 Simple Guides For Filipino Parents With ADHD ChildDocument8 pagesYou Are The Perfect Parent: 9 Simple Guides For Filipino Parents With ADHD ChildOnah C ArnidoNo ratings yet