Professional Documents
Culture Documents
ACS - Clinical Review 2015
ACS - Clinical Review 2015
Uploaded by
Purwoko SugengOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
ACS - Clinical Review 2015
ACS - Clinical Review 2015
Uploaded by
Purwoko SugengCopyright:
Available Formats
evidence & practice / CPD / cardiology
ACUTE CORONARY SYNDROME
Acute coronary syndrome: assessment
and management
NS885 Norton C (2017) Acute coronary syndrome: assessment and management. Nursing Standard. 31, 29, 61-70.
Date of submission: 10 November 2016; date of acceptance: 16 December 2016. doi: 10.7748/ns.2017.e10754
Cormac Norton Abstract
Lecturer in clinical Acute coronary syndrome is a serious condition that requires urgent assessment and
simulation and clinical management. This article outlines the nature of the condition, and discusses its underlying
practice, School of Health pathophysiology. It discusses three types of acute coronary syndrome: unstable angina, ST
Professions, Murdoch elevation myocardial infarction and non-ST elevation myocardial infarction. Research and
University, Mandurah, guidelines are used to guide the reader through approaches to initial nursing assessment and
Australia the immediate management of patients with suspected acute coronary syndrome.
Correspondence Keywords
c.norton@murdoch. acute coronary syndrome, angina, cardiology, cardiovascular system, coronary heart disease,
edu.au myocardial infarction, myocardial ischaemia, stable angina, unstable angina
Conflict of interest
None declared Aims and intended learning This article relates to The Code in the
outcomes following ways:
Peer review The aim of this article is to discuss the »» The Code states that nurses must act
This article has been initial nursing assessment and management when an emergency arises in their practice
subject to external of patients presenting with suspected setting. Acute coronary syndrome is a
double-blind peer acute coronary syndrome. After reading medical emergency and nurses should be
review and checked this article and completing the time out equipped to undertake urgent assessment
for plagiarism using activities you should be able to: and management of patients.
automated software »» Describe normal coronary circulation »» Emergency care is constantly evolving,
and how it relates to the cardiovascular and nurses should be aware of up-to-date
Revalidation system. guidelines and research underpinning
Prepare for revalidation: »» Explain the pathophysiology related to their practice. This article provides
read this CPD article, acute coronary syndrome. evidence-based information about the
answer the questionnaire »» Identify the signs and symptoms of acute causes, assessment and management of
and write a reflective coronary syndrome, and differentiate acute coronary syndrome.
account: rcni.com/ between the various types of the condition. »» Nurses must recognise and respond
revalidation »» Discuss the initial nursing assessment to people’s physical, psychological
and management of patients presenting and social needs. This article provides
Online with suspected acute coronary syndrome. information about how nurses can
For related articles visit identify the symptoms of acute coronary
the archive and search Relevance to The Code syndrome, how to undertake a structured
using the keywords Nurses are encouraged to apply the nursing assessment for these patients,
four themes of The Code: Professional and appropriate treatment interventions.
Standards of Practice and Behaviour for »» Patients with suspected acute coronary
Nurses and Midwives to their professional syndrome and their families might be
practice (Nursing and Midwifery Council frightened and anxious. Nurses have a
(NMC) 2015). The themes are: Prioritise central role in supporting them through
people, Practise effectively, Preserve safety, this time, which is in accordance with
and Promote professionalism and trust. the theme to prioritise people.
nursingstandard.com volume 31 number 29 / 15 March 2017 / 61
evidence & practice / CPD / cardiology
To write a CPD article Introduction effects for patients. Short-term effects
Please email gwen. The incidence of acute coronary syndrome include a reduction in 30-day mortality
clarke@rcni.com. decreased between 2002 and 2016 in most following admission (Chung et al 2014),
Guidelines on writing for developed countries (Timmis 2015). Between while long-term effects include a reduction
publication are available 2002 and 2012, the rate of acute myocardial in the frequency of morbidities associated
at: journals.rcni.com/r/ infarctions decreased by 33% in men and with acute coronary syndrome, including
author-guidelines 31% in women in England (Smolina et al chronic heart failure (Cowie et al 2005).
2012). Despite this decrease, acute coronary
syndrome remains one of the leading causes TIME OUT 1
of premature death in the UK, and was Using an anatomy and physiology textbook such as
responsible for 16% of all deaths in men in that written by Tortora and Derrickson (2013), revise the
2012 (Bhatnagar et al 2015). This article primary function of the cardiovascular system and list
discusses three types of acute coronary the main components.
syndrome: unstable angina, ST elevation
myocardial infarction (STEMI) and non-ST Cardiovascular system
elevation myocardial infarction (NSTEMI). When considering disease processes, it might
Survival following acute coronary be useful to consider the ‘building blocks’
syndrome is linked to prompt assessment, of human life. The most basic structure
diagnosis and management (Timmis 2015). in the human body is the cell. For life to
Nurses have an important role in increasing exist, the cell must produce energy, and the
survival rates, because they are usually the substances required to produce energy must
first healthcare practitioners to come into be delivered to the cells of the body, and the
contact with the patient (Nikolaou et al waste products of energy removed.
2015). Nurses who are knowledgeable and The primary function of the
skilled are more likely to ensure that patients cardiovascular system is to deliver nutritive
presenting with signs and symptoms of acute substrates to cells, such as oxygen and
coronary syndrome are assessed and treated glucose, and to remove the waste products
promptly. of metabolism, such as carbon dioxide and
The complex nature of acute coronary water (Tortora and Derrickson 2013). The
syndrome can mean that classic signs of cardiovascular system comprises the heart,
acute myocardial injury, such as changes blood and blood vessels. This article focuses
in the ST segment on an electrocardiogram on the heart. The heart is responsible for
(ECG), might be absent. Evidence indicates pumping blood to cells and, in conjunction
that the incidence of acute coronary with blood vessels, producing the pressure
syndrome without classical ST segment necessary to perfuse the cells with the
elevation on an ECG is more frequent than nutrients they require (blood pressure).
the incidence of acute coronary syndrome Unless it is compensated for, a failure of
with ST segment elevation (Yeh et al 2010, the cardiovascular system will result in an
Roffi et al 2016). Nurses are increasingly interruption to the supply of nutrients to
likely to encounter such patients; therefore, cells, reducing aerobic respiration, affecting
it is essential that they understand the energy production and ultimately leading to
pathophysiology of the condition, and how cell death (Thiele et al 2015). If this adversely
the signs and symptoms might vary. affects one cell, it will have significant effects
The in-hospital mortality rate of patients on whole organs or body systems.
with STEMI is higher than the in-hospital Since this article focuses on acute
mortality rate of patients with NSTEMI; coronary syndrome, it is important to
however, the mortality rate in the six review what the heart requires to function
months following the event is similar normally. Coronary blood supply is the
(Fox at al 2006). This is significant for most significant factor in maintaining
nurses caring for patients with suspected normal cardiac function. The pumping
acute coronary syndrome, because initial motion of the heart is provided by cardiac
assessment and immediate management muscle (myocardium). The heart beats from
have significant short-term and long-term an early stage in embryonic development
62 / 15 March 2017 / volume 31 number 29 nursingstandard.com
For related CPD articles visit
evidenceandpractice.nursingstandard.com
until death. Myocardium requires constant for Health and Care Excellence (NICE)
perfusion with oxygen and nutrients to 2016).
function. To meet this need, the heart is Angina pectoris is the term for chest pain
supplied with a coronary blood supply. that is usually on exertion or at times of
No single organ other than the heart, stress. The pain is caused by ischaemia within
has such an adverse effect on the rest of the myocardium, resulting from inadequate
the body if it is compromised. Therefore, blood supply through the narrowed coronary
any disease process affecting the heart may arteries (Thiele et al 2015). When the patient
have a life-threatening effect. rests, the pain will usually resolve in less
than 15 minutes (NICE 2016). This is an
TIME OUT 2 important factor to consider when taking a
List three of the main coronary arteries and outline the patient history. Such angina is termed stable
areas of the heart they supply. angina, because the blood supply to the
myocardium meets demand soon after the
Coronary heart disease stressor, for example exercise, is removed.
Acute coronary syndrome is often a Chest pain that does not resolve with rest,
consequence of coronary heart disease, termed unstable angina, will be discussed
although in rare cases acute coronary later in this article.
syndrome may be attributed to other There are several risk factors that
causes, for example drug use. The most determine how likely an individual is to
common cause of acute coronary syndrome develop coronary heart disease. These risk
is atherosclerosis (Roffi et al 2016). factors may be divided into modifiable
Atherosclerosis is a process by which fatty and non-modifiable (Table 1). Many of
deposits (plaque) build up on the inner the modifiable risk factors in Table 1 can
(intimal) lining of arteries. In the coronary be reduced through changes in lifestyle.
arteries, this process gradually leads to Timmis (2015) observed that over the past
a narrowing in the lumen of the artery 50 years, reductions in death from coronary
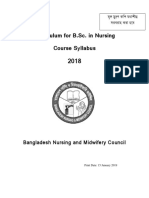
(Figure 1) (Nable and Braunwald 2012). heart disease can be attributed as much to
The needs of the myocardium change changes in lifestyle as to drug and surgical
depending on activity. For example, at rest interventions. From a nursing perspective,
the myocardium will have a relatively low this emphasises the importance of effective
demand for blood, whereas on exertion the health promotion at an appropriate time.
myocardium must contract faster to meet
the demands of skeletal muscle (Tortora Acute coronary syndrome
and Derrickson 2013). This rise in heart Acute coronary syndrome is a medical
rate increases the demand for oxygenated emergency in which blood supply to the
blood to the myocardium. Healthy myocardium has become partially or
coronary vessels will meet this demand completely occluded, most commonly
because blood is unrestricted. However,
coronary vessels that have developed
atheromatous plaque will have a reduced TABLE 1. Modifiable and non-modifiable risk factors for
capacity to carry blood. The increased coronary heart disease
demand will not be met, resulting in
ischaemia in the affected myocardial tissue. Modifiable risk factors Non-modifiable risk factors
Coronary heart disease might be non-
»» Diabetes »» Age
symptomatic in the early stages of the »» Diet (lack of fruit and vegetables) »» Ethnicity
disease. As the disease progresses, signs and »» Hypercholesterolaemia »» Gender
symptoms will develop. The most common »» Hypertension »» Genetic factors, for example family history
symptom the patient will experience is »» Lack of exercise in a first-degree relative at premature age
chest pain. Classically, this is described as a »» Obesity
tight band around the patient’s chest. The »» Smoking and alcohol use
patient may also experience discomfort in »» Stress
one arm or in the jaw (National Institute (Adapted from Perk et al 2012)
nursingstandard.com volume 31 number 29 / 15 March 2017 / 63
evidence & practice / CPD / cardiology
caused by a rupture of atheromatous plaque becomes necrotic, resulting in damage to
(Nikolaou et al 2015). The term ‘syndrome’ the myocardium (Thiele et al 2015).
is used because the signs and symptoms of For a myocardial infarction to be
the disease process are similar; however, diagnosed, specific criteria must be met, such
the specific disease process might differ. For as an increase or decrease in troponin levels,
example, acute myocardial infarction will and ST segment elevation on an ECG or one
have a different pathogenesis from unstable of the other criteria listed in Box 1 (Timmis
angina, but the effect on the myocardium 2015). It is possible for acute myocardial
will ultimately be the same if left untreated ischaemia to occur in the absence of ST
(Nikolaou et al 2015). segment change on an ECG, for example
Most nurses will be familiar with NSTEMI, or without complete occlusion of a
myocardial infarction – the death of coronary vessel (unstable angina). Therefore,
myocardium as a result of a complete while the signs and symptoms might be
occlusion of a coronary vessel. The identical, the exact cause of the ischaemia
occlusion occurs as result of rupture may differ.
of the atheromatous plaque, leading to
bleeding, which results in the formation TIME OUT 3
of a thrombus (Figure 1). The thrombus Describe how you would structure an initial assessment
lodges in the coronary vessel, occluding it. for a patient who is acutely unwell. Why have you used that
Myocardial tissue distal to the occlusion approach? What alternative approaches are available?
becomes ischaemic, and if left untreated
Initial nursing assessment
It is essential that all assessments are
Figure 1. Atherosclerosis and formation of a thrombus in a coronary artery
undertaken in a structured manner, to ensure
the information necessary to formulate an
appropriate plan of care is acquired. The
Direction of blood flow ABCDE (airway, breathing, circulation,
Red blood cells
disability, exposure) approach to initial
Normal artery assessment has been used in emergency
care settings for many years (Thim et al
2012). Using the ABCDE approach, the
practitioner assesses, identifies and resolves
life-threatening problems in a logical order;
Atherosclerosis
Atherosclerosis buildup for example, resolving an obstructed airway
takes priority over assessing the circulatory
system. This structured approach is efficient
and prevents deterioration in an emergency,
Formation of a thrombus where reaching a definitive diagnosis is often
difficult.
Atherosclerosis buildup with thrombus Patients with acute coronary syndrome
are likely to be acutely unwell, and the
ABCDE approach should be followed in
BOX 1. Criteria for the diagnosis of myocardial infarction the initial stages of care (Box 2). For the
purposes of the treatment and management
Rise or fall in troponin levels, with at least one value above the 99th percentile upper reference interventions discussed in this article, it will
limit, plus at least one of the following: be presumed that the patient is conscious
» Symptoms of ischaemia, for example chest pain and dyspnoea and has a patent airway.
» New ST segment elevation or T wave changes, or new bundle branch block on an
electrocardiogram (ECG)
» Pathological Q waves on an ECG
TIME OUT 4
» Imaging evidence of infarction Mark is a 56-year-old man who has been admitted to your
» Identification of an intracoronary thrombus by angiography or autopsy clinical setting, experiencing chest pain. As you take the
(Adapted from Thygesen et al 2012. ©European Society of Cardiology: tinyurl.com/ESC-myocardial) history, he states he is a secondary school teacher and
is married with three children. Mark says he smokes ten
64 / 15 March 2017 / volume 31 number 29 nursingstandard.com
For related CPD articles visit
evidenceandpractice.nursingstandard.com
cigarettes per day, but does not drink alcohol. He states that
Ischaemia in the myocardium can lead to life-
his father had a myocardial infarction when he was 44 years
old and died of a ‘heart attack’ aged 58 years. When asked
threatening arrhythmias (Zorzi et al 2016).
about his medication, Mark states he takes lisinopril 10mg Normal cardiac rhythm requires specific
once daily, and cannot recall why he takes the medication. concentrations of electrolytes within
List Mark’s risk factors for coronary heart disease and the myocardium. Ischaemia may affect these
indicate whether they are modifiable or non-modifiable. concentrations leading to arrhythmias, which
in some cases may lead to cardiac arrest.
Once immediate life-threatening problems
have been identified, it is important to TIME OUT 5
obtain a detailed history from the patient. Review your knowledge of a normal ECG. Draw the shape
This should include: (morphology) of a normal sinus rhythm. Referring to a
»» Description of the pain – how long since its 12-lead ECG, indicate the area of the heart that each of the
onset, and nature and location of the pain. following leads relates to: lead I, lead II, lead III, aVR, aVL,
»» Medical history. aVF, V1, V2, V3, V4, V5, V6.
»» Drug and medication history, including
smoking or alcohol intake. Table 2 shows the usual anatomical
»» Allergies. location of ECG leads for a normal 12-
»» Social and occupational history. lead ECG. Figure 2 shows the limb lead
The information provided enables the placement, and Figure 3 shows the chest
practitioner to develop an understanding lead placement in a normal 12-lead ECG.
of the patient’s risk factors, for example While cardiac monitors will display
smoking or a history of heart disease. arrhythmias, they are not effective in
Patients with acute coronary syndrome assessing the heart for abnormalities such
should be specifically assessed for (NICE as ischaemia, because they only display the
2016): electrical activity in one plane. Typically,
»» Pain in the chest and/or other areas, for in three-lead cardiac monitors this will be
example the arm, jaw, teeth or back, lead II, which shows electrical activity in
lasting longer than 15 minutes. the inferior surface of the myocardium. To
»» Chest pain with shortness of breath, record the electrical activity in all planes
nausea and vomiting, sweating or of the heart, a 12-lead ECG should be
abnormal blood pressure. recorded within ten minutes of the patient’s
»» Chest pain that is new to the patient, or arrival in the clinical setting (NICE 2016,
a worsening pattern of chest pain in the Roffi et al 2016).
patient with stable angina. This might Detailed analysis of ECGs requires skill
include increasing regularity of pain and knowledge and is beyond the scope
caused by minimal exertion. of this article. Figure 4 shows the normal
It is important to appreciate that some sinus rhythm complex. The most important
patients, such as those with diabetes ECG change that relates to acute coronary
mellitus, might not present with chest
pain (Timmis 2015, Roffi et al 2016). For
example, they may present to healthcare BOX 2. ABCDE approach to assessment of the patient with
services following a collapse or feeling acute coronary syndrome
unwell with nausea and vomiting. It is »» Airway: ensure the airway is patent
important to consider the risk factors for »» Breathing: assess the respiratory rate; oxygen saturation; depth and symmetry of chest
coronary heart disease (Table 1) when expansion
assessing this patient group. »» Circulation: assess the pulse for rate, rhythm and volume; blood pressure; capillary refill;
urine output; general colour; attach the patient to a cardiac monitor and perform a 12-lead
Cardiac monitoring electrocardiogram
Patients presenting with chest pain »» Disability: establish conscious level using either AVPU (alert, voice, pain, unresponsive) or
the Glasgow Coma Scale
should be attached to a cardiac monitor, with »» Exposure: record the temperature, observe the patient for any external abnormal signs, for
a defibrillator, as soon as possible (NICE example rashes or bruising
2016). Ideally this can be done during the ‘C’ (Adapted from Thim et al 2012)
(circulation) part of the ABCDE assessment.
nursingstandard.com volume 31 number 29 / 15 March 2017 / 65
evidence & practice / CPD / cardiology
syndrome is in the ST segment. The ST The abnormality shown demonstrates an
segment (Figure 4) reflects a period in anterior myocardial infarction that could not
which the ventricle has reached the end be seen on the three-lead cardiac monitor.
of its mechanical contraction, and where Where possible, it is recommended that a
the electrolytes responsible for causing the 12-lead ECG is performed in the pre-hospital
electrical activity are returning to their pre- setting (Nikolaou et al 2015). The ECG may
contraction state (repolarisation). Under be transmitted electronically to the receiving
normal conditions, the ST and T waves will medical facility for analysis by a senior
be in line with the P and QRS waves. This clinician, or presented on arrival with the
line is known as the isometric line (Booth patient. Evidence suggests that this enables
and O’Brien 2015). prompt diagnosis and treatment, resulting
Following an acute myocardial infarction, in lower overall rates of mortality following
blood supply to a proportion of the acute coronary syndrome (Quinn et al 2014).
myocardium is obstructed. This obstruction
affects the electrical activity in the area of Laboratory investigations
the heart. During the acute phase of the Injury to myocardial cells caused by
infarction, the time in which the S and occlusion of the coronary artery will be
T waves return to the isometric line are indicated in blood tests. Troponin is a protein
delayed, causing the ST segment to be found in myocardial tissue that is responsible
raised (Figure 5). This is termed ST segment for regulating myocardial contractility.
elevation; when this occurs on an ECG, the When myocardial cells become damaged,
patient is diagnosed with STEMI. While this troponin leaks into the surrounding blood.
is a classic sign of a myocardial infarction This increase of troponin levels in the blood
on an ECG, there are cases in which the ST
segment remains unaltered, is depressed,
Figure 2. Limb lead placement in a normal
or where the T wave changes shape, this is 12-lead electrocardiogram
termed NSTEMI (Booth and O’Brien 2015).
Failure to undertake a 12-lead ECG can
result in significant cardiac abnormalities
being missed. A cardiac monitor trace
may show normal sinus rhythm, with no
suggestion of ST elevation. However, a
12-lead ECG recording will show ST
elevation in leads V1, V2 and V3 (Figure 5).
TABLE 2. Usual anatomical location of electrocardiogram
(ECG) leads
ECG leads Relative location Coronary artery
V1, V2, V3, V4 Anterior Left anterior descending
V1, V2 Septal Left anterior descending
I, aVL, V5, V6 Left lateral Left circumflex
II, III, aVF Inferior Right coronary artery
aVR, V1 Right atrial Right coronary artery
Posterior chest lead Posterior Right coronary
placement*
*Leads may be placed in the posterior chest wall to help identify specific abnormalities
(Adapted from Booth and O’Brien 2015)
66 / 15 March 2017 / volume 31 number 29 nursingstandard.com
For related CPD articles visit
evidenceandpractice.nursingstandard.com
provides an indication of tissue damage. opiate-based analgesia, for example a history
The rise in troponin levels may not be of chronic obstructive pulmonary disease
evident for up to four hours following cell (COPD) or hypotension. Administering
injury (Roffi et al 2016). For that reason, glycerine trinitrate through either the buccal
guidelines recommend serial blood tests or sublingual route will cause vasodilation,
at zero, three and six hours following and may relieve chest pain for some patients.
the patient’s arrival in the clinical setting Evidence shows that a single dose of
(Nikolaou et al 2015). Where possible, aspirin 300mg enhances the benefits of any
blood samples should be taken and results reperfusion therapy the patient may receive
available within one hour of the patient’s (Nikalaou 2015), reducing mortality rates
arrival (Roffi et al 2016). The reliability in the 30 days following the event (Timmis
and validity of troponin results depend 2015). As with all medicines, the nurse
on the timing of the blood sample and should consider any contraindications,
the laboratory system used to analyse such as gastric ulceration. If there are
the sample (Shah et al 2015, Cullen et al contraindications to aspirin, clopidogrel
2016). From the nurse’s perspective, this is an effective alternative medicine (NICE
means having a clear understanding 2013).
of local policy about the timing of
appropriate blood tests and ensuring this Figure 3. Chest lead placement in a normal
is adhered to. 12-lead electrocardiogram
Immediate management
It is important to understand that the reason
the patient will have attended the clinical
setting is pain, or anxiety related to pain.
Nurses in the emergency care setting will
encounter patients who have life-threatening
conditions, with little or no warning. Patients V1 V2
may feel frightened and anxious during this V3
V4 V5 V6
time, so it is essential that nurses establish
trust, and provide clear communication
during the initial critical period of the
patient’s arrival to the clinical setting. Aside
from the human factors, anxiety increases
heart rate, thereby increasing myocardial
oxygen demand. When considering Figure 4. Normal sinus rhythm complex
the management of the patient, nurses
should be aware of their duty to act as Atria Ventricles
an advocate for the patient and engender 2
trust (NMC 2015). Patients experiencing RR interval
a life-threatening condition such as acute
coronary syndrome require compassion and R S-T
support with decision making. Therapeutic 1 segment
communication is essential and, where
necessary, nurses should have the courage
to challenge practice that may not be of a P T
sufficiently high standard. 0
The patient should be made as comfortable
as possible. Intravenous opiates are Q S
recommended as the first-line treatment Q-T interval
for chest pain (NICE 2016). As with all P-R interval = 0.16 sec
patients, consideration should be given to the –1
0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6
contraindications or cautions to the use of
nursingstandard.com volume 31 number 29 / 15 March 2017 / 67
evidence & practice / CPD / cardiology
KEY POINT The administration of oxygen should be STEMI is restoration of blood supply to
The crucial factor that avoided in patients with suspected acute the myocardium. This may be achieved by
determines the success coronary syndrome where their oxygen either surgical intervention or
of percutaneous coronary saturation is greater than 94%, or 88-92% pharmacological means. In the UK, surgical
intervention is the time for patients with COPD with a risk of intervention in the form of percutaneous
from vessel occlusion hypercapnic respiratory failure (NICE 2016). coronary intervention is preferred (Figure 6)
to treatment. Guidelines The administration of supplemental oxygen (NICE 2016). The patient can be taken
recommend undertaking may cause vasoconstriction. In patients with from the pre-hospital setting directly to the
percutaneous coronary acute coronary syndrome, this could result in cardiac catheterisation laboratory for this
intervention as soon as further occlusion of affected coronary vessels procedure to be undertaken, where
possible following diagnosis (Stub et al 2015). Where oxygen saturation possible, which will minimise delays to
(Nikolaou et al 2015, Roffi et falls below 94%, supplemental oxygen treatment (Nikolaou et al 2015).
al 2016). Alongside clinical should be administered with a target range as Percutaneous coronary intervention
considerations, the nurse previously described. involves inserting a catheter through
should ensure the emotional the arterial system, usually through the
and psychological needs of Medical management radial artery (Timmis 2015). The catheter
the patient are attended to The nurse should always presume the patient is inserted under X-ray guidance to the
is experiencing a life-threatening condition coronary vessels. Once in the coronary
until proven otherwise. Nurses should also be vessels, the affected vessel or vessels are
aware of technological or pharmacological identified. The clinician will then inflate
developments in emergency care, because the catheter balloon, compressing the
recommendations about investigations and thrombus. A stent is then inserted to
subsequent treatments change frequently. maintain patency of the vessel (Figure 6).
The medical management of the patient The crucial factor that determines
will depend on the definitive diagnosis the the success of percutaneous coronary
clinician reaches; whether this is unstable intervention is the time from vessel
angina, STEMI or NSTEMI. occlusion to treatment. Guidelines
recommend undertaking percutaneous
ST elevation myocardial infarction coronary intervention as soon as possible
In the case of STEMI, clear evidence of ST following diagnosis (Nikolaou et al 2015,
segment elevation on an ECG and a Roffi et al 2016). Alongside clinical
supporting history or blood test results considerations, the nurse should ensure the
make diagnosis relatively straightforward emotional and psychological needs of the
(Box 1). The definitive treatment for patient are attended to.
Figure 5. ST elevation on a 12-lead electrocardiogram
I aVR V1 V4
II aVL V2 V5
III aVF V3 V6
II
68 / 15 March 2017 / volume 31 number 29 nursingstandard.com
For related CPD articles visit
evidenceandpractice.nursingstandard.com
TIME OUT 6 Blood tests, specifically troponin levels, will KEY POINT
Refer to the patient information for Mark in Time out 4, be within the normal range. The symptoms associated
and answer the following questions: In NSTEMI, signs may be identical to with unstable angina
» What are your nursing management priorities? unstable angina and STEMI. There may include chest pain lasting
» If Mark was found to have ST segment elevation on
be evidence of ischaemia on an ECG. The longer than 15 minutes,
leads II, III and aVF of his 12-lead ECG, combined with crucial factor that may enable the clinician which may or may not be
raised troponin levels, what would the diagnosis be? to differentiate between NSTEMI and associated with exertion.
unstable angina is blood results. Troponin Signs include evidence
» What part of the heart is affected, based on the levels following NSTEMI typically increase of ischaemia to the
findings of the ECG?
or decrease (Thygesen et al 2012). myocardium on an ECG.
In addition to the interventions outlined Such changes include ST
Non-ST elevation myocardial infarction in the immediate management section in segment depression or
and unstable angina this article, treatment will be determined changes to T waves. Blood
The nature of acute coronary syndrome by the patient’s risk factors. These risk tests, specifically troponin
means that in the absence of the classic factors can be calculated by the clinician levels, will be within the
signs of STEMI, diagnosis is may be using the GRACE (Global Registry of normal range
challenging for clinicians. The symptoms Acute Coronary Events) risk score (Timmis
the patient will experience between the 2015). This is a web-based model that
three types of acute coronary syndrome indicates the risk of death within six
might be identical. Therefore, the clinician months of the cardiac event, taking into
must interpret the patient’s signs and account risk factors such as the patient’s
symptoms to reach a definitive diagnosis. age, the presence of heart failure and ST
The symptoms associated with unstable segment elevation (Fox et al 2006). Where
angina include chest pain lasting longer possible, patients should be investigated
than 15 minutes, which may or may not through angiography (Roffi et al 2016).
be associated with exertion. Signs include This investigation will confirm the
evidence of ischaemia to the myocardium existence and extent of any infarction and
on an ECG. Such changes include ST the extent of any myocardial damage.
segment depression or changes to T waves. There is evidence that intravenous
nitrates may be more effective in patients
Figure 6. Percutaneous coronary intervention with NSTEMI or unstable angina than
nitrates administered via the buccal or
oral route. Cotter et al (1998) found
intravenous nitrates were effective in
relieving chest pain and in some cases were
more effective in reversing ST segment
depression on an ECG, which is a sign of
Artery showing stent on uninflated balloon myocardial ischaemia. The administration
of nitrates has several benefits to the
ischaemic myocardium. Dilation of blood
vessels results in a lower volume of blood
returning to the right side of the heart
(preload). This reduces the workload
for the myocardium, thereby reducing
Artery showing stent on inflated balloon myocardial oxygen demand (Roffi et al
2016). It should be noted that the research
by Cotter et al (1998) is dated, and that
more recent additional research is required
to validate this evidence.
Conclusion
Acute coronary syndrome is a medical
Artery showing expanded stent in place
emergency that may be challenging for
nursingstandard.com volume 31 number 29 / 15 March 2017 / 69
evidence & practice / CPD / cardiology
the nurse. A structured approach to initial technology and/or pharmacology. However,
assessment, such as the ABCDE approach, one factor that will not change is that a
will ensure that life-threatening problems human being will be at the centre of the
are identified rapidly and important clinical process. Nurses are not simply technicians;
information is gathered. While in some cases they provide care, and an important aspect
the cause of the patient’s condition may be of nursing care involves demonstrating
obvious, such as in STEMI, in other cases, compassion, providing support and acting
patients will present with a variety of signs as an advocate for the patient during one
and symptoms. The nurse should always of the most vulnerable times in their life.
presume the patient is experiencing a life-
threatening condition until proven otherwise. TIME OUT 7
Knowledge of risk factors, ECG Nurses are encouraged to apply the four themes of
interpretation and local protocols will The Code (NMC 2015) to their professional practice. Consider
enable the nurse to make informed how knowledge of the assessment and management of
decisions when planning the patient’s care. acute coronary syndrome relates to the themes of The Code.
Research in emergency care means that
recommendations regarding investigations TIME OUT 8
and subsequent treatments change Now that you have completed the article you might like to
frequently, because of developments in write a reflective account as part of your revalidation.
References
Bhatnagar P, Wickramasinghe K, Williams observational study (GRACE). BMJ. 333, of the European Society of Cardiology and oxygen in ST-segment-elevation myocardial
J et al (2015) The epidemiology of 7578, 1091. Other Societies on Cardiovascular Disease infarction. Circulation. 131, 24, 2143-2150.
cardiovascular disease in the UK 2014. Heart. Prevention in Clinical Practice (constituted
101, 15, 1182-1189. Nable EG, Braunwald E (2012) A tale of by representatives of nine societies and by Thiele H, Ohman EM, Desch S et al (2015)
coronary artery disease and myocardial invited experts). European Heart Journal. 33, Management of cardiogenic shock.
Booth KA, O’Brien TE (2015) infarction. The New England Journal of 13, 1635-1701. European Heart Journal. 36, 20, 1223-1230.
Electrocardiography for Healthcare Medicine. 366, 1, 54-63.
Professionals. Fourth edition. McGraw-Hill Quinn T, Johnsen S, Gale CP et al (2014) Effects Thim T, Krarup NH, Grove EL et al (2012)
Education, New York NY. National Institute for Health and Care of prehospital 12-lead ECG on processes Initial assessment and treatment with the
Excellence (2013) Unstable Angina and of care and mortality in acute coronary airway, breathing, circulation, disability,
Chung SC, Gedeborg R, Nicholas O et al (2014) NSTEMI: Early Management. Clinical guideline syndrome: a linked cohort study from the exposure (ABCDE) approach. International
Acute myocardial infarction: a comparison No. 94. NICE, London. Myocardial Ischaemia National Audit Project. Journal of General Medicine. 5, 117-121.
of short-term survival in national outcome Heart. 100, 944-950.
registries in Sweden and the UK. The Lancet. National Institute for Health and Care Thygesen K, Alpert JS, Jaffe AS et al (2012)
383, 9925, 1305-1312. Excellence (2016) Assessment, Diagnosis and Roffi M, Patrono C, Collet JP et al (2016) ESC/ACCF/AHA/WHF expert consensus
Immediate Management of Acute Coronary 2015 ESC Guidelines for the management document: third universal definition of
Cotter G, Faibel H, Barash P et al (1998) High- Syndromes. pathways.nice.org.uk/pathways/ of acute coronary syndromes in patients myocardial infarction. Circulation. 126, 16,
dose nitrates in the immediate management chest-pain#path=view%3A/pathways/ presenting without persistent ST-segment 2020-2035.
of unstable angina: optimal dosage, route of chest-pain/assessment-and-immediate- elevation: Task Force for the Management
administration, and therapeutic goals. American management-of-suspected-acute-coronary- Timmis A (2015) Acute coronary syndromes.
of Acute Coronary Syndromes in Patients BMJ. 351, h5153.
Journal of Emergency Medicine. 16, 3, 219-224. syndrome.xml&content=view-index (Last Presenting without Persistent ST-Segment
accessed: 22 February 2017.) Elevation of the European Society of Tortora G, Derrickson B (2013) The
Cowie MR, Lacey L, Tabberer M (2005)
Heart failure after myocardial infarction: Nikolaou NI, Welsford M, Beygui F et al (2015) Cardiology (ESC). European Heart Journal. cardiovascular system – blood. In
a neglected problem? British Journal of Part 5: acute coronary syndromes. 2015 37, 3, 267-315. Essentials of Anatomy and Physiology.
Cardiology. 12, 3, 205-208. international consensus on cardiopulmonary Ninth edition. John Wiley & Sons,
Shah ASV, Griffiths M, Lee KK et al (2015) Singapore, 377-396.
resuscitation and emergency cardiovascular High sensitivity troponin and the under
Cullen L, Greenslade J, Menzies L et al (2016) care science with treatment recommendations.
Time to presentation and 12-month health diagnosis of myocardial infarction in Yeh RW, Sidney S, Chandra M et al (2010)
Resuscitation. 95, e121-e146. women: prospective cohort study. BMJ. Population trends in the incidence and
outcomes in patients presenting to the
emergency department with symptoms Nursing and Midwifery Council (2015) The 350, g7873. outcomes of acute myocardial infarction.
of possible acute coronary syndrome. Code: Professional Standards of Practice and The New England Journal of Medicine. 362,
Smolina K, Wright F, Rayner M et al (2012) 23, 2155-2165.
Emergency Medicine Journal. 33, 6, 390-395. Behaviour for Nurses and Midwives. NMC, Determinants of the decline in mortality
London. from acute myocardial infarction in England Zorzi A, Peruzza F, Stella F et al (2016)
Fox KA, Dabbous OH, Goldberg RJ et al
(2006) Prediction of risk of death and Perk J, De Backer G, Gohlke H et al (2012) between 2002 and 2010: linked national Life-threatening tachyarrhythmias in the
myocardial infarction in the six months European guidelines on cardiovascular database study. BMJ. 344, d8059. cardiology department: implications for
after presentation with acute coronary disease prevention in clinical practice appropriate prescription of telemetry
Stub D, Smith K, Bernard S et al (2015) Air versus monitoring. Resuscitation. 101, 6-11.
syndrome: prospective multinational (version 2012). The Fifth Joint Task Force
70 / 15 March 2017 / volume 31 number 29 nursingstandard.com
evidence & practice / self-assessment questionnaire
Acute coronary syndrome
TEST YOUR KNOWLEDGE BY COMPLETING SELF-ASSESSMENT QUESTIONNAIRE 885
1. What is the most common cause of acute 7. Following the patient’s arrival in the clinical How to complete
coronary syndrome? setting, it is recommended that serial blood this assessment
a) Cardiac arrhythmia c tests are taken at:
a) 1, 2 and 3 hours This self-assessment
b) Hypertension c c
questionnaire will help you
c) Atherosclerosis c b) 0, 2 and 4 hours c
to test your knowledge.
d) Hypotension c c) 1, 4 and 8 hours c
It comprises ten multiple choice
d) 0, 3 and 6 hours c questions that are broadly
2. Which of the following is not a type of acute
linked to the article starting on
coronary syndrome? 8. What should be used to record the electrical
page 61. There is one correct
a) Unstable angina c activity in all planes of the heart?
answer to each question.
b) ST elevation myocardial infarction (STEMI) c a) 3-lead cardiac monitor c »» You can test your subject
c) Non-ST elevation myocardial infarction (NSTEMI) c b) 12-lead electrocardiogram c knowledge by attempting
d) Tachycardia c c) Angiogram c the questions before reading
d) Magnetic resonance imaging c the article, and then go
3. What is the difference between stable and back over them to see if you
unstable angina? 9. The preferred treatment to restore blood supply would answer any differently.
a) Chest pain usually resolves on rest within to the myocardium in a STEMI is: »» You might like to read the
15 minutes in stable angina c a) Glycerine trinitrate c article before trying the
b) Stable angina is caused by a widening of the b) Intravenous nitrates c questions. The correct
answers will be published
coronary arteries c c) Percutaneous coronary intervention c
in Nursing Standard on
c) Chest pain usually resolves on rest within d) Aspirin c
29 March.
15 minutes in unstable angina c
10. Which statement is true? Subscribers making use
d) The blood supply to the myocardium remains
adequate in stable angina c a) Diagnosis is easier for clinicians in the absence of their RCNi Portfolio can
of the classic signs of a STEMI c complete this and other
4. What does the D in ABCDE assessment stand for? b) The time from vessel occlusion to treatment is questionnaires online and save
a) Disease c the crucial factor that determines the success of the result automatically.
b) Diagnosis c percutaneous coronary intervention c Alternatively, you can cut
out this page and add it to your
c) Deterioration c c) A single dose of aspirin 300mg reduces the
professional portfolio. Don't
d) Disability c benefits of reperfusion therapy c
forget to record the amount
d) Acute coronary syndrome is rarely of time taken to complete it.
5. How can clinicians differentiate between
life-threatening c
an NSTEMI and unstable angina? You may want to write
a) Troponin levels typically increase or decrease a reflective account based
in unstable angina c This self-assessment questionnaire was compiled by on what you have learned.
Alex Bainbridge Visit journals.rcni.com/r/
b) ST segment elevation occurs in an NSTEMI, reflective-account
but not in unstable angina c The answers to this questionnaire will be published on 29 March
c) Troponin levels typically increase or decrease The answers to SAQ 883 on implantable cardioverter
following an NSTEMI c defibrillators, which appeared in the 1 March issue, are:
d) Atheromatous plaque builds up in the coronary
1. b 2. d 3. b 4. c 5. d 6. b 7. b 8. a 9. d 10. a
vessels in unstable angina only c
6. Which of the following is a modifiable factor
for coronary heart disease?
a) Age c
b) Diet c
c) Genetic factors c
d) Ethnicity c
nursingstandard.com volume 31 number 29 / 15 March 2017 / 71
You might also like
- Reflective PracticeDocument6 pagesReflective PracticeBlessing N. Ikiseh (Bibieandrea)No ratings yet
- Tamara Case StudyDocument6 pagesTamara Case Studymike0% (1)
- Essay Example 1 - DementiaDocument7 pagesEssay Example 1 - DementiaMarzio FagioliNo ratings yet
- Cardiovascular Nursing Practice A Comprehensive Resource Manual and Study Guide For Clinical NursesDocument3 pagesCardiovascular Nursing Practice A Comprehensive Resource Manual and Study Guide For Clinical Nursesydtrgn0% (1)
- Comprehensive Nursing Assessment ToolDocument7 pagesComprehensive Nursing Assessment ToolRamesh KandagatlaNo ratings yet
- 200W SyllabusDocument9 pages200W SyllabusBaranigha CjNo ratings yet
- Improvement in Documentation of Intake and Output ChartDocument2 pagesImprovement in Documentation of Intake and Output ChartanurajoneNo ratings yet
- The New Doctor 09Document52 pagesThe New Doctor 09Almas JanjuaNo ratings yet
- S. Faubel and J. Topf 4 Volume RegulationDocument24 pagesS. Faubel and J. Topf 4 Volume RegulationJoel TopfNo ratings yet
- Interventional CardiologyDocument36 pagesInterventional CardiologyRufus RajNo ratings yet
- AMI Case ReportDocument19 pagesAMI Case ReportTimothy TanNo ratings yet
- Reumatoid ArthritisDocument19 pagesReumatoid Arthritishenning_mastereid166No ratings yet
- Compassion OutlineDocument12 pagesCompassion OutlineIan LagmanNo ratings yet
- Nursing As An Art Nursing As An Art Nursing As An Art Nursing As An ArtDocument14 pagesNursing As An Art Nursing As An Art Nursing As An Art Nursing As An Artraj100% (3)
- B.SC in Nursing Syllabus 2018 For Web PDFDocument100 pagesB.SC in Nursing Syllabus 2018 For Web PDFYolanda Nadya0% (1)
- Diagnosis and Differential Diagnosis of Rheumatoid Arthritis - UpToDateDocument20 pagesDiagnosis and Differential Diagnosis of Rheumatoid Arthritis - UpToDateDannyGutierrezNo ratings yet
- Diagnosis and Management of Acute Coronary - An Evidence Based UpdateDocument11 pagesDiagnosis and Management of Acute Coronary - An Evidence Based Updatedanny17phNo ratings yet
- The 6Cs of NursingDocument14 pagesThe 6Cs of Nursingsamuel wandetohNo ratings yet
- Non-Pharmacological Pain ManagementDocument19 pagesNon-Pharmacological Pain ManagementStill DollNo ratings yet
- Nursing Student Guide TantocksengDocument0 pagesNursing Student Guide TantocksengUmiaziente SuchiNo ratings yet
- Theory Inspired Practice For End-Of-life Cancer CareDocument8 pagesTheory Inspired Practice For End-Of-life Cancer CareFerdy LainsamputtyNo ratings yet
- Discuss The Signs and Symptoms Associated With Myocardial InfarctionDocument2 pagesDiscuss The Signs and Symptoms Associated With Myocardial InfarctionDebra YoungbloodNo ratings yet
- Reading Sub-Test - Question Paper: Part CDocument10 pagesReading Sub-Test - Question Paper: Part CSarah Jane PetalioNo ratings yet
- Introduction To Nursing EthicsDocument16 pagesIntroduction To Nursing EthicsGladz C CadaguitNo ratings yet
- Duty Week 2: Etiologic/Causative Factors: Increased Risk For Death From Other Causes IncludingDocument5 pagesDuty Week 2: Etiologic/Causative Factors: Increased Risk For Death From Other Causes IncludingMeryville JacildoNo ratings yet
- Breaking Bad NewsDocument4 pagesBreaking Bad NewsHussam KabakbjiNo ratings yet
- Evidence-Based Nursing Care of Patient With Acute Myocardial Infarction: Case ReportDocument7 pagesEvidence-Based Nursing Care of Patient With Acute Myocardial Infarction: Case ReportAhmed AlkhaqaniNo ratings yet
- Nursing Students' Perceptions of Caring For Dying People, After One Year in Nursing SchoolDocument5 pagesNursing Students' Perceptions of Caring For Dying People, After One Year in Nursing SchoolPariNo ratings yet
- Check - October - 2014 - Daibetes and ObesityDocument38 pagesCheck - October - 2014 - Daibetes and ObesityVahid INo ratings yet
- Nursing in 21st CenturyDocument41 pagesNursing in 21st CenturyCarissa De Luzuriaga-Balaria0% (2)
- Cardiovascular System: Presented byDocument76 pagesCardiovascular System: Presented bySoma Al-mutairiNo ratings yet
- Guide To Clerking 2014Document24 pagesGuide To Clerking 2014Ridhwan Amid100% (1)
- Course OutlineNUR 1113 - Professional Nursing 2011-12 Sem 1studentDocument4 pagesCourse OutlineNUR 1113 - Professional Nursing 2011-12 Sem 1studentNurul AiniNo ratings yet
- A. Ward Round IPS Example FINALDocument5 pagesA. Ward Round IPS Example FINALEzra Ledya Sevtiana SinagaNo ratings yet
- Doctor-Patient Relationship - Cultural Aspects and Other Issues - Adel Adly RaghebDocument10 pagesDoctor-Patient Relationship - Cultural Aspects and Other Issues - Adel Adly RaghebAdel Adly100% (1)
- Renal Disease and FailureDocument40 pagesRenal Disease and FailureAlice ChoiNo ratings yet
- IELTSFever Academic IELTS Reading Test 163 With Answers - IELTS FeverDocument14 pagesIELTSFever Academic IELTS Reading Test 163 With Answers - IELTS FeverKamalNo ratings yet
- Nursing DefinitionDocument30 pagesNursing Definitionaibuty100% (2)
- Predictive Validity of OSCEDocument8 pagesPredictive Validity of OSCEmagdy balahaNo ratings yet
- Nursing Practice Is Based and Provides The Foundation For Understanding Theory As One Type of Nursing KnowledgeDocument32 pagesNursing Practice Is Based and Provides The Foundation For Understanding Theory As One Type of Nursing Knowledgeyousuf pogiNo ratings yet
- 2019print Friendly Future Nurse ProficienciesDocument30 pages2019print Friendly Future Nurse ProficienciesStacyNo ratings yet
- Introduction To Nursing Research Part 1Document22 pagesIntroduction To Nursing Research Part 1Ciedelle Honey Lou DimaligNo ratings yet
- Ielts 1Document69 pagesIelts 1Ganga SharmaNo ratings yet
- NM1726 Yr 1 FACT Handbook F10 CohortDocument12 pagesNM1726 Yr 1 FACT Handbook F10 CohortDibora AlemayehuNo ratings yet
- Information For Candidates: Introducing IELTS To Test TakersDocument8 pagesInformation For Candidates: Introducing IELTS To Test TakersHimanshi GuptaNo ratings yet
- Clinical Scenario FinalDocument10 pagesClinical Scenario Finalapi-257865334No ratings yet
- CarperDocument2 pagesCarperGlenn SunnyNo ratings yet
- Elder AbuseDocument30 pagesElder AbuseLokhie CheelaNo ratings yet
- OET Official Blog NotesDocument12 pagesOET Official Blog NotesMehmet Şevki UyanıkNo ratings yet
- Nur 862 Clinical Competencies PortfolioDocument11 pagesNur 862 Clinical Competencies Portfolioapi-457407182No ratings yet
- Neurologic Emergencies 2 MergedDocument71 pagesNeurologic Emergencies 2 MergedDanica FrancoNo ratings yet
- Measurement of Knee Joint Range of Motion With A Digital Goniometer: A Reliability StudyDocument7 pagesMeasurement of Knee Joint Range of Motion With A Digital Goniometer: A Reliability StudyTripatdeep SinghNo ratings yet
- David's CPNE NotesDocument21 pagesDavid's CPNE Notesdbryant0101100% (14)
- Previous IB Exam Essay QuestionsDocument4 pagesPrevious IB Exam Essay Questionsloveis1020No ratings yet
- The British Institute For Learning Found ThatDocument9 pagesThe British Institute For Learning Found ThatnouriiNo ratings yet
- Course PacketDocument176 pagesCourse Packethgfree41392No ratings yet
- Article - Medical ErrorsDocument4 pagesArticle - Medical ErrorsDavid S. ChouNo ratings yet
- Nursing Code of EthicsDocument2 pagesNursing Code of EthicsClarissa HeatonNo ratings yet
- Effects of HypoxiaDocument6 pagesEffects of HypoxiaMaria TelloNo ratings yet
- Activation of T LymphocyteDocument33 pagesActivation of T LymphocyteBaraa SharifNo ratings yet
- SKRIPSI Ghina FLDocument127 pagesSKRIPSI Ghina FLRini AprianiNo ratings yet
- Ischemic Heart Disease I SlideDocument36 pagesIschemic Heart Disease I Slidenoramzar mdnoarNo ratings yet
- AmlodipineDocument9 pagesAmlodipineMA 09No ratings yet
- Circulatory System AssignmentDocument8 pagesCirculatory System AssignmentMonroe P ZosaNo ratings yet
- Vascutherm2: Download Information Sheet (PDF 2.3M)Document2 pagesVascutherm2: Download Information Sheet (PDF 2.3M)D_StubbyNo ratings yet
- DES Vs BMS Pres - BaimPostACC - MetaBMSDES - 0508Document8 pagesDES Vs BMS Pres - BaimPostACC - MetaBMSDES - 0508Furqan MirzaNo ratings yet
- Amphibian Circulation - The FrogDocument15 pagesAmphibian Circulation - The FrogaraneyaNo ratings yet
- Echo Protocol GuideDocument29 pagesEcho Protocol Guideapi-722001988No ratings yet
- White and Red Pulp (Spleen)Document4 pagesWhite and Red Pulp (Spleen)Noreen BañagadoNo ratings yet
- Pulmonary Artery Dissection in Eight DogsDocument13 pagesPulmonary Artery Dissection in Eight DogsYoga RivaldiNo ratings yet
- Cardiac TamponadeDocument2 pagesCardiac TamponadekathzheinNo ratings yet
- Difficult Weaning From Cardiopulmonary Bypass Final Edit LiaDocument41 pagesDifficult Weaning From Cardiopulmonary Bypass Final Edit LiaYuri SadewoNo ratings yet
- Cardiovascular System: The Heart: Chapter 19 - Lecture NotesDocument73 pagesCardiovascular System: The Heart: Chapter 19 - Lecture Noteshersheys72002No ratings yet
- Shock and Its Nursing InterventionsDocument3 pagesShock and Its Nursing InterventionsWendy EscalanteNo ratings yet
- Introduction - MIDocument10 pagesIntroduction - MIkhimiiiNo ratings yet
- Atherosclerotic Cardiovascular DiseaseDocument68 pagesAtherosclerotic Cardiovascular DiseaseMarisa Adytia Adha100% (1)
- NNS Tutorial NotesDocument7 pagesNNS Tutorial NotesGio AmadorNo ratings yet
- PeripheralVascularDisease NotesDocument6 pagesPeripheralVascularDisease NotesNoah PontinoNo ratings yet
- Health Assessment - Cardiac & PVSDocument56 pagesHealth Assessment - Cardiac & PVSclaire3230No ratings yet
- Pathophysiology (Cerebrovascular Accident Hemorrhagic Right Lobe)Document4 pagesPathophysiology (Cerebrovascular Accident Hemorrhagic Right Lobe)jhonkivenNo ratings yet
- Lymphatic System Part 1Document33 pagesLymphatic System Part 1NaveelaNo ratings yet
- Physical Assessment Part 3 Assignment - SuzukiDocument21 pagesPhysical Assessment Part 3 Assignment - SuzukiNANAMI BOLIGOR SUZUKINo ratings yet
- Lecture 10Document5 pagesLecture 10bibifamelaganieNo ratings yet
- Final patho-HCVDDocument2 pagesFinal patho-HCVDAlvin RamirezNo ratings yet
- 4 5780579467025976939Document843 pages4 5780579467025976939osama hosniNo ratings yet
- Hypoplastic Left Heart SyndromeDocument13 pagesHypoplastic Left Heart SyndromeYaser AlmafrajiNo ratings yet
- Cody Michel's Blood PressureDocument4 pagesCody Michel's Blood PressureAnonymous G3r8ckbkqhNo ratings yet