Download as pdf or txt
You might also like
- Opthalmlogy MCQsDocument19 pagesOpthalmlogy MCQssimi y100% (2)
- Mitomycin C For Pterygium: Long Term Evaluation: Extended ReportDocument4 pagesMitomycin C For Pterygium: Long Term Evaluation: Extended ReportmegaparamitaNo ratings yet
- Mitomycin C-Associated Scleral Stromalysis AfterDocument4 pagesMitomycin C-Associated Scleral Stromalysis AftersrihandayaniakbarNo ratings yet
- tmpC47C TMPDocument4 pagestmpC47C TMPFrontiersNo ratings yet
- Transplantation of Conjunctival Limbal Autograft and Amniotic Membrane Vs Mitomycin C and Amniotic Membrane in Treatment of Recurrent PterygiumDocument6 pagesTransplantation of Conjunctival Limbal Autograft and Amniotic Membrane Vs Mitomycin C and Amniotic Membrane in Treatment of Recurrent PterygiumFrc 'Hario' FanachaNo ratings yet
- MMC in GlaucomaDocument6 pagesMMC in GlaucomaDayang SayalamNo ratings yet
- CLG PterygiumDocument3 pagesCLG PterygiumMichael HumiantoNo ratings yet
- CO 2767 Alpay 120108Document6 pagesCO 2767 Alpay 120108MaRia AnastasiaNo ratings yet
- Outcome of Recurrent Pterygium With Intraoperative 0.02% Mitomycin C and Free Flap Limbal Conjunctival AutograftDocument4 pagesOutcome of Recurrent Pterygium With Intraoperative 0.02% Mitomycin C and Free Flap Limbal Conjunctival AutograftPoppy PradinaNo ratings yet
- Cornea PDFDocument4 pagesCornea PDFHariadhii SalamNo ratings yet
- Translate Jurnal MataDocument5 pagesTranslate Jurnal MataferryNo ratings yet
- Comparison of Free Conjunctival Autograft Versus Amniotic Membrane Transplantation For Pterygium SurgeryDocument5 pagesComparison of Free Conjunctival Autograft Versus Amniotic Membrane Transplantation For Pterygium SurgeryTri Novita SariNo ratings yet
- Telaah Jurnal Rhizky Shasqia Putri NurDocument23 pagesTelaah Jurnal Rhizky Shasqia Putri NurrhizkyNo ratings yet
- Pterygium Excision With Free Conjunctival Limbal AutograftDocument7 pagesPterygium Excision With Free Conjunctival Limbal AutograftIOSRjournalNo ratings yet
- Conjunctival Autografting Combined With Low-Dose Mitomycin C For Prevention of Primary Pterygium RecurrenceDocument9 pagesConjunctival Autografting Combined With Low-Dose Mitomycin C For Prevention of Primary Pterygium RecurrenceNatalia LeeNo ratings yet
- Amniotic Membrane Transplantation For Primary Pterygium SurgeryDocument5 pagesAmniotic Membrane Transplantation For Primary Pterygium SurgerySa 'ng WijayaNo ratings yet
- Pterygium Management - Today: Medical ScienceDocument3 pagesPterygium Management - Today: Medical ScienceLiestiono NasiNo ratings yet
- Jurnal 4Document4 pagesJurnal 4tarietarooNo ratings yet
- Sutureless and Glue Free Conjunctivo-Limbal Autograft in Primary Pterygium Surgery - Outcome S and Recurrence RateDocument8 pagesSutureless and Glue Free Conjunctivo-Limbal Autograft in Primary Pterygium Surgery - Outcome S and Recurrence RateThomas KweeNo ratings yet
- Journal EyeDocument5 pagesJournal Eyehariwangsa23No ratings yet
- JClinOphthalmolRes43143-3289519 090815Document6 pagesJClinOphthalmolRes43143-3289519 090815Wielda MutafadhilahNo ratings yet
- Comparison of Recurrence of Pterygium Following Excision by Bare Sclera Technique With and Without Mitomycin CDocument80 pagesComparison of Recurrence of Pterygium Following Excision by Bare Sclera Technique With and Without Mitomycin CShoaib AbbasNo ratings yet
- 69 EdDocument10 pages69 EdAnna ListianaNo ratings yet
- Pterygium PDFDocument5 pagesPterygium PDFAfrizal AdzNo ratings yet
- Journal PterygiumDocument15 pagesJournal Pterygiumbeechrissanty_807904No ratings yet
- 1 s2.0 S1319453417301418 MainDocument4 pages1 s2.0 S1319453417301418 MainEzra MargarethNo ratings yet
- Comparison of Hyperdry Amniotic Membrane Transplantation and Conjunctival Autografting For Primary PterygiumDocument6 pagesComparison of Hyperdry Amniotic Membrane Transplantation and Conjunctival Autografting For Primary PterygiumNazliah SyarbinNo ratings yet
- tmp607F TMPDocument5 pagestmp607F TMPFrontiersNo ratings yet
- Mitomycin C and Conjunctival Autograft PDFDocument5 pagesMitomycin C and Conjunctival Autograft PDFfauziahputri29No ratings yet
- Comparison of Hyperdry Amniotic Membrane Transplantation and Conjunctival Autografting For Primary PterygiumDocument6 pagesComparison of Hyperdry Amniotic Membrane Transplantation and Conjunctival Autografting For Primary PterygiumNazliah SyarbinNo ratings yet
- OJOph 2013101413373503Document6 pagesOJOph 2013101413373503LaburengkengNo ratings yet
- TVT Nihms335507 PDFDocument30 pagesTVT Nihms335507 PDFAhmed NahrawyNo ratings yet
- Granuloma PCLDocument5 pagesGranuloma PCLEmrys1987No ratings yet
- Usa, 2002Document8 pagesUsa, 2002Maha OmarNo ratings yet
- tmpC73A TMPDocument8 pagestmpC73A TMPFrontiersNo ratings yet
- PterigiumDocument6 pagesPterigiumNdha SolidarityNo ratings yet
- 015 7851Document6 pages015 7851dradnanahmad82No ratings yet
- Jurnal PterigiumDocument6 pagesJurnal PterigiumMonica Lauretta Sembiring IINo ratings yet
- Treatment of Primary Pterygium: Role of Limbal Stem Cells and Conjunctival Autograft TransplantationDocument4 pagesTreatment of Primary Pterygium: Role of Limbal Stem Cells and Conjunctival Autograft TransplantationdianamariniNo ratings yet
- Complication Rate in Preliminary Experience in Phacoemulsification Cataract SurgeryDocument5 pagesComplication Rate in Preliminary Experience in Phacoemulsification Cataract SurgeryimtiazbscNo ratings yet
- Opth 14 2087Document4 pagesOpth 14 2087Savitri IndrasariNo ratings yet
- Efficacy of Autologous Blood Clot in Primary Pterygium Surgery Compared With Suture Technique in A Tertiary Hospital of BangladeshDocument7 pagesEfficacy of Autologous Blood Clot in Primary Pterygium Surgery Compared With Suture Technique in A Tertiary Hospital of BangladeshBOHR International Journal of Current Research in Optometry and Ophthalmology (BIJCROO)No ratings yet
- YahyaDocument33 pagesYahyaيحيى آل صايغ الكريريNo ratings yet
- Out 3Document7 pagesOut 3Oldi Nelson PatadunganNo ratings yet
- Pterygium EmedicineDocument9 pagesPterygium EmedicineThomas SmithNo ratings yet
- Clinoidal MeningiomaDocument10 pagesClinoidal MeningiomaAyu Yoniko CimplukNo ratings yet
- Conjunctivolimbal Autograft Using A Fibrin Adhesive in Pterygium SurgeryDocument9 pagesConjunctivolimbal Autograft Using A Fibrin Adhesive in Pterygium SurgeryRifqi AthayaNo ratings yet
- Jurnal 2Document4 pagesJurnal 2tarietarooNo ratings yet
- iOCT Guided Simulated Subretinal InjectionsDocument8 pagesiOCT Guided Simulated Subretinal InjectionsxuedunNo ratings yet
- Intracameral Mydriatics Versus Topical Mydriatics in Pupil Dilation For Phacoemulsification Cataract SurgeryDocument5 pagesIntracameral Mydriatics Versus Topical Mydriatics in Pupil Dilation For Phacoemulsification Cataract SurgeryGlaucoma UnhasNo ratings yet
- Patients and MethodsDocument6 pagesPatients and Methodsapi-3770306No ratings yet
- Phacoemulsification Versus Manual Small Incision Cataract Surgery in Hard NuclearDocument6 pagesPhacoemulsification Versus Manual Small Incision Cataract Surgery in Hard NuclearRagni MishraNo ratings yet
- Size, Location and ShapeDocument7 pagesSize, Location and Shapehenok birukNo ratings yet
- Full Thickness Skin Grafts in Periocular Reconstructions: Long-Term OutcomesDocument4 pagesFull Thickness Skin Grafts in Periocular Reconstructions: Long-Term OutcomesdrelvNo ratings yet
- Dr. Ankur Kumar, Dr. Kishor KumarDocument4 pagesDr. Ankur Kumar, Dr. Kishor KumarValentina Gracia ReyNo ratings yet
- Closed-Chamber Techniques For Iridodialysis Repair BMC 2018Document6 pagesClosed-Chamber Techniques For Iridodialysis Repair BMC 2018Alexandre IshizakiNo ratings yet
- Evaluation of The Safety and Efficacy of Therapeutic Bandage Contact Lenses On Post-Cataract Surgery PatientsDocument7 pagesEvaluation of The Safety and Efficacy of Therapeutic Bandage Contact Lenses On Post-Cataract Surgery PatientsFitrian Hanif ZulkarnainNo ratings yet
- Selective Capsulotomies and Partial Capsulectomy inDocument8 pagesSelective Capsulotomies and Partial Capsulectomy inirdaNo ratings yet
- Jurnal Mata 5Document6 pagesJurnal Mata 5Dahru KinanggaNo ratings yet
- Surgical Management of Childhood Glaucoma: Clinical Considerations and TechniquesFrom EverandSurgical Management of Childhood Glaucoma: Clinical Considerations and TechniquesAlana L. GrajewskiNo ratings yet
- Stat Activity 1Document40 pagesStat Activity 1Gerald Jem BernandinoNo ratings yet
- What Is Colour Theory in FilmDocument7 pagesWhat Is Colour Theory in FilmGraphite Box StudioNo ratings yet
- Aerial PhotographyDocument45 pagesAerial Photographypavan hiranNo ratings yet
- General Practitioner - Ophthalmology MCQsDocument25 pagesGeneral Practitioner - Ophthalmology MCQsAsif Newaz100% (3)
- Close-Up and Macro PhotographyxDocument45 pagesClose-Up and Macro PhotographyxfragmenteNo ratings yet
- NO - IL - ' - ' - .J: Instructions To Candid - AtesDocument15 pagesNO - IL - ' - ' - .J: Instructions To Candid - AtesnivedhaNo ratings yet
- Assessment of Stereovision With Digital Testing in Adults and Children WithDocument14 pagesAssessment of Stereovision With Digital Testing in Adults and Children WithMiguel Angel Palacios BlazquezNo ratings yet
- Bathes MethodDocument7 pagesBathes MethodluisazcarateNo ratings yet
- Ejercicios Inglés RepasoDocument9 pagesEjercicios Inglés RepasoMorgannaLeFairNo ratings yet
- Computer Vision 8th Sem Lab ManualDocument29 pagesComputer Vision 8th Sem Lab ManualJaikishanNo ratings yet
- Contrast For CreativityDocument20 pagesContrast For CreativityAndrei Pitigoi100% (1)
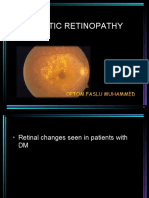
- Diabetic RetinopathyDocument44 pagesDiabetic RetinopathyGetLyricsNo ratings yet
- Berikut 350 + Kode Warna HTML - CSS LengkapDocument7 pagesBerikut 350 + Kode Warna HTML - CSS LengkapArs KassiuwNo ratings yet
- Sensation and Perception OrganizerDocument5 pagesSensation and Perception OrganizerBunnyNo ratings yet
- Underwater Image Enhancement For Improving The Visual Quality by CLAHE TechniqueDocument5 pagesUnderwater Image Enhancement For Improving The Visual Quality by CLAHE TechniqueijsretNo ratings yet
- Thesis Write UpDocument32 pagesThesis Write UpVishwas NayakNo ratings yet
- B04 Fastness To Light Summary Eng. Revized#3Document1 pageB04 Fastness To Light Summary Eng. Revized#3Timmi Timmi ChoiceNo ratings yet
- SofaScore Basic GuidelinesDocument7 pagesSofaScore Basic Guidelinesjijisi2861No ratings yet
- Solvent-Based Acrylic Paint Net:10 To Thin: Mr. Color ThinnerDocument20 pagesSolvent-Based Acrylic Paint Net:10 To Thin: Mr. Color Thinnercello Foryou100% (1)
- 2.3 Dynamic HTML Filters and Transitions CH - 15Document61 pages2.3 Dynamic HTML Filters and Transitions CH - 15Selva Ganesh100% (1)
- Spot Lights: NSP-001-1W NSP-002-3WDocument12 pagesSpot Lights: NSP-001-1W NSP-002-3WswaroopNo ratings yet
- Ophthalmology III Slit Lamp PDFDocument38 pagesOphthalmology III Slit Lamp PDFAgungNo ratings yet
- Care For Patients With Alteration in Perception and CoordinationDocument12 pagesCare For Patients With Alteration in Perception and Coordinationevlujtrep9690100% (1)
- ICT-2123-2012S Visual Graphic Design (NC II) P1: Week 11-20Document8 pagesICT-2123-2012S Visual Graphic Design (NC II) P1: Week 11-20Blah idkNo ratings yet
- How Digital Cameras WorkDocument17 pagesHow Digital Cameras WorkAnusha DandayNo ratings yet
- Police Photography Instructional MaterialDocument82 pagesPolice Photography Instructional MaterialEkaj Montealto MayoNo ratings yet
- JVT IiiDocument4 pagesJVT Iiimugammad wasimNo ratings yet
- Lecture 3 EdgeDetectionDocument52 pagesLecture 3 EdgeDetectionvimalfuNo ratings yet
- CSE Artificial EyeDocument15 pagesCSE Artificial Eyemounica saiNo ratings yet